 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
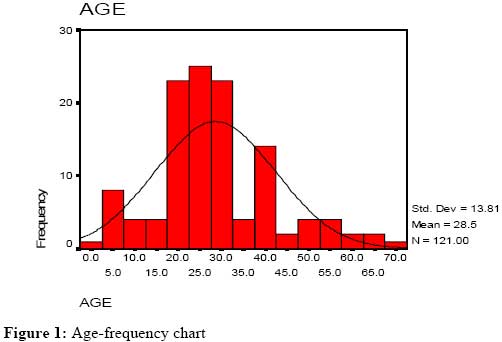
East and Central African Journal of Surgery, Vol. 14, No. 2, July-Aug, 2009, pp. 33-37 Boda-boda Injuries a Health Problem and a Burden of Disease in Uganda: a Tertiary Hospital Survey Galukande M, Jombwe J, Fualal J, Gakwaya A Department of Surgery, Mulago Hospital, Department of Surgery, Kampala, Uganda Correspondence to:Dr. Moses Galukande, Email: mosesg@img.co.ug Code Number: js09031 Background: Injury and deaths due to road traffic crashes are a major public health problem in developing countries. Boda bodas (motorcycles) are a practical and a sought after economic activity in Uganda’s capital and cities. The injuries related to boda bodas contribute significantly to the number road traffic injuries seen at Mulago hospitals, taking out significant resources including consumables and the health worker time. This study investigated the pattern of injuries, mortality and estimate cost of care. Methods: A prospective descriptive observational study over a 9 months period was carried out at Mulago Hospital and Complex, Accident and Emergency wards. The Study population was patients involved in Boda Boda related road traffic crushes. Consecutive patients presenting on every 3rd day were selected. Research Ethics committee approval was sought before the study was commenced. Results: A total of124 patients presented with injuries that warranted at least an overnight stay at the Accident and Emergency ward. Out of the just over 2000 admissions, the majority were males (sex ratio F: M 1:3.5) There was one fatality. Injuries were in 7 categories namely Head, chest, abdominal, pelvic, spinal and soft tissues and extremity fractures. Helmet use in this study was 22%, an improvement from previous nearly zero percent. The estimated cost of care per injured patient was USD 300. Conclusion: Boda Bodas continue to be a major cause or agent of road traffic injuries and a significant economic burden. The morbidity and mortality can be mitigated by encouraging use of protective gear like helmets and encouraging enforcement of traffic laws. Introduction Globally Road traffic injuries are a major cause of death and disability with a disproportionate number accruing in developing countries1,2. The problem is increasing at a fast rate in developing countries due to rapid motorization and other factors3. Public policy responses to this epidemic have been muted at national and international levels4. Boda Boda is a term that refers to both bicycles and small motorcycles with engine capacity of mostly 50-80cc. It is a term derived from the fact that they (boda bodas) plied routes involving borders of two countries, before this Ugandan innovation spread out to the rest of the country. Boda boda as a term is an alteration of the English ‘border border’. The phenomena’s small beginnings date back to the early 1960s5. The original services were provided on a man’s bicycle, equipped with a padded cushion fitted over the rear carrier, in the 1990s the bicycle based carriers were complemented by and completed with the light motorcycles that have greatly extended the range and load carriage of services6. They are a quick means of transport especially for short distances in cities and towns. They are efficient in mitigating traffic jam delays in the cities especially Kampala. They are available throughout the day and night hours. For tourists they are fun. They can be considered as variant of the Asia ‘tuk-tuk’. They are of great use in low-density demand areas or those where access is restricted by the width or quality of the route. Taxis do not find it profitable to go to many villages due to insufficient demand. Equally they physically cannot use the footpaths and tracks that provide access to many low-income urban settlements. It’s a source of livelihood for the operations and owners. It is estimated that over 100,000 Ugandans youths are involved in this business. The negative side of boda bodas as a means of transport is the risk of injury as highlighted in this and a study by Naddumba7. They are a health problem and contribute to the burden of disease. A health problem is a disease, injury or illness, or a risk factor for one of these. Burden of disease is a measure of the impact of a health problem. It includes the physical, emotional, social, and financial consequences as a result of the health problem. The number of boda bodas has increased over the years, regulation of its riders by way of licensing and punishing of traffic offences is at most poorly implemented. They are licensed to carry one passenger however it is not uncommon to see two or three passengers or cargo more than twice its size loaded on them. They maneuver through busy traffic at unbeatable speeds on pavements past pedestrians and sometimes through busy markets. They many times disregard traffic regulations as seen when they ride in wrong lanes and directions. For many passengers boda bodas are a necessary evil, they beat traffic jams, and are the cheapest means for those who cannot afford personal vehicles or cabs. Whereas the Naddumba7 study highlighted the Mulago hospital based prevalence and pattern of boda boda injuries, this study highlights prevalence, pattern, of injuries and the related health costs albeit estimates. Patients and Methods A prospective descriptive observational study was undertaken at at Mulago Hospital over a 9 months period. A total of124 patientswho sustained boda-boda injuries and were managed in the Accident and Emergency wards. The Study population was patients involved in Boda Boda related road traffic crushes. Consecutive patients presenting on every 3rd day were selected. Research Ethics committee approval was sought before the study was commenced Results The male to female sex ratio was 3.5:1 and the mean age 28.5 years and the median was 26 years. Figure 1 shows the age distribution. Helmet use was recorded in 22 (17.7%) against 98(79%) who admitted to not using protective headgear. Table 1. Patterns of Boda-boda Injuries.
Table 2. The Pattern of Fractures Caused by Boda-bodas
Table 3. Investigations Done.
Table 4. Road Traffic Related Injuries at Mulago Hospital 2004-2005
72% of fatalities were related to motorists, 26% to motorcyclists and 2% to bicycles There was one death of a 20 year old male multiply injured patient with brain contusion, cervical spine injury, a femoral fracture and double fracture of tibia & fibula. Fractures and soft tissue injuries were respectively sustained by 113 (80.1%) of all the admitted patients.. Table 1 shows the pattern of injuries sustained by the patients.More than 41% of the fractures involved the lower limbs. Close to 50% were extremity fractures (Table 2). Of the soft tissue injuries, 42.7% were bruises, 9.7% laceration and bruises. Forty three chest injuries were recorded. They were all blunt injuries, no penetrating injuries noted. Two had lung contusions and one had multiple rib fractures. Blunt bdominal injuries occurred in 29 (23.4%) of the patients. Splenic rupture occurred in one patient and the other 28 had blunt injuries without visceral rupture. Forty four (35.5%) patients had head injuries of which 43 were diagnosed as concussions and one has a brain contusion. Seven patients had spinal injuries, all cervical as anatomic site with one having injuries involving both cervical and lumbar spines. No paraplegics or quadriplegics were noted over the period investigated. No pelvic fractures were noted. Notably no DPL, no neuro-echos no MRI scans were done. No Urea and electrolytes, no random blood sugar or alcohol blood levels done. Two US Scans were done for the 124 patients of which 29 sustained blunt abdominal injuries. On average 20% of the patients had a full Haemogram done. The most requested for investigations were xrays, in total 249 x-rays were done, on average two radiograms per patient. We used the Mulago private wing billing guidelines, the cost of looking after these injured patients, investigating them, performing the indicated interventions approximate 490,000 Uganda shillings per patient. Discussion These injuries occurred in the urban area, were most Road traffic injuries occur in the developing countries8. The patterns of injuries included a soft tissue, chest, head, abdominal injuries and fractures. The largest proportion of individuals had Soft Tissue Injuries and fractures. The proportion of the multiple injuries was 20%. There was one case fatality among the 124 patients over the 9 months period and was multiply injury with head injury and limb fractures. The 2004 data indicated 28.6% of all road traffic injuries were motorcycle related with 14 fatalities (26%) of all fatalities. The injured are mostly young men (Ratio 1:3.5) in their most productive years. Fifty eight patients sustained fractures that would put them out of work for 10 to 30 weeks if no significant complications happen. Fractures contributed 80.6% and of these lower limb fractures contributed 45% like seen in other studies elsewhere The investigations done in these emergencies situations are mostly limited to basic plain x-rays an average of two body parts per patient who presented. Only 20% of patients had laboratory investigations done. The only round the clock available investigative modality is plain x-rays. Ultrasound scans are only available during that daytime and competed for by the outpatients /wards appointment patients, though efforts to introduce FAST (Focused Abdominal Sonography for Trauma), ultrasound for trauma in the accident and emergency department are underway. The majority of interventions were basic resuscitations with intravenous fluids administration. Analgesics, anti-tetanus prophylaxis and other surgical procedures such as surgical toilet with or without suturing and limb Splintage (Plaster of Paris applications) were used. The majority of these procedures were carried out by the surgical trainee with the tutorship of the appropriate specialist surgeons. The estimates use for these were adopted from the billing lists in the private outpatient wing. The costs on these lists are lower than the costs quoted in the ‘open market’ private facilities in Kampala. These costs are approximated. They exclude hidden costs to the patient and the family, which include buying medicines, commuter expenses, food and loss of revenue. The averaged out cost of 490,000/- Uganda shillings (USD 300) per injured patient is the salary of a registered nurse. Possibly this costs should be borne by the third party insurance cover that the boda boda operators take out. Among the challenges faced by institutions like Mulago hospital is to provide sufficient medical attention to the injured, but as highlighted by the inadequacy of the basic investigations done, this capacity can be improved and utilization of this insurance cover could be one way. Conclusion 1. The number of road traffic crushes and injuries is likely to continue increasing as the number of motorcycles and cars increase. 2. Poor enforcement of traffic safety regulations in low-income countries, inadequate resources, administrative problems and corruption continues to contribute to the burden of injuries. Other factors include education and state of our roads. 3. Policies on safety must be enforced to protected road users and the vulnerable productive young risk groups and reduce the stress on public health infrastructure and meager resources available for health care provision. This would include use of helmets, reflective jackets and riding with head lights on9. Alternative means of financing like the third party insurance could be explored some more to fund health institutions involved in care of the injured. References
Copyright © 2009 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js09031f1.jpg] [js09031t2.jpg] [js09031t4.jpg] [js09031t1.jpg] [js09031t3.jpg] |
| |||||||||

{kind=link}