 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
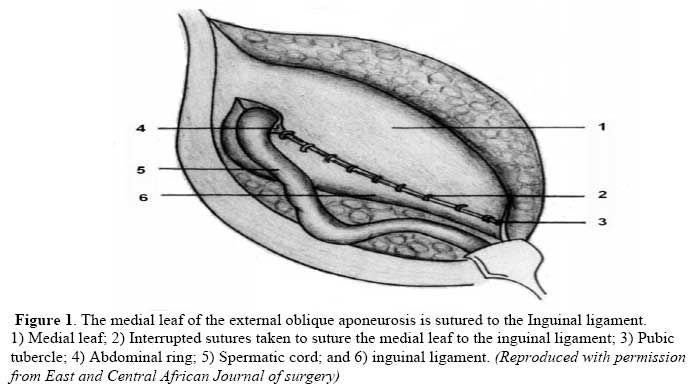
East and Central African Journal of Surgery, Vol. 14, No. 2, July-Aug, 2009, pp. 70-76 Comparison of Desarda versus Modified Bassini inguinal Hernia Repair: A Randomized controlled trial. S M Situma, S. Kaggwa, N.M. Masiira, S.K. Mutumba. Department of Surgery, Mulago Hospital, Kampala - Uganda. Correspondence to: Dr. S M Situma (email: smssituma@yahoo.com) Code Number: js09037 Background: Although the tension free inguinal hernia repair with a mesh is the standard technique in many developed countries, its use has remained low in the developing world due to the initial cost of the mesh. The most commonly used method in Mulago hospital is modified Bassini. The main aim of this study was to compare the short-term out come of Desarda’s versus modified Bassini inguinal hernia repair. Methods: One hundred and eight patients each with a unilateral, primary, reducible inguinal hernia were recruited through the surgical out patients department. Patients were randomly assigned to either the Desarda’s or Modified Bassini inguinal hernia repair. Postoperative pain was assessed using a visual analogue scale 1 to 2 hours after the operation, on the 3rd post operative day (POD) and again on the 7th POD. The gait was assessed on the 7th POD for all the patients and again on the 14th POD for those patients who had not attained their normal gait or had any postoperative wound complications on the 7th POD. Results: Of the 108 patients recruited, 88 (81%) were male and 20(19%) female. 3 patients were lost to follow up and 1 had an emergency laparotomy. The mean POD for resumption of normal gait was 3.62 for both methods. There was no statistically significant difference between the days of resumption of normal gait between the two methods (p-value = 0.94). There were no major complications using either of the two methods. There was no statistically significant difference between the two methods as regards the postoperative pain patterns 2 hours postoperative, on 3rd POD and on the 7th POD. Conclusion: There is no difference in short-term outcome between Desarda and modified Bassini inguinal hernia repair as regards resumption of normal gait and patterns of pain. Introduction Inguinal hernias by far are the most common types of hernias seen in most parts of Africa1.Inguinal hernia repair is one of the commonest operations done in Mulago hospital. The choice of a method depends on the surgeon; however, the ideal method for modern hernia surgery should be simple, cost effective, safe, tension free and permanent. The Lichtenstein operation to a great extent achieves all these goals2, 3.The Lichtenstein mesh, however has its shortcomings which include; its initial cost, non availability in many parts of the developing world, tendency to fold and wrinkle, movement that may lead to mesh failure, since the groin is a very mobile area and chronic groin sepsis, that requires mesh removal4. The predictors of medium term and long term outcomes are determined not only by the hernia characteristics, such as presence of a bulge at time of operation and the size of the defect, but also the short term post operative pain and the length of time taken to resume work or usual duties5. Desarda has described a new method that seems to satisfy the above criteria and does not require a prosthetic mesh and does not use weakened muscles or transversalis fascia for repair. It is cost effective with low rates of complications6, 7. The most commonly used method in Mulago Hospital is the Modified Bassini8 because it is easier to learn and cheaper in terms of initial costs. This study was undertaken to compare the short-term outcome of Modified Bassini repair and Desarda’s repair of inguinal hernias in Mulago Hospital. Patients and methods The study was conducted from December 2007 to March 2008 at Mulago Hospital, the teaching hospital for Makerere Medical School. The study design was a single blinded, single centered randomized controlled trial. A total of 108 patients with unilateral reducible inguinal or inguinal scrotal hernias, attending the general surgical out-patient clinics were randomly recruited into the study. They were randomly assigned either modified Bassini or Desarda’s repair. The operations were all done under local anesthesia via a regular oblique inguinal incision made about 1.5cm above and parallel to the medial two thirds of the inguinal ligament. The standard procedure of opening in layers and subsequent herniotomy was followed for all the patients. The difference only arose during repair of the defect. In Desarda’s repair, the medial leaf of the external oblique aponeurosis was sutured with the inguinal ligament from the pubic tubercle to the abdominal ring using polypropylene (Prolene) interrupted sutures (Figure 1). The first two sutures were taken in the anterior rectus sheath where it joins the external oblique aponeurosis. The last suture will be taken so as to narrow the abdominal ring sufficiently without constricting the spermatic cord. Each suture was passed first through the inguinal ligament, then the transversalis fascia, and then the external oblique. The index finger of the left hand was used to protect the femoral vessels and retract the cord structures laterally while taking lateral sutures. A
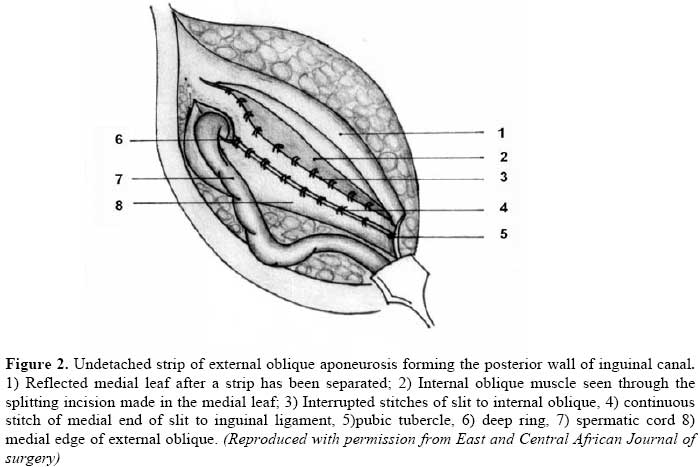
splitting incision was made in this sutured medial leaf, partially separating a
strip with a width equivalent to the gap between the muscle arch and the
inguinal ligament but not more than 2 cms. This splitting incision was then
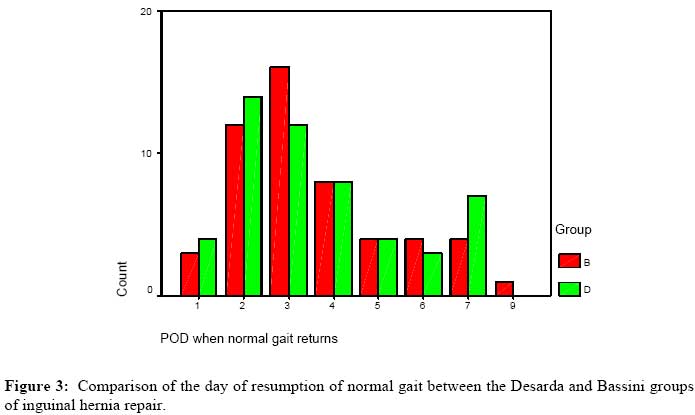
extended medially up to the pubic For modified Bassini repair, the cord and sac were drawn away, and then interrupted nylon 1/0 sutures were used to approximate the conjoint tendon and the internal oblique muscular edge to the shelving edge of the inguinal ligament. The first stitch was put in the periosteum over the pubic tubercle, care being taken not to injure the femoral vessels. The sutures were placed at intervals of approximately1cm between them and at different depths into the inguinal ligament. The most lateral stitch picked into the margins of the deep ring. The sutures were all put in place before being tied in reverse order of placement to minimize tension. The cord was then allowed to fall back on the strengthened posterior wall of the canal. The aponeurosis of external oblique was repaired with continuous nylon 2/0 and the superficial ring reconstructed to fit snugly around the cord. Each patient received intramuscular diclofenac at end of the operation and a course of oral diclofenac for five days. The first follow up was done 1 to 2 hours after the end of the operation, where pain was assessed using a VAS. The second pain assessment was done by the patient at home on the 3rd POD using a VAS similar to the one used for initial assessment. It was done in the morning before taking the medicines for that day. The third follow up was done on the 7th POD during which, pain and gait assessment was done. The gait assessment was done by asking the patient to tell the doctor on which day he was able to walk as he used to walk before the operation. The pain assessment was done again using a VAS similar to the one used in the initial assessment. Those who could not read or write would report back verbally. All pain assessment was done based on pain felt when walking. Those who had not attained their normal gait on the 7th POD were told to report back on the 14th POD to reassess the gait. Statistical analysis. Distribution of baseline characteristics was done using chi-square test. The day of return of normal gait and pain patterns was compared between the two arms using chi-square test. Pearson correlation coefficient and chi square test was used to determine the correlation of the VAS scores of the two groups on different days and its significance. Results A total of 108 patients were recruited and randomized, 55 were in the Bassini group and 53 in the Desarda group. Of the 55 who were in the Bassini group, 3 (5.5%) did not complete the follow up, while of the 53 enrolled for the Desarda group, 1 (2 %) did not complete follow up. The reasons for failure to complete were; 1 patient in Bassini group had a laparotomy before completion, so pain assessment was not done because he then had 2 wounds. The other 2 in Bassini and 1 in the Desarda group could not be accessed by the mobile telephone contacts recorded and yet they did not come back for review. The distribution of baseline characteristics was similar between the two groups as shown in Tables 1. Figure 3 shows the post operative day when patient resumed normal gait. All the patients had resumed their normal gait by the 10th POD. The mean POD for resumption of normal gait for the two groups was similar, 3.62. The range for the Desarda group was 6 days, (1 – 7), while that for the Bassini group was 8, (1 –9). The mode for the Bassini repair was 3rd POD and 2nd POD for Desarda repair. The difference between the days of resumption of normal gait between the two groups was not statistically significant, (χ2 = 0.33, P-value = 0.94). Assessment of pain. The mean pain score of the Desarda group was 4.84 as compared to Bassini group, which was 4.24. There was no statistically significant difference between the pain scores of the two groups in the first 2 hours after the operations. The mean pain score for the Desarda group on 3rd POD was 3.87 as compared to the Bassini of 3.58. There was no statistically significant difference between the pain scores in the two groups on the 3rd POD. The mean pain on the 7th POD was 2.27 and 2.23 for Bassini and Desarda respectively. The difference in pain scores between the 2 groups was not statistically significant. Table 1 Socio-demographic characteristic
Table 2. Comparison of Visual Analogue Pain Scores, 1 – 2 hours post operative, between the Desarda and Bassini Inguinal Hernia repair groups
Table 3. Comparison of Visual Analogue Pain Scores on the 3rd post operative day.
Table 4. Comparison of Visual Analogue Pain Scores on the 7th postoperative day.
Discussion In this study, the postoperative pain patterns and time taken to resume normal gait were similar for both groups. All patients had resumed normal gait by the 10th POD. The mode was also determined as the mean may be influenced by the extremes on both ends. The mode of the Bassini group was 3rd POD compared to 2nd POD of the Desarda group. The mean day in resumption of normal gait was similar to findings by Kyamanywa et al10 who compared the Lichtenstein mesh repair to modified Bassini. The similarity in day of resumption of normal gait between the two methods is because both these methods are tension methods. Desarda’s technique theoretically offers less tension, but during reconstruction of the inguinal canal, stitching of the new medial edge of external oblique muscle and its lateral edge, after repair of the defect, restores this tension that had been reduced by the slit. Other randomized studies have to be done to verify this. This may also explain the small difference in the mode between the two groups. Gait assessment, although less specific, is an activity done by the patient. Other studies that have used activities like bathing, dressing and walking around the house have shown that the majority of the patients could do all these activities by the 4th POD11. However all patients in this study were day cases and all walked out of the hospital, an estimated distance of about 100 meters. The first pain assessment was done 1 to 2 hours postoperative because all these operations were done under local anesthesia, 1% lignocaine chloride and therefore, these patients were fully conscious and alert. This was taken as a baseline measure of pain. The mean pain score for the Desarda group was 4.84 as compared to the Bassini group, which was 4.24. These were similar due to reasons already stated above, that these are both tension repairs. The mean pain score in both groups was higher than that observed in a multivariate analysis comparing several methods by Lau and Lee12. However, they used post incision infiltration of macain, which we did not do in this study. They also gave a combination of oral dextropropoxyphene 32.5mg and voltaren suppositories 50mg to each patient compared to only 75 mg of injectable diclofenac given to each patient in this study. Combination treatment is more effective than monotherapy in pain management; however it also increases the cost per patient. The next pain assessment was done on 3rd POD. The mean score for Desarda was slightly higher than that of Bassini. This pattern was similar to that observed two hours post operative. The similarity in the pain values is most likely because both these are tension methods, although Desarda theoretically offers less tension7,13. These however differ from those reported by Desarda, who reported that 96 percent of his patients reported mild pain in the first 4 days and none had severe pain7. However, he did not state the extent of mild as per VAS he used, dosages of drugs and time of pain assessment. His mode of assessment of the pain was not clearly stated. Other comparative studies have found the pain index to be highest with the Bassini repairs as compared to the others12. Our findings in this study imply that the Desarda technique offers similar tension to the Bassini if the amount of pain is equivalent to the tension in suture lines other factors being constant. The last pain assessment was done on the 7th POD when the patient had come for stitch removal. Again, the patterns were similar for both groups. The two patients who scored 9 and 10 in the respective group had wound sepsis, which caused a pressure effect due to pus formation on a closed wound, and hence significantly increased the pain. The analgesics had been stopped 2 days earlier on the 5th POD. There was no statistically significant difference between the postoperative score and the method used for herniorraphy on the 7th POD. This compares with Kyamanywa et al10 who found the mean pain for Bassini on the 7th POD to be 2.8. This is also in agreement with what Lau and Lee12 reported that that postoperative pain in herniorraphy was not affected by method used on the 7th and 14th POD. Using Pearsons’ correlation coefficient, there was no statistically significant correlation between the postoperative pain score and the operation group 2 hours post operative, on the 3rd POD and the 7th POD. This correlation decreases further from 2 hours postoperative to the 7th POD. These findings are in agreement with previous comparative studies 9, 10, 12. Conclusion There was no statistically significant
difference between the two groups as regards to day of resumption of normal
gait and the immediate post operative pain patterns in both Desarda and
modified Bassini inguinal hernia repairs. It is recommended that Desarda
inguinal repair be introduced in the training programmes in our region.
Copyright © 2009 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js09037t3.jpg] [js09037f3.jpg] [js09037t4.jpg] [js09037t1.jpg] [js09037f2.jpg] [js09037f1.jpg] [js09037t2.jpg] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}
{kind=link}
{kind=link}