 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 14, No. 2, July-Aug, 2009, pp. 2-8 Principles of Management of Open Fractures A.M. Buteera, J. Byimana Consultant
Orthopedic Surgeons, King Faisal and Kanombe Military Hospitals, Kigali, Rwanda. Code Number: js09026 Background: Open fractures are known orthopedic emergencies associated with risk of
infection and healing problems. They also present as part of the spectrum in
multiply injured patients in a third of cases. The cases of open fractures are
common in our environment because of motor vehicle and motorbike accidents,
falls from height and sometimes gun-shot wounds. They do carry significant
morbidity and subsequent disability, if not managed appropriately. The initial
management of Open fractures usually affects the ultimate outcome. A closer
look at principles of evaluation and management of open fractures is necessary
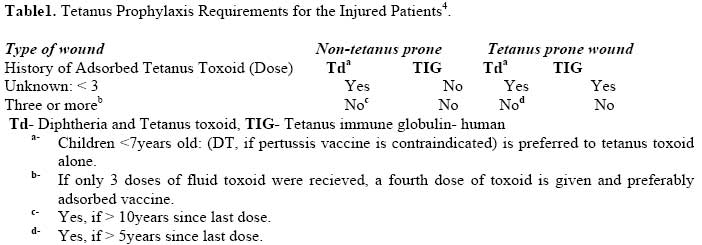
if they are to be managed appropriately. Introduction Open fractures are complex injuries of bone and soft tissue. They refer to osseous disruption in which a break in the skin and underlying soft tissue communicates directly with the fracture and its hematoma. They are orthopedic emergencies due to risk of infection secondary to contamination and compromised soft tissues and sometimes vascular supply and associated healing problems. Any wound occurring on the same limb should be suspected as result of open fracture until proven otherwise. The principles of management of open fracture are initial evaluation and exclusion of life threatening injuries, prevention of infection, healing of fracture and restoration of function to injured extremity. Initial Assessment Open fractures usually result from high energy trauma and occur in 1/3 of cases of multiply injured trauma. Injury dissipated to the soft tissues and bone is equivalent to the kinetic energy (KE=½mv2), where m is mass and v is velocity of the body. It is imperative to initially manage the patient in accordance with Advanced Trauma Life Support (ATLS) principles, exclude life threatening injuries of the head, chest, abdomen and Pelvis. Resuscitation immediately instituted as may be necessary and management of associated injuries according to their priorities. Co-morbidity factors like Diabetes mellitus, malnutrition, liver disease, peripheral vascular disease, extremes of age, immune deficiency syndromes, smoking and use of steroids are associated with delayed healing and should be taken into consideration early in management. The injured extremity is assessed for extent of wound, soft tissue injury and contamination. The neuro-vascular status of the limb is also assessed and noted and should exclude compartment syndrome1. Soft tissues are assessed for contamination, stripping, devascularization and degree loss as they affect method of fracture immobilization and infection risk. Soft tissue injuries are vital in management of fractures and Tscherne classified them into groups according to severity and initially for closed fractures and later as understanding of pathophysiology of soft tissue improved more sophisicated and detailed grading system were developed by Hannover fracture scale and AO soft tissue grading system which can be of use in severe open fractures2,3. Exploration of the wound in emergency rooms is not indicated, if operative intervention is planned to decrease risk of further contamination. After removal of obvious foreign bodies and acquiring trauma radiographs, wounds are covered with saline socked gauze. Appropriate antibiotic coverage and tetanus prophylaxis should be given. The current dosage of toxoid is 0.5ml regardless of age, and immune globulin is 75U for <5years, 125U for 5-10years, and 250U for >10years. They should be injected intramuscularly each from a different syringe and into different sites. Recommended Tetanus Prophylaxis is based on patient immunization history and type of wound whether tetanus prone or non tetanus prone. Non tetanus prone wound is a clean minor wound < 6hours after injury. Tetanus prone is one more than 6 hrs after injury, irregular configuration, > 1cm deep, from missile, crush, burn or frost bite. Below is a table for requirements of Tetanus Prophylaxis4. Provisional reduction and splinting also accomplished in emergency department to decrease further injury to fracture site while moving patient or extremity. Classification Any system of fracture classification helps in communication between clinicians and may aid in decisions of management and prognosis. The system of classification of open fractures into three types of increasing severity was first introduced by Veliskakis5.This concept was fully developed by Gustilo and Anderson6. It was subsequently modified by Gustilo et al7 and is the most commonly used classification and is shown below in Table 2. The above classification had an interobserver agreement of about 60% as shown by Brombark and Jones in a study of classification of tibial fractures by 245 orthopedic surgeons8. Because of this disagreement, it advisable to classify open fractures in operating theatre after extending the wound, assessing the contamination and state of the fractured bone and soft tissues. The risk of clinical infection as shown in a study by Patzakis and Wilkins is shown in the table below and depend on fracture characteristic and location9. The infection of tibia fractures is twice that of other locations. In cases involving severe crush injuries of limbs and Gustilo grade III, decision on further management is controversial. The key issue is to decide on limb salvage or amputation. The following should be considered; presence of nonviable limb, irreparable vascular injury, warm ischemic time > 8hours,severe crush with minimal remaining tissues, post salvage function less satisfactory than use of prosthesis, limb constituting threat to patients life and injury necessitating multiple operations and reconstructions which are not compatible with the will of the patient personally, socially and economically. To help in decision making whether limb salvage or amputation the mangled extremity severity score is used. A score of 7 or above had predictive of 100% for amputation10,11. Subsequent studies by Bosse et al did not prove this predictive value for this score and other four scores for lower limbs, this multicenter lower extremity assessment project ( LEAP) found that the most important factors were tibial fracture patterns, presence of open fractures, foot fractures, muscle injury, vein injury, arterial injury, and loss of planter sensation12. More recent studies did not prove loss of planter sensation as an important factor in deciding amputation as some patient regained sensation after reconstruction13. Whether a salvaged limb can be better than prosthesis is still controversial14. The decision for amputation should be taken carefully taking in consideration the MESS Score, The results of LEAP Study, the psychosocial aspects of the patient and available expertise. Antibiotic use Open fractures are contaminated, so antibiotic cover is inevitable. Use of antibiotics in the management in open fractures significantly reduces rate of infection6,7,8,9,10,15. Delay of greater than three hours increase rate of infection, and if given reduces infection by six-fold. It is advisable to give the initial dosage as soon as possible16, . There is still controversy in the duration of antibiotics given in open fractures. Current literature support duration of thee days15,16, to be repeated at times of wound closure, bone stabilization, or bone grafting. The recommended antibiotics in open fractures are cephalosporin alone for Gustilo type I, Cephalosporin and aminoglycoside for type II, and cephalosporin, Penecillin, and Aminoglycoside for type III injuries. The Antibiotics given should target the contaminating organisms. The most common organism infecting open fractures is Staphylococcus aureus and coagulase negative staphylococcus. Infections occurring in open fracture later in hospital are nosocomial and are mostly caused by gram negative. That commonly occurring in puncture wounds of the feet is Pseudomonas aerogenosa. Of concern are open fractures occurring on the farm or those with deep tissues without debridement as they are prone to Clostridial infections. Methicillin resistant staph.aureus (MRSA) has been isolated in patients as a community acquired and nosocomial and its appearance is associated with morbidity and mortality and increased treatment costs. It occurs commonly in institutionalized patients and intensive care units in outbreaks. Daptomycin has been approved for use against MRSA in Europe and America and its efficacy against MRSA osteomyelitis has been effectively been shown but they is scanty data on its treatment of orthopedic surgical infections in a randomized control study17. Lanezolid and Vancomycin are effective against MRSA and some old antibiotics like tetracycline, Rifampicin, clindamycin and Trimethoprim- sulphamethoxazole but culture and sensitivity patter should be respected. Ciprofloxacin and other quinolones should be used with caution in MRSA due to rapid resistance except if used in combination with other antibiotics17,18. Table 2. Classification of open fractures according to Gustilo et al
Table 3. Risk of Clinical Infection in Open Fractures by Patzakis and Wilkins
Table 4. Mangled Extremity Score (Adopted from Johansen et.al. 1990)
Recent studies advises addition of gram negative cover for grade I fractures. Aminogycoside should be used with caution in multiply injured patients whose renal function may be compromised. Ciprofloxacin replace aminoglycoside and has the advantage of oral use19. Use of local antibiotics bead construct utilizing antibiotic powder (amino glycoside) and polymethylmethacrylate (PMMA) cement reduce incidence of infection20. Tobramycin or gentamycin is commonly used. Debridement and Irrigation Debridement of open fractures is one of the single most important principles in management of open fractures. It was first described by Desault, and now involves generous lavage. It should be done meticulously and dissection should be sharp. All debris, devitalized tissue, loose cortical bone fragments should be removed. Dissection is continued to viable tissues edges identified by colour, consistency and contractility. Grade I and II wounds need to be extended to be able adequately debride them. The recommended time for debridement within 6 hours has for long been considered critical in prevention of infection. This 6 hour rule has been questioned by literature21. Knowledge of perforators and angiosomes is useful for proper placement of incisions. Before we have conclusive evidence against 6 hour time before debridement, debridement should be done as soon as possible if all requirements and expertise are available. Where necessary, a repeat debridement should be done within 24 to 48 hours. Irrigation is very important principle in open fracture management, but the method of delivery, optimal amount or irrigation solution still remain controversial. Some have proposed 3 litres for grade I wounds, 6 litres for grade II and 10 litres for Grade III injuries. Antibiotic solutions appear more effective than saline but literature support is lacking. Detergents (soap) help remove bacteria and in one study were similar in reducing risk of infection to antibiotics22. Antiseptics should be avoided as they are toxic to tissues. The pressure required remains controversial, high pressure improves removal of bacterial but damages soft tissues and bone. Low pressure like bulb syringe and suction is adequate23. No difference was noted between use water and saline in wound cleaning24. Most surgeons still use saline. Based on current evidence, normal saline should be used routinely, use of additives should be limited until we have enough supporting evidence, low pressure lavage is advocated, if high pressure is used it should be limited to 50psi25. Closure of wounds Most wounds in open fractures are closed with delayed primary closure. Surgical incisions performed during initial debridement can be closed primarily and original open fracture wound left open. Assisted wound closure using antibiotic bead pouch or vacuum assisted dressings are useful methods. Management of wounds in open fractures may necessitate early primary closure, split skin graft (SSG), fasciocuteneous flap, rotational muscle flap and free muscle flaps. Godina showed that wide early experienced debridement to clearly healthy tissues and early rotational or free muscle flap cover may be better in experienced hands than sequential debridement and delayed closure26. Early closure has shown to prevent nosocomial infections common with multiple repeated debridements with delayed closure. The aim should be to achieve closure in 72hours. Fracture stabilization Fracture stabilization may be temporary or definitive. Temporary fixation includes skeletal traction and sometimes external fixation. Definitive fixation includes external fixation, plate fixation and intramedullary nailing. Each of these procedures has advantages and disadvantages. Skeletal traction may be useful in pelvic fractures and temporarily in femoral fractures for very short time. External fixation is the mainstay of treatment in severe open fracture like IIIA and IIIB, and has the advantage of allowing easy access to management of soft tissues injuries and bone transport, and can be exchanged for an intramedullary nail27. For safe exchange there should be no pin tract infection and within fourteen days. The main problem of External fixator is pin tract infections, loosening and delayed or nonunion28. Plate and screw fixation has higher infection rates open fractures29. Plates reserved for selected periarticular fractures. The intramedullary nails are mostly used in open fractures of the femur, radius and ulna gun-shot wounds, and grade I open tibia fractures30. They are also exchanged for type II open tibial fractures. There has been controversy over using either reamed or undreamed nails. Reaming has the advantage of decreased time to healing, decreased rate of non union, and less screw breakage31. The superiority of unreamed nails in multiply injured patient have been shown as it decreases pulmonary complications and spares endosteal blood flow, well knowing that the soft tissue blood flow is already compromised31. At present in isolated fractures no consensus has been reached for or against reaming. Adjuncts to management Bone grafting of non union in open fractures do occur. There is the option of use of human recombinant Bone morphogenic protein (BMP) 2 in severe open fractures32, and prophylactic bone grafting. Conclusion The management of open fractures presents a challenge due to risk of infection, healing problems and subsequent morbidity. Antibiotics and Tetanus prophylaxis started as soon as possible. Adequate debridement and copious levage remains one of the cornerstones of management of open fractures. Early internal fixation and soft tissue closure is advocated and collaboration with plastic or micro-vascular surgeon early where necessary is advocated. Use of adjuncts to management like vacuum assisted closure, recombinant human bone morphogenic protein 2 may improve tissue and bone healing respectively. The treating surgeon has to adhere to the principles of open fracture management for optimal outcome, prevent complications and decrease hospital stay and costs. References
Copyright © 2009 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js09026t1.jpg] |
| |||||||||

{kind=link}