 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
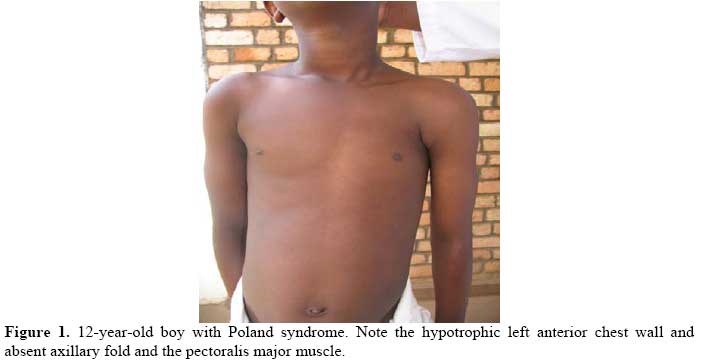
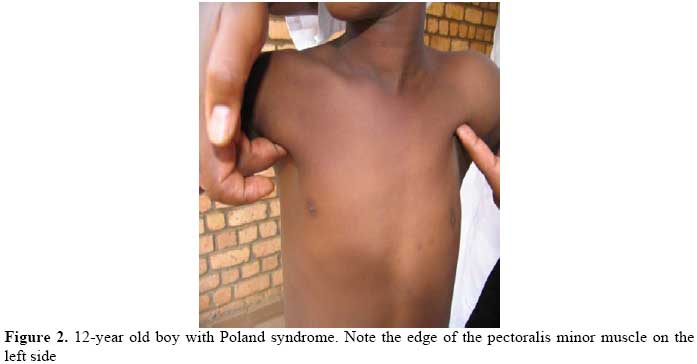
East and Central African Journal of Surgery, Vol. 14, No. 2, July-Aug, 2009, pp. 112-114 Poland’s Syndrome: A Case Report J. Gashegu1, J.C. Byiringiro2, M. Nyundo2, A. Uwineza3, L. Mutesa3 1Anatomy Laboratory, 2Surgery Department, 3centre for Medical genetics, Faculty of Medicine, National University of Rwanda. Correspondence to: Dr. Julien Gashegu, Email: jgashegu@nur.ac.rw Code Number: js09045 Poland’s Syndrome is a rare congenital condition. It is classically characterized by absence of unilateral chest wall muscles and sometimes ipsilateral symbrachydactyly (abnormally short and webbed fingers). The condition typically presents with unilateral absence of the sternal or breastbone portion of the pectoralis major muscle which may or may not be associated with the absence of nearby musculoskeletal structures. We report a 12-year-old boy patient with typical features of Poland syndrome. To the best of our knowledge, this is the first documented case of a patient with Poland syndrome reported from Rwanda. The Poland's anomaly was first described in 1841 by Sir Alfred Poland as a syndrome presenting with absence or underdevelopment of pectoralis major muscle, associated in some cases with a hypoplasia of the breast, an agenesis of 2,3,4 and 5 ipsilateral costal cartilage, an athelia, and an ipsilateral webbing of the fingers (cutaneous syndactyly)1,2. Therefore the Poland syndrome may occur with different gravity. Currently, it is assumed that Poland syndrome is characterized by a missing sternocostal bundle of the pectoralis major muscle3. Its incidence is difficult to determine, but current estimates range between 1:7,000 and 1: 100,000 births, with higher frequency among males (ratio, 2:1 – 3:1). In 75% of the cases, it is located on the right hemithorax in the unilateral form1,3,4,5,6. Affected individuals may have variable associated features, such as underdevelopment or absence of one nipple including the areola and/or patchy absence of hair in the axilla1,4. In females, there may be underdevelopment or aplasia of one breast and underlying (subcutaneous) tissues7. In some cases, associated skeletal abnormalities may also be present, such as underdevelopment or absence of upper ribs; elevation of the shoulder blade (Sprengel deformity); and/or shortening of the arm, with underdevelopment of the forearm bones (i.e., ulna and radius)1,4. A review of literature reveals that only two cases of Poland’s syndrome have been reported from Sub-Saharan Africa2,8. We present the first documented case from Rwanda. This paper is aimed at bringing awareness to health professional in the region of this rare congenital condition. Case report A 12-year-old, six-year-primary-school boy,first presented to us in 2005 with a flattening of the left anterior chest wall since the birth. He was the second child in a family of four. There was no familial history of similar disorder and specifically a coagulation disorders. Examination revealed an adolescent with normal growth parameters and good mental status. There were no unusual cranio-facial findings. His chest was asymmetric, with hypoplasia of the left side (Figure 1). He had a shapeless left shoulder, flattening of the left chest wall and absence of the left axillary fold. The pectoralis major muscle was absent but the pectoralis minor muscle as well as the anterior serratus muscle were present (Figure 2). The movements of the left shoulder were possible with the muscle power at abduction estimated at 4/5. He had normal heart sounds, and respiration and breath pattern were normal as well. The limbs were normal and symmetric, and ipsilateral fingers were found to be normal. Radiological examination of the chest showed no abnormalities of the ribs or heart. X-ray of bones of the ipsilateral upper limb did not showed any abnormality. Based on those physical findings, a diagnosis of Poland’s syndrome was made. No surgical treatment was offered. The family was counseled and the patient followed up on outpatient basis. During the last three year of follow up, the boy has bee found to continues to grow normally with good school progress Discussion The case of Poland Syndrome we present is the first described in Rwanda and is of the pure presentation as it consists only on the unilateral aplasia of the pectoralis major muscle without any other associated defects 1,3. However, it presented in the left hemithorax while the right side is the most frequently involved3,4. The exact etiology of the Poland syndrome is unknown. It is assumed that the aplasia of the pectoralis muscles and associated chest defects, as the athelia, aplasia of costal cartilages, are consequences of an interruption of early embryonic blood supply of subclavicular artery branches5,6. A combination of the blockage of various branches could lead to different manifestations of the Poland syndrome. It is known that thoracic wall is supplied by medial thoracic branches, intercostals artery, and the thoracic artery from axillary artery, the thoraco-acromial artery and the lateral thoracic artery. All these branches come from the subscapular artery or axillary artery. The interruption of the blood supply is caused by thrombus or embolus, which prevent the blood to reach the developing tissue. Another cause of blood supply interruption is the misdevelopment of vessels. However, there have been case reports of Poland syndrome associated with unusual defects, which can not be explained on the basis of compromised blood supply alone. On the other hand, Ferraro and colleagues3 described an unusual presentation of the Poland’s anomaly without any vascular alteration, raising the question as to the true pathogenesis of the Poland’s syndrome. Geneticists currently hold the view that Poland syndrome is rarely inherited and generally is a sporadic event. There are rare instances where more than one individual has been identified with Poland syndrome either in the immediate6,9,10 or extended family11,12,13. Therefore, some authors believe that an inherited abnormal vasculature formation may be the central underlying mechanism for this condition. Several reconstructive procedures are available to correct the functional and structural deformities associated with this syndrome. As forthe chest deformity, customized silicone prosthesis is simply and safely used. Transposition of the latissimus dorsi muscle for soft-tissue reconstruction has been used by many authors with satisfactory esthetic and functional results14. References
Copyright © 2009 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js09045f2.jpg] [js09045f1.jpg] |
| |||||||||

{kind=link}
{kind=link}