 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
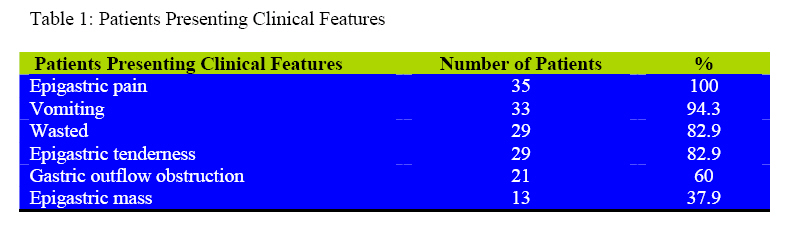
East and Central African Journal of Surgery, Vol. 14, No. 1, March-April 2009, pp. 130-134 Gastric Cancers At Kibogora Hospital G. Ntakiyiruta Kigali University Teaching hospital, Rwanda Email georgentakiyiruta@yahoo.co.uk Code Number: js09024 Background: Epigastric pain is very common in our patients of both sexes and upper GI endoscopy is offered in very few hospitals. Antacids are routinely prescribed countrywide. Helicobacter pylori is very common in our region. Not only most clinicians lack the means to diagnose this infection, but they also cannot confirm its eradication. Many of our patients present with advanced gastric cancer with no prospective for cure. The aim of this study was to determine the frequency, the clinical presentations, the anatomical and pathological aspects and the management of gastric cancers at Kibogora hospital. Introduction Gastric cancers are an important cause of cancer death worldwide1. For not very well understood reasons, gastric cancer is endemic in the region comprising Rwanda, Burundi, South Western Uganda and eastern Kivu province of DRC 2. This region is also being called the stomach cancer region. Lack of trace minerals in the volcanic soils has been advocated as a likely risk factor 2, 3 . The link between H. pylori and the non cardia gastric cancer is now well established 4,5,6. There is a long process from H. pylori chronic gastritis to gastric atrophy, intestinal metaplasia, dysplasia and cancer. Together with other still not well known risk factors, this process occurs in populations dwelling in the stomach cancer region where it is believed there could be different genotypes of H. pylori with different virulence. Medical practitioners in developing countries are faced with a large number of people consulting with dyspeptic disorders. However very few hospitals in our region are equipped with upper GI endoscopy. Therefore the management of such disorders is based solely on clinical examination. There is no mean to diagnose H. pylori infection. It is not surprising that patients will eventually present with advanced gastric cancers when there is no hope for cure. Patients with chronic dyspeptic disorders seen at Kibogora hospital are fortunate in having upper GI endoscopy done and some of them are diagnosed with gastric cancers. Most of the tumours are advanced and unresectable. Palliative surgery is performed to relieve gastric obstruction and to alleviate pain. The aim of this study was to determine the frequency, the clinical presentations, the anatomical and pathological aspects and the management of gastric cancers at Kibogora hospital. Patients and Methods This study was a descriptive retrospective case-series of gastric cancer patients seen over a one year period from July 2006 to June 2007 at Kibogora hospital. The hospital is a missionary district hospital in the south of the western province of Rwanda. It is one of the rare district hospitals which offer upper GI endoscopy and surgical services at a specialized level. In that respect, patients with chronic dyspeptic disorders are being managed there. Data was collected from records of patients with diagnoses of gastric cancers. SPSS 11.5 for Windows was used for data entry and data analysis. Results Patients’ characteristics Forty one patients were operated on for gastrointestinal cancers during the study period. Five patients had colo-rectal cancers and one patient had a tumour in the proximal jejunum. The other thirty five patients were diagnosed with gastric cancer. The age ranged between 30 years and 80 years with a mean of 55.9 years. There were more females 20(57.1%) than males 15(42.9%). The mean age for males was 56.7 years and the mean age for females was 55.2 years. The difference between males and females was not statistically significant (p=0.663) On admission patients had the following features: epigastric pain 100 (100%), vomiting 33(94.3%), severe weight loss with wasting 29(82.9%), gastric outflow obstruction 21(60%), epigastric tenderness 29(82.9%), epigastric mass 13(37.1%). The diagnosis of gastric cancer was made at endoscopy in 29(82.9%). The antrum accommodated the majority (71.4%) of the tumours. The body of the stomach had 25.7% of the tumours on the lesser curvature. This means that 97.1% of the tumours were distal gastric cancers. Only 2.9% of the tumours were proximal cancers. TNM Staging The majority 27(77.1%) of the primary tumours were T3 (tumour was penetrating through the serosa without involving contiguous structures) Thirty three patients (94.3%) had N2 lymphatic involvement (>3cm of primary tumour) whereas two patients had N1 lymphatic involvement (within 3cm of primary tumour). Sixteen patients (45.7%) had no obvious distant metastases (M0) and 19 patients (54.3%) had distant metastases (M1). These had ascites and liver metastases. Operative management Palliative surgery was done for 34 (97.1%) patients. Unresectable gastric cancers were 71.4% of all tumours. 60% of all tumours were treated by anterior gastrojejunostomy. 28.6% of all tumours were resectable. Partial gastrectomies with either Bilroth I or Bilroth II repairs were performed depending on the individual conditions. Pathology and Outcome Twenty (57.1%) operative specimens were sent for pathology. All the tumours were gastric adenocarcinomas of the intestinal type. The hospital stay ranged between 7 and 32 days with a mean of 14days. Twenty seven (77.1%) patients had markedly improved quality of life and were discharged home. Seven patients (20%) were not improved. One patient died in hospital. Discussion The stomach is one of the leading sites of cancer 1. The results from this study show that gastric cancer outnumbers all other gastro intestinal tract cancers. Gastric cancer is the second most common cause of cancer-related death in the world 1. During the study period, gastric cancer represented 83% of the primary gastrointestinal cancers with gastric to colorectal cancer ratio of 7:1. In the developed world, colorectal cancer accounts for more than75% of primary GIT cancers1, 3 . The stomach has been found to be the most frequent site of cancer for both sexes in Mizoram (India), a region with high gastric cancer prevalence 7,9,10. In the western countries, the typical patient with gastric cancer is male (male-to female ratio 1.7:1) and the mean age of the patients is 72years1, 4. The incidence rate of gastric cancer is also on the decline. In this study there were more female than male patients. The difference was however not statistically significant. However the study population was small and this may be the reason to explain this finding. The mean age of the patients was 55.9 years. Compared to the mean age in western countries, the population in this study was relatively young. This should prompt our clinicians to be more vigilant in screening patients for gastric cancer Patients in the 4th decade of life whose epigastric pain persists despite medical treatment should be followed up carefully. It must be emphasized that H. pylori infection, the strongest risk factor for gastric cancer is acquired in early childhood. As its diagnosis is made difficult by the lack of diagnostic means, the majority of the patients will not have proper treatment before a long time. Early gastric cancer has no specific symptoms. This explains why gastric cancer continues to be diagnosed when it is already advanced4,8 . In Japan liberal endoscopic screening is routinely performed and early gastric cancer can be diagnosed and managed accordingly with very good results. Even in USA two thirds of gastric cancers are diagnosed at an advanced stage. Symptoms of abdominal pain, vomiting, unintended weight loss and loss of appetite are associated with advanced gastric cancer with poor prognosis4, 8 . As gastric cancer appears to occur at a younger age in our population as compared to western world, patients over 40 years with vague dyspeptic disorders or long history of epigastric pain should be recommended for oesophago-gastro-duodenoscopy. If any suspicious lesion is observed multifocal biopsies should be taken. Of course in order to achieve this there is a need to have endoscopy equipment available at least at all regional referral hospitals and to train more surgeons and physicians in endoscopy. In this study gastric cancer was distal in 97.1%. The tumour was in the antrum in 71.4% and on the lesser curve of the stomach in 25.7%. Strong evidence is established that distal gastric cancer is commonly associated with H. pylori infection but proximal gastric cancer is not. H. pylori is quite prevalent in our region5,6,11. It is one of the most common infections in humans with an estimated prevalence rate of 50% worldwide and 90% in developing countries where infection is rapidly acquired in childhood and will persist lifelong. Available pathology reports say that all the operative specimen were adenocarcinoma of the intestinal type according to the classification of Lauren12. Gastric cancer of the intestinal type is associated with H.pylori but the diffuse type is not. No gastric lymphoma was diagnosed in this study. Lymphoid follicle is thought to be child-specific immune response. Therefore when infection is acquired in adulthood as it commonly occurs in western world, the patient acquires child-like immune response. Whereas when the infection is from childhood, the body becomes adapted because of chronic infection and therefore the body does not elicit similar immune response2 . None of the surgical procedures was performed in order to cure the disease. Of course palliation is very important in such situation because it improves the quality of life of the patient and also of the family. The patient is allowed oral intake of food and also surgery allows alleviation of pain. From our experience most of those patients recover very well and they can resume their usual duties. They regain weight because they are able to eat well. Some may even think they are cured. These patients should be well counseled because their life expectancy is not long. Adjuvant chemotherapy reportedly improves survival12,13 . However, in Rwanda, just like in many developing countries, most patients cannot afford adjuvant chemotherapy and is hot readily available. Prevention is also an important aspect of gastric cancer management. The aetiology of gastric cancer is multifactorial but some risk factors are well documented and others are yet to be investigated especially in our region. Preventive measures should focus on those risk factors. Eradication measures for H. pylori should be planned and implemented. Preventive measures together with eradication regimen should be available at the community level. Eradication programs were implemented in various countries (Costa Rica, Iran) with good results. Gastric cancer used to be the leading cause of mortality in the USA five decades ago but it is now on the decline. Dietary habits can also be addressed in such a way everybody can access to a balanced diet 15 . This is of course an issue of social development in general. Refrigeration of food and vitamin C are considered protective. Risk factors for gastric cancer in our region also need being properly investigated in order to understand very well what dietary habits could be addressed. Conclusions and recommendations Gastric cancer is a real cause of morbidity and mortality in our region. Diagnosing early gastric cancer is still a challenge because of inadequate investigative means. The management of advanced disease is only palliative and we do not have access to adjuvant chemotherapy. Prevention can help us to reduce gastric cancer incidence in our region. Campaigns to eradicate H. pylori infection should be planned and implemented particularly among patients with symptomatic H Pylori infection. This will hopefully reduce gastric cancer rates in our region. References
© 2009 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js09024t1.jpg] |
| |||||||||

{kind=link}