 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
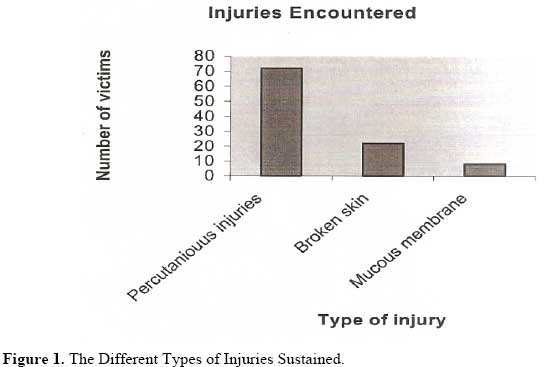
East and Central African Journal of Surgery, Vol. 14, No. 2, July-Aug, 2009, pp. 99-102 Knowledge, Attitude and Practices of Staffs towards Post-exposure Prophylaxis for HIV Infection at Mulago Hospital in Uganda R.Alenyo, J.Fualal, J.J Jombwe Department of Surgery, Mulago Hospital, Kampala – Uganda. Correspondence to:Rose Alenyo alenyom@yahoo.co.uk Code Number: js09042 The use of anti-human immunodeficiency virus (HIV) drugs after occupational exposure to HIV is a proven method of preventing some HIV infection and there is record that these drugs are being used in treatment of post exposure infection to HIV. This then raises the issues of the impact of such treatment on the staffs. The objective of the study was to asses the level of knowledge attitudes and practices of (PEP) against HIV among surgical staffs. 190 questionnaires were sent to staffs in the department of surgery but One twenty nine (68%) was returned. Questionnaires contained items related to awareness of occupational exposure to HIV and 0.77% had experience of its use in the department and 100% noted that there was no specific policy in relation to PEP in the Surgery Department at mulago Hospital. In relation to attitude staff believe strongly that PEP reduces risks to HIV infection but were also not willing to test for HIV after exposure. Introduction After initial reports in 1981, Sub-Saharan Africa now has the highest prevalence of Human Immunodeficiency Virus (HIV) infection in the world with profound social economic impact.1This has led to a heightened concern in the surgical community in terms of its impact on the practice of surgery and safety of the practitioners.2 This concern arises from the significant risk of infection through the parental route, lack of curative treatment, and the highest risk of exposure of surgical staff to the body fluids of patients. While most cases of infection in Africa are through heterosexual transmission, there is inadequate documentation of the incidence of occupational HIV infection among health care workers. It has been estimated that at least 1 in 500 surgeons is likely to be infected by HIV in the next 35 years an that a surgeons cumulative life risk of HIV sero conversion ranges from 1% to 10%1, 3.This risk arises from the frequent and intimate exposure to the patient’s body fluids through glove punctures, needles tick injuries, or ocular splashes and it is related to the prevalence of HIV infection in the community. In a study done in Nigeria, attitude and practices of Nigerian surgery trainees to HIV infected persons in 1997; it was found that non-availability of relevant devices remains the most important factor mitigating against the use of universal precautions. Studies from other parts of the world have addressed these issues, but due to differences in sero-prevalence, among other factors the results of studies conducted in one environment cannot be extrapolated to others 4, 5, 7. Previous studies in this environment have either focused on health workers generally or on categories of health. Subjects and Methods This was a cross-sectional study carried out 2006-2007.All surgical units were included in the study to demarcate boundaries of sampling frame. The number of surgical staff to be considered was determined by simple random sampling. All names of surgical staff were compiled and awarded numbers that were written each on pieces of paper put in a cup and churned thoroughly. These numbers then acted as cords. For collection of data structured questionnaire was used. The study population consisted of nurses, interns, orthopedic officers, and Surgeons. The parameters studied included; knowledge, and demographic characteristics of the study population such as age, sex of respondent, and occupation. Also looked at is attitude and practices of the study population on HIV prophylaxis. Results A total of 190 questionnaires were given out with only 129 (68%) were in position to return there responses in time. The majority (70%) of the respondants was females; males were only 30%. Married staffs accounted for 58.9% of the study population; 34.7% were singles. Table 1 shows the category of staff that responded to the questionnaire. More than half of the respondents were Nurses who totalled to 73(56.6%). Most of the respondents had practiced at the unit for more than a year and the longest duration of practicing at the unit was 35 years by one respondant. An overwhelming majority (95%) of the respondants had heard about post exposure prophylaxis for HIV but only 61% believed it was able to reduce the risk of HIV transmission. It was also noted that many were not sure when PEP is started following exposure to risky body fluids (Table 2). Although most of the respondants, had ever been exposed to potentially infectious materials which put them at high risk of contracting HIV, over 60% of the respondents noted that there was no provision for voluntary testing of the patients putting them at even higher risk of contracting HIV at their places of work. Figure 1 shows the nature of exposure reported. Table 1. Category of Respondants
Table 2. Responses to when to start PEP
Table 3. Respondants who have ever been exposed to potentially infectious materials
A significant number of respondant suffered from percutanious injuries but only 28% had ever sought advice on Post exposure prophylaxis. Failure to seek advice for PEP amidst the high rate of injuries sustained placed the respondents at a very high risk of contracting HIV/AIDS. A total of 49% of those who had ever been exposed to potentially infectious materials had ever had an HIV/AIDS test done on individual and private arrangement. Discussion Post Exposure prophylaxis is often given to individuals after exposure to high risk body fluids. The rate of transmission of HIV following percutanous exposure has been shown to be three per 1000 injuries and because there is no cure or effective vaccine for HIV infection, optimal post –exposure care, including administration of antiretroviral drugs to prevent HIV infection, remains a high priority for protecting health care personnel3, 10, 15. In our study only 20.2% reported that they have seen the guideline for Universal precautions for prevention of blood pathogens. Yet even though post exposure prophylaxis was really available an used its not 100% effective so prevention strategies through safer needle devices, and other innovations, remains the best way to prevent occupational infection by HIV and other blood borne pathogens. 8, 11, 12, In ideal situation PEP should be commenced preferably one hour after exposure however up to 2 weeks after exposure one may still start and will still be beneficial. In the study 48.1% had no idea when it should be started many gave varying time between 2 hours to one month with only 22.3% being sure it should be started within an hour of exposure. Timely post exposure prophylaxis to high risk body fluids is believed to reduce the risk of sero-conversion to HIV. The staffs showed a lot of reluctance to follow up the system set up for post exposure prophylaxis many once got exposed would either ignore or assume patient is safe or test the patient. Although 82.9% of the staff members had been exposed to potentially infectious fluids this was mostly after percutenious injury only 21% sought some sort of advice for PEP and did not follow it up. Most reason given was fear of being stigmatized and also most believed their fellow staffs would not buy the idea that it was from being exposed in the line of duty. What also came out is that the staffs do not wish to know their HIV status and also that the services were not readily available with no standard system set up to make it easy for one to go through the process. At the time of the study only one individual had ever taken PEP and did not accomplish the course because of the side effect of the drugs. Conclusion and Recommendation The staffs still have the fear of stigmatization and the fear of knowing their HIV status. Therefore all health care units should ensure that they have adequate staff counseling and education about risk of infection after exposure to high risk body fluids. And to ensure they have polices and procedures in place to ensure their staffs are aware of the actions to be taken if they are at risk of occupational exposure. Acknowledgements To all staffs in the Surgical Department, Mulago National Hospital who contributed to the study. References 1. Ministry of Health Antiretroviral treatment policy for Uganda. Draft 2003, 1:6-8 2. Patterson JM, Novac CB, McKinnon SE Patterson G: A surgeons concern and practices of protection against blood borne pathogens. 3. Lowenfels AB, Wormser GP, and Ramesh J: Frequency in puncture injuries in surgeons and estimated risk of HIV infection. Arch Surg 1989, 124:1284-1286. 4. Najem GR, Okuzu EI: International comparison of medical student’s perception of HIV and AIDS.J NatL Med Assoc 1998, 90:765-774.
Copyright © 2009 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js09042t2.jpg] [js09042f1.jpg] [js09042t3.jpg] [js09042t1.jpg] |
| |||||||||

{kind=link}