 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
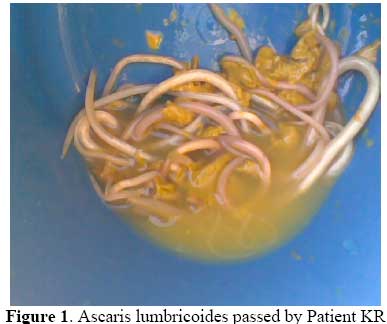
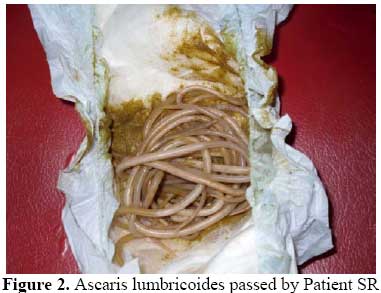
East and Central African Journal of Surgery, Vol. 14, No. 2, July-Aug, 2009, pp. 117-118 Code Number: js09047 Letters to the Editor . Dear Sir, RE: Laparotomy Due To Ascaris Lumbricoides at A.I.C Litein Mission Hospital – Kenya The above titled article by LugariaLD. published in East and Central African Journal of Surgery Volume 12 Number 2 November/December 2007 pages 105 -1091 makes an interesting reading. It is quite interesting that intestinal obstruction caused by Ascaris lumbricoides constituted the commonest indication for laparotomy in that hospital. This is not the situation in our hospital in Nigeria where typhoid intestinal perforation constituted the commonest indication for laparatomy in children aged 4years and above2. It seems from the study, that all the 69 patients with mechanical intestinal obstruction from Ascaris lumbricoides were managed by laparatomy1. This is very surprising because many of such patients can be managed successfully non operatively. Villamizer et a3l reported their experience with 87 children in Columbia. Sixty-four patients responded to medical treatment with nasogastric tube and racine oil (15 to 30 mL) and piperazine (75 mg/kg/d) for 5 days. Only twenty-three cases required surgery, because they did not respond to medical treatment or because of acute onset. In India, Mishra PK et al 4 reported one hundred and three patients with intestinal obstruction due to Ascaris lumbricoides treated over five years. All the patients were managed as for acute intestinal obstruction by keeping them nil by mouth, nasogastric aspiration, intravenous fluids and hypertonic saline enema twice daily. The hypertonic saline enema was used only for disentangling and expulsion of colonic worms and children were watched closely for any features of dehydration. No antihelmenthic drugs were given to the patient during the acute stage. Eighty-seven children (84.47%) responded favourably to conservative management and passed worms per rectally from third to fifth day onwards and did not require any surgical intervention. Only 16 children who presented with abdominal guarding or rigidity and those who developed them subsequently were taken for emergency exploration. In our center, we have managed three patients in five years. Two responded to non-operative management and one had laparatomy and enterotomy to extract the worms. Our protocol of management involved keeping them nil by mouth, nasogastric aspiration, intravenous fluids and antibiotics. Patients were given anti helminthes when they are out of obstruction. The first patient is KR, a 4-year-old girl who presented with colicky abdominal pain and non bilious vomiting of one day duration. Abdomen was soft with a vague mass at the left iliac region. Rectum was emptied. She was managed successful non-operatively and passed several bolus of worms (Figure 1) from 24 hours of admission. The second patient is SR, a 21/2-year-old girl who presented with sudden onset of vomiting and constipation of 6hour duration. On examination, she was conscious, afebrile with distended, soft and non tender abdomen. There were multiple vague abdominal masses. She also responded to non operative management and started passing bolus of worms from the second day of admission (Figure 2). The third patient had exploratory laparotomy for suspected intussusception but intra-operative findings revealed obstruction with Ascaris lumbricoides. She had enterotomy and extraction of the worms. She had uneventful postoperative period and was discharged home. From the foregoing, it is clear that non operative management of intestinal obstruction from Ascaris lumbricoides is associated with good outcome and avoids unnecessary surgery for children. Dr. Abdulrasheed A Nasir, Post fellowship Senior Registrar, Paediatric Surgery Unit University of Ilorin Teaching Hospital, PMB 1459 Ilorin, Nigeria. Email: draanasir@yahoo.com References
Copyright © 2009 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js09047f2.jpg] [js09047f1.jpg] |
| |||||||||

{kind=link}
{kind=link}