 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 15, No. 1, Mar-Apr, 2010, pp. 16-21 Breast Cancer Awareness among Females in a Developing World - A Study from KashmirS.A. Salat1, A. Rather2, S. Ahmad3, A.B. Khan4 1Department
of Surgical Specialties,King Fahad Medical City, Riyadh,Saudi
Arabia Code Number: js10003 Background: Breast cancer is a major health issue and in
developing regions, where the early cancer detection facilities are unavailable
awareness about this disease can lead to early detection and thereby
potentially decrease the morbidity and mortality. Introduction Breast Cancer is globally one of the leading causes of morbidity and mortality in women1. In underdeveloped and developing regions of the world, lack of awareness about breast cancer and facilities for early detection and treatment, results in delay in seeking medical care and hence in poorer prognosis 2. Presently, about 75,000 new cases are reported in Indian women every year. 3 This figure looks even more alarming if viewed against the backdrop that the National Cancer Registry and that the Hospital-based Tumor Registries hardly sample 3% of the total population. Advanced breast cancer (LABC) constitutes more than 50 to 70% of the patients presenting with breast cancer. 3 In Kashmir valley, dedicated breast cancer screening clinics are nonexistent and hence increased breast cancer awareness among general population can be a hope to fight this disease. A study was undertaken to study the level of awareness regarding breast cancer among Kashmiri females. Subjects and Methods The study was conducted in the Department of General Surgery, Sheri-Kashmir Institute of Medical Sciences,(Medical College), Bemina, Srinagar,Kashmir,India over a period of one year from August 2008 to July 2009 , to assess the level of awareness of breast cancer in Kashmiri women. Kashmir is a sub-Himalayan valley with a total population of about 6 million. The female visitors of patients were selected randomly and explained the purpose of the study as per the ethical guidelines of Helsinki. The ladies who agreed to participate in the study were requested to answer a self designed questionnaire after assuring them of confidentiality. The female medical interns in the department assisted in administering the questionnaire to subjects who did not understand the English language. The exclusion criteria included self or family history of breast disorders, on the presumption that their level of awareness will be higher. The questionnaire included basic signs and symptoms of breast cancer and breast self examination as shown in Table 1. The questionnaire was designed after taking text books of general surgery 4 and Toronto breast self examination inventory 5 into consideration. Attempt was made to simplify the questionnaire with the aim of getting insight into level of knowledge of subject with minimum possible consumption of time of the participants. There were 18 features related to breast cancer; for awareness of each feature a single point was awarded and no point was awarded if the lady was unaware. Accordingly three categories of breast cancer awareness were defined as per the total scores as depicted in Table 2. Table 1. Questionnaire to assess breast cancer awareness
Table 2. Categories as per the Attained Scores
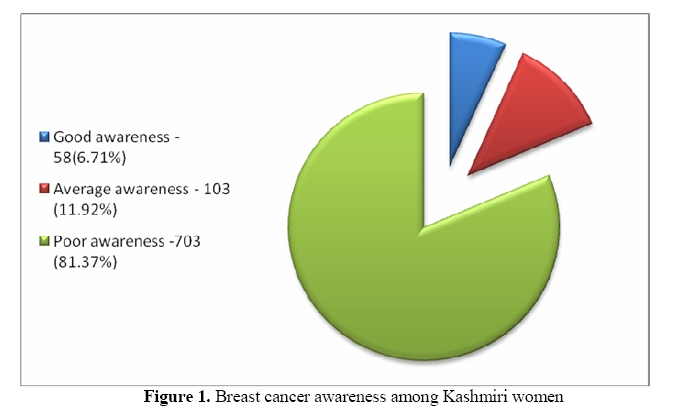
Data was processed and analyzed after one year of study period with the aid of SPSS software (statistical package for social sciences version- 10) for Windows. Statistical significances were determined by testing null hypothesis (computing p-values). Results During the study period 2132 females were approached for participation in the study and 864(40.49%) participated in the study. The results derived after analysis of data are given in the Figure 1 and Figure 2 and Table 3. Table 3. Awareness as per the Economic Status
Table 4. Awareness as per Educational Background
Table 5. Awareness as per Occupation
Table 6. Awareness as per the Age Group
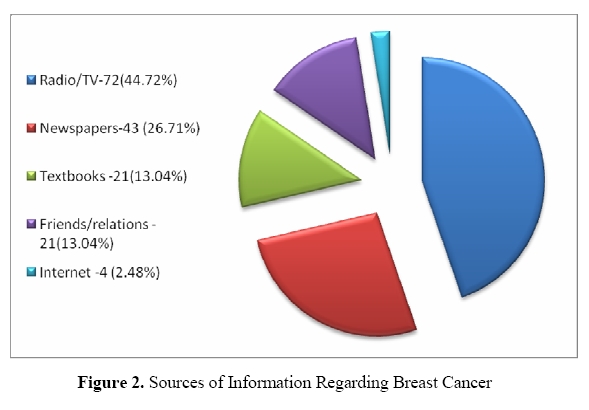
None of the subjects in our study was aware about the correct concept or technique of breast self examination (BSE). In the 161 patients who were found to have average (score 6-12) and good (13 and higher score) awareness, the sources of information regarding breast cancer are as given in Figure 2. Discussion Breast cancer is the commonest cause of cancer in females in most of the states of India 6 . The facilities of breast clinics for early detection of breast cancer are not available to a major percentage of the population both in India and Kashmir valley. The only feasible way to decrease the morbidity and mortality associated with cancer is when the females seek medical advice in early stages of the disease7 and in the absence of breast screening facilities; this can only be possible if the females are breast aware28 . Being ‘breast aware’ means that women should be aware of what is normal for them and what the features in the breast are, they should look and feel for. It was against this background, this study was undertaken to assess the breast awareness among our female population. A similar study regarding breast cancer awareness among Kashmiri males has been published by the authors separately 9. From our study, we found that out of 864 participants, 703(81.37%) had poor breast cancer awareness and 103(11.92%) had average awareness. Only 58(6.71%) had good awareness about breast cancer. This scenario is similar to many other parts of developing world 10, 11. However we could not detect any statistically significant difference (p>0.05) among the subjects when classified on the basis of economic status depicting thereby that improvement in economic status does not reflect in improved health related awareness. When studied on the basis of level of formal education, graduates and above were better aware than less or uneducated group (p<0.05). Similarly teachers and students were better aware though the difference was not significant. But the fact that about 72% of teachers had poor awareness about breast cancer needs a serious attention and improvement as it has been proved in many studies that by improving the health-related awareness among the teachers, the level of awareness in children improves significantly 12, 13 who in turn have been found to disseminate health awareness in homes and general population. However even in developed regions of the world, health education has not been found as a constant part of certification programmes of teachers 14. When classified on the basis of age-groups, the subjects belonging to 20-30 years age group had better awareness than other groups but most of these aware subjects were either graduates, students or teachers, so age alone per se cannot be considered as significant factor. Keeping in view this dismal state of awareness regarding breast cancer in Kashmiri women and the near absence of dedicated breast screening clinics, there is a need to improve the level of awareness as only that can lead to early reporting of breast cancer patients to healthcare facilities and thereby leading to ultimate reduction in morbidity and mortality of this disease. In many studies from India 15 and elsewhere, it has been clearly proved that, it is the lack of awareness and late reporting, that results in poorer prognosis of breast cancer. Breast self examination is still being advocated in developing countries as a method of early detection of breast cancer 11 though in developed countries its importance has faded due to availability of well equipped breast clinics 16 and the evidences that breast examination do not reduce mortality associated with cancer. None of our subjects had awareness about the correct technique of breast self examination. In other studies also 17, only a small percentage of females have been found to be aware of the correct technique. The sources of information included health related programmes on local radio, television and articles in local newspapers were sources of information of 71.4% of subjects having average and good awareness regarding breast cancer. Since these sources are widely available, impetus needs to be laid on further and focused utilization of these means of education to improve breast cancer awareness among masses. Special teachers training sessions need to be organized particularly during winter vacations when schools remain closed for three months as these in-service training sessions have been found effective in other health related issues 12. Change to positive result can be achieved by establishing a definite role for schools and teachers in promotion of health 18. Even the social and religious leaders can also be educated and made part of a programme aimed at health education as they have direct access to the population and can influence their knowhow19. Conclusion Breast cancer awareness is very low among Kashmiri women .In the absence of breast cancer screening clinics, there is a dire need to take measures to improve breast cancer awareness so that the patients might present earlier in the course of this killer disease. References
Copyright © 2010 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js10003f2.jpg] [js10003f1.jpg] | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}
{kind=link}