 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
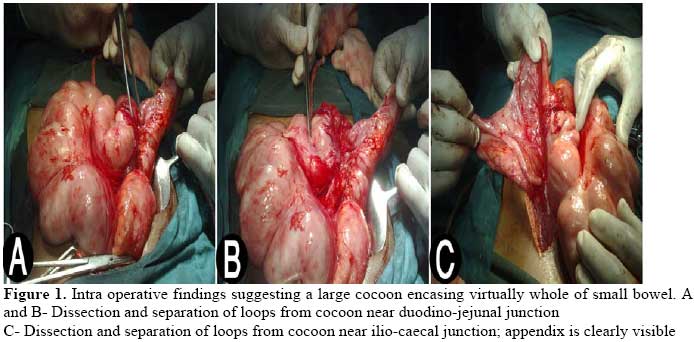
East and Central African Journal of Surgery, Vol. 14, No. 2, July-Aug, 2009, pp. 109-111 Tubercular Abdominal Cocoon in a Young Girl S. Dwivedi, P. Gharde, S.R.Johrapurkar, Sawangi, Wardha M.H., India Correspondence to: Dr. Sankalp Dwivedi, Associate Professor, Department of surgery Sawangi, Wardha M.H. India. E-Mail; sankalpdwivedi@yahoo.com Code Number: js09044 Tubercular abdominal cocoon, is a rare acquired condition in which small bowel is encapsulated by a thick fibro-collaginous membrane. The formation of a cocoon is probably due to sub-clinical peritonitis. Diagnosis is usually incidental and a "surprise" upon laparotomy1,10. Preoperative diagnosis is a challenge because biochemical investigations are usually normal, and imaging findings are nonspecific. CT scan gives a more complete picture and can clinch the diagnosis. We present a case of tubercular abdominal cocoon in a 16 years old young girl diagnosed only at laparotomy. The tubercular origin may be speculated here on the basis of her strongly positive TB ELISA for both IgG and IgM and raised ESR. Introduction Abdominal cocoon is a rare acquired condition in which an encapsulation of the small bowel by a fibrous membrane leads to small bowel obstruction. Diagnosis is usually incidental at laparotomy. It remains a clinical condition of obscure etiology and tuberculosis of abdomen (as in our case) is very infrequently reported in English literature as the cause of abdominal cocoon. Case Report A 16 years young female was admitted in the department of surgery with features of sub acute small bowel obstruction. She had a history of similar episodes during last 4 years, which were resolved with conservative treatment. Her routine blood and urine tests were normal except for raised ESR (65). X-Ray chest and sputum for AFB were also normal but TB ELISA was strongly positive for both IgM and IgG. Her pulse and temperature were within normal range. On per abdominal examination, diffuse mild tenderness and intermittent palpable loops of intestine (more prominent in left lower abdomen) were evident with otherwise normal abdomen. Pre-operative radiology including CXR abdomen, USG and even CT scan abdomen did not reveal any specific etiology. Figure 1During Barium enema, she went into retention and absolute constipation with features of acute obstruction. So decision of surgical exploration was taken. At emergency laparotomy, a thick whitish fibrous capsule, encasing virtually whole of small bowel loops, was revealed with the presence of inter loop adhesions. A diagnosis of abdominal cocoon was established and extensive adhesinolysis was performed. Histopathology of the biopsy taken from the fibrous capsule showed only fibrous tissue. The post operative period was uneventful. She has now been kept on anti tubercular therapy under the supervision of chest physician and doing well in follow-up. Discussion Abdominal cocoon is a rare condition that refers to total or partial encapsulation of the small bowel by a fibro-collagenous membrane/ cocoon1,2,10. Till date very few cases (<50) are mentioned in English literature. The condition has been described as ‘peritonitis chronica fibrosa encapsulata’ by Owtschinnikow in 1907 and sclerosing encapsulating peritonitis, (SEP) by Deeb et al in 19981,10. Patients are generally adolescent girls from tropical and subtropical countries5. Other organs like the large intestine, liver and stomach can also be involved within the fibro-collagenic cocoon3. The etiology is unknown and the disease is probably due to sub-clinical peritonitis or chemical peritonitis due to retrograde menstruation8. Although rare, secondary cocoon due to peritoneal tuberculosis and after continual ambulatory peritoneal dialysis has also been reported in English literature. In great majority, a high erythrocyte sedimentation rate and a positive Mantoux test were noted but no acid fast bacilli were found1. In present case also no confirmatory evidences like tubercular bacilli or granuloma at biopsy were found but TB ELISA (IgG & IgM) was strongly positive along with raised ESR. The basic patho-physiology of abdominal cocoon or SEP is an inflammatory process resulting in loss of the mesothelial layer of the peritoneum and fibro-connective tissue proliferation. Excessive fibrogenesis is thought to be due to Fibrin deposition and fibrinolysis and hyalinization of the superficial stromal collagen2,6,10. The recurrent episodes of severe peritonitis due to Pseudomonas aeruginosa and Staphylococcus aureus, could have been the trigger factors for the onset of post dialysis SEP7. Histopathology of the cocoon shows thick fibroco-llagenous tissue, with or without areas of lymphocyte and plasma cell infiltrates. Clinical presentation includes acute, subacute or chronic intestinal obstruction, abdominal distension, and weight loss secondary to kinking and/or compression of the intestines within the constricting cocoon1,10. A fluctuant abdominal mass may also be present due to an encapsulated cluster of dilated small bowel loops10. Preoperative diagnosis is a challenge because findings on biochemical investigations are usually normal, and imaging findings are nonspecific11. The diagnosis is usually made at laparotomy. Only rare attempts have been made and reported in literature of making preoperative diagnosis of this clinical curiosity known as abdominal cocoon. Conventional radiographs are nonspecific and show features of small bowel obstruction 2 6. On sonography, the small-bowel loops are encased in a thick membrane and arranged in a concertina shape with overall appearance of a cauliflower. The only differential diagnosis is an internal hernia3,5. Currently, abdominal CT scans are requested commonly by clinicians, because a CT scan most often can clinch the diagnosis and gives a more complete picture of this entity as well as any associated complications2. The characteristic findings of CT include that small bowel loops congregated to the center of the abdomen, encased by a soft-tissue density3,5, 6. Other CT features include signs of obstruction, agglutination and fixation of intestinal loops, mural thickening and ascites1. At times, the surrounding membrane may be thin and difficult to identify on a CT scan making it difficult to diagnose this condition preoperatively on imaging2. A barium meal and follow-through study also may help sometimes by showing a characteristic serpentine configuration of the dilated distal small bowel within a cocoon-like structure and delayed transit time with a normal mucosal pattern2,3,6. Various treatment options have been suggested. These include the use of immuno-suppression, corticosteroids with parenteral nutrition, tamoxifen and surgical debridement. Surgery is important in the management of AC. Careful dissection and excision of the thick sac with the release of the small intestine leads to complete recovery as was in our patient2. In addition, dense inter bowel adhesions also need to be freed for complete recovery. Resection of the bowel is indicated only if it is nonviable. Prognosis is usually good. Conclusion A tubercular abdominal cocoon, although rare, may be the cause of surgical emergency and it is difficult to make a definite pre-operative diagnosis. A high index of clinical suspicion with plausible etiologies combined with relevant imaging may help the clinicians to pursue a preoperative diagnosis, as it may prevent a "surprise" upon laparotomy and result in proper management. References
Copyright © 2009 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js09044f1.jpg] |
| |||||||||

{kind=link}