 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
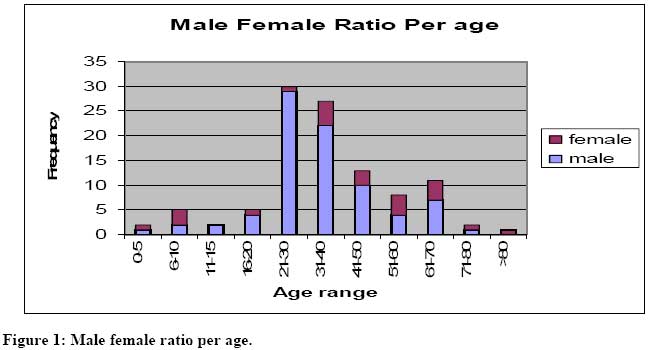
East and Central African Journal of Surgery, Vol. 14, No. 2, July-Aug, 2009, pp. 93-98 Epistaxis in Nigerians: A 3-year Experience J.A.E. Eziyi1, O.V. Akinpelu1, Y.B. Amusa1, A.K. Eziyi2 . 1Department of Surgery, Obafemi Awolowo University Teaching Hospitals Complex (O.A.U.T.H.C), Ile-Ife, Osun State, Nigeria. 2Department of Surgery, Ladoke Akintola University of Technology (LAUTECH) Teaching Hospitals Complex, Osogbo. Correspondence to: Dr (Mrs) JAE Eziyi, Email: eni_adeyemo@yahoo.com Code Number: js09041 Background:Epistaxis is a common symptom encountered in otolaryngological practice.This study was aimed at analyzing the aetiology, treatment and management outcome of the patients who presented with epistaxis at Obafemi Awolowo University Teaching Hospital, Ile – Ife, Nigeria. Methods: This is a prospective study of all consecutive patients that presented with epistaxis to our emergency rooms and ENT clinics from January 2003 to December 2005. Evaluation of patient included a detailed history taking and clinical examination. Control of epistaxis was obtained by treatment ranging from cauterization, anterior nasal packing to arterial ligation. Analysis was done using SPSS11. Results: A total of 106 patients who had on-going epistaxis were enrolled for the study. Eighty- two (77.4%) were male and 24 patients (22.6%) were female. Peak age incidence was in the age group 21- 40 (53.8%). Epistaxis was less common in the extremes of life. The most common aetiology was trauma (70.8%) Others included nasopharyngeal carcinoma, sinonasal carcinoma, sinusitis and allergic rhinitis. Majority of the patients (79.1%) were managed by nasal packing. All patients with atraumatic epistaxis (29.2%) had previous history of nasal bleeds. Blood transfusion was needed for 20 (18.9%) patients. The complication and mortality rates as a result of epistaxis were 1.9% (2 patients) and 0.9% (1 patient) respectively. Mean hospital stay was 5days + 2.68. Conclusion: Most epistaxis patient can be managed by a non-interventional method. Surgical Interventional treatment should only be used following failure of adequate non-interventional treatment. Complication rate was low. Introduction Epistaxis is a frequent otolaryngologic emergency1. It is a symptom of a large number of widely, diverse conditions. It has been reported that up to 60% of the general population will experience at least one episode of epistaxis in their life time, and 6% will seek medical attention for it1. Some authors portray epistaxis as a disease of the young2,3, whereas others have noted epistaxis to be more common in the elderly4 . The causes of epistaxis include both local and systemic factors such as trauma, tumours, infection, blood dyscrasias, ureamia, cardiovascular diseases, and allergic rhinitis 3, 5. However, the aetiology is idiopathic in majority of cases3. Epistaxis is broadly divided into anterior and posterior epistaxis. Most nasal bleeding is anterior, originating from a plexus of vessels in the anterior-inferior part of the septum (little’s area) and more frequently at an early age4. The less common but more severe posterior nose bleeding occurs frequently in the elderly with pre-existing artherosclerotic vessels or patients with bleeding disorders4. Varied modalities of treatment can be found in the literature1. The goal of treatment include: haemostasis, short hospital stay, low complication and cost effectiveness of the method of therapy1. Treatment modality is broadly divided into non-surgical (non-interventional / conservative) and surgical (interventional). The non- interventional therapy include anterior nasal packing, posterior nasal packing with catheters, balloons or packs, and local cauterization (chemical or electro-cautery). The surgical approaches include cryotherapy, submucosal septal resection, endoscopic cauterization, arterial ligation and endovascular embolisation of maxillary or ethmoidal arteries. The causes, management and outcome of patients who presented to our hospital with epistaxis were studied and analyzed. Patients and Methods A prospective study of all consecutive patients that presented with ongoing epistaxis via the ENT clinics, the accident and emergency units of a tertiary hospital and consultations for those that developed epistaxis while undergoing management for other diseases between January 2003 and December 2005 was conducted. Evaluation of patients included history taking- demographics, aetiological factors, past history of epistaxis, and detailed clinical examination - anterior rhinoscopy after decongestion with Adrenaline and rigid nasoendoscopy where indicated. Information on necessity of blood transfusion, treatment methods, duration of hospitalization and outcome of management of epistaxis were entered into a questionnaire and analyzed using SPSS11.0. Results A total of 106 patients were seen. Seventy one (67.0%) presented through the accident and emergency units and 35 (33.0%) presented in the ENT Clinics. Figure 1 shows the age distribution of patients with epistaxis. Their age ranges from 4 to 81 years with a mean age of 31.5 years, standard deviation of 12.3 years. Peak incidence was in the age group 21 – 40 (53.8%). Epistaxis in children accounted for 8.5% (9 patients) of the series (Table 1). There was a male preponderance. Eighty-two of 106 patients (77.4%) were male and 24 patients (22.6%) were female with a male to female ratio of 3.4: 1. Figure 1 shows the male female ratio per age. Table 2 shows the aetiological factors of epistaxis in this series. Twenty four patients (22.6%) had atraumatic, 75 patients (70.8%) had traumatic and 7 patients had idiopathic epistaxis. All patients with atraumatic epistaxis had previous episodes ranging from one to over 6 episodes with a mean of 3 episodes (+ 1.3 episodes). Non-traumatic epistaxis was more common in the paediatric age group (9 patients) with 6(66.7%) presenting with bleeding from the little’s area, 2(22.2%) had epistaxis secondary to allergic rhinitis, and 1(11.1%) had epistaxis secondary to nasal mass. Fifty percent (12 out of 24 patients) of epistaxis with atraumatic causes was due to malignancies, and these occurred equally in the middle aged and elderly with 80.0% of the sinonasal carcinoma occurring in the elderly and 71.4% of NPC occurring in the middle aged. Seventy six percent (57 patients) of traumatic causes of epistaxis occurred in the young adult and middle aged. Table 3 summarizes the treatment received. One hundred and four patients (98.1%) responded to non surgical treatment, anterior nasal packing for 48 – 72 hours with uniform vaseline gauze ribbon used in 51% of cases being the most common non surgical technique used, followed by cauterization with silver nitrate stick or solution in 20 patients (18.8%). Out of the twenty patients who were cauterized, seven patients (35%) had bleeding from the Little’s area; five patients (25%) had isolated nasal injuries and eight patients (40%) had maxillofacial injuries with local bleeding spots. Table 2: Aetiological Factors of Epistaxis
Table 3. Treatment Options Applied to Control Epistaxis
Table 4. Different Aetiologies of Patients that received blood transfusion.
Two patients (2.0%) with maxillofacial injuries had surgical method of control of epistaxis after failure of combined anterior and posterior packing. Hospital stay varied from 1 day to 10 days. Mean length of stay was 5 days + 2.68. Blood transfusion was required in 20 patients (18.8%). Table 4 shows the different aetiologies of patients that received blood transfusion.The unit of blood transfused ranged from one to four pints of fresh whole blood. Patients were transfused when their Packed cell Volume was 25% or less on presentation or during the course of management. Four patients had one pint of blood each while two to four units of blood (mean 2.2 pints) was delivered to 16 patients. Mortality was recorded in 0.9% (1 Patient) in a pre - irradiated nasopharyngeal carcinoma (NPC) who developed internal carotid artery bleeding. Complication of non surgical treatment such as partial synechiae occurred in two patients (1.9%). Discussion Epistaxis is a common symptom encountered in otolaryngological practice. In this survey, all age group were represented. Epistaxis was found to be more common in the young adult (54% in the 20-40 age groups) with a mean age of 31.5 years. This is contrary to findings by Pallin et al who found a bimodal age-related frequency with peaks among those younger than 10 years and aged 70-79 years4. The lower age incidence compared with some studies may have resulted from the fact that 70.8% of the cases had traumatic epistaxis and patients with traumatic epistaxis tended to be younger than those with atraumatic epistaxis4. Men were affected much more often than women by 3.4:1. This male preponderance has been documented in literature3,6,7. Majority of the patients had traumatic while 22.6% had atraumatic and 6.6% had idiopathic epistaxis. This corroborates the work done by Shahid et al8, and Saha et al9. The most common cause in literature is either idiopathic, hypertension or other atraumatic causes3,6,7 . Patients fell into 2 groups on the basis of treatment. This review demonstrated that 98.1% of patients were treated successfully by non interventional surgical treatment. The patients had either anterior, posterior nasal packing or combination of both for maximum of 3 days with satisfactory result. Head injury accounted for 38.7% (29 patients) of patients with traumatic epistaxis, they also had nasal packing because they presented with severe on-going bleeding. Nasal packing has the advantage of easy placement and removal; there was no need for an anaesthetist or theatre space for that treatment. It is also affordable to the patients. The complication in our series was synechiae in 1.9% of patients. The two patients presented with maxillofacial injuries and were packed once for 72hours. This complicationhas also been reported by Pallin et al4. Local chemical cauterization was also beneficial in 20 patients (18.9%). When bleeding comes from little’s area, coagulation with silver nitrate or diathermy is usually the only treatment needed. Five patients who had isolated nasal injuries and eight patients who had maxillofacial injuries with local bleeding spots also had coagulation as a form of treatment. Two patents (1.9%) had failed non surgical treatment. This failure rate is lower than that reported by Varshney et al, which ranged from 26-52%1. External ligation of anterior ethmoidal and external carotid arteries each was done in the 2 patients (1.9%). The risks of surgical treatment include the risk of anaesthesia, blindness, oro-antral fistula, ophthalmoplegia, cosmetic deformity, infra orbital nerve dysfunction. Two (1.9%) patients had surgical treatment to secure haemostasis and none of these complications was encountered. None of our patients had septal surgery because there was no indication for it. The mean hospital stay was 5 days. This correlate with reported mean hospital stay of between 4.67 and 5.6 days 7,10,11.Availability of nasal endoscopes which offers both proper visualization and direct facility for endoscopic cauterization to the area that is not easily accessible may have been able to further reduce the hospital stay and the discomfort of postnasal packing. The reported percentage of patients requiring blood transfusion for epistaxis ranges between 6.92 - 15.1% which is less than the 18.9% that required blood transfusion in our study 1,7,12 . This high rate of blood transfusion is probably due to severe acute blood loss from the trauma sustained. Mortality (0.9%) was in a nasopharyngeal carcinoma patient with rupture of the internal carotid artery. Rupture of the internal carotid artery has been reported in post- irradiated NPC patients6. Conclusion: In our study, the most common cause of epistaxis was trauma especially secondary to road traffic accident. The peak age incidence is in the third to fourth decade with epistaxis in children and the elderly accounting for 8.5%, 13.2% respectively. Nasal packing was the first line of management and found to be effective in 79.1% of the patients. Interventional treatment should only be used following failure of adequate non-interventional surgical treatment. Anterior nasal packing is still very effective and safe. Materials for it should be available at every emergency room of any hospital and all accident and emergency unit doctors should know how to put an anterior nasal pack in place. References
Copyright © 2009 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js09041t1.jpg] [js09041t4.jpg] [js09041t2.jpg] [js09041t3.jpg] [js09041f1.jpg] |
| |||||||||

{kind=link}