 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 15, No. 1, Mar-Apr, 2010, pp. 57-61 The Impact of Bodaboda Motor Crashes on the Budget for Clinical Services at Mulago Hospital, KampalaJ. Kigera, L. Nguku, E.K. Naddumba Department of Orthopedics, Mulago Hospital, Kampala
Uganda Code Number: js10009 Background: Bodabodas
are a common form of transport and are becoming a major cause of road traffic
accidents in Uganda. We evaluated the magnitude of injuries related to
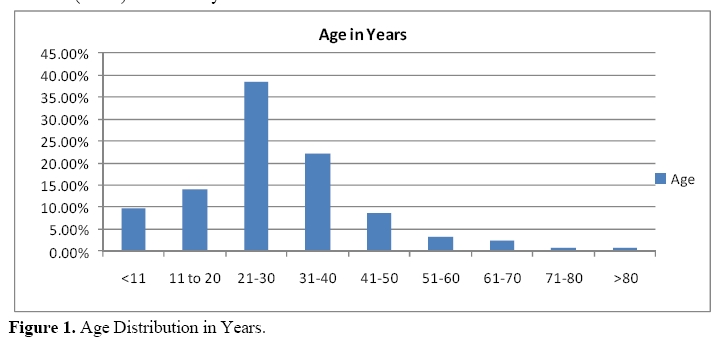
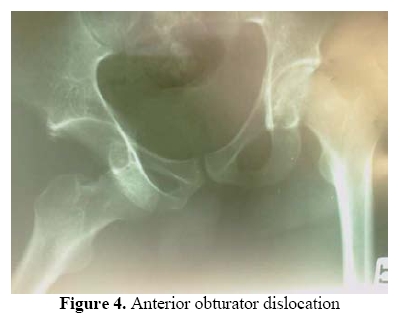
bodabodas and their impact on clinical services at Mulago hospital. Introduction Bodaboda motorcycles are a common and popular form of transportation in Kampala city and in many other towns in Uganda. Since their introduction in Kampala in 2001, there has been an increase in the number of road traffic crashes many attributable to them. The percentage of accidents attributable to bodabodas between RTCs has been increasing annually. Bodabodas are also the leading cause of accident scene fatalities in Kampala1. Road traffic crashes and in particular bodaboda ones commonly affect the young adults in the 20 – 29 years age group2.This is because the bodabodas business is dominate by youths as a means to a livelihood. Naddumba3 in his study found that the peak age incidence of both the riders and passengers was in the 20-30-age group. Otieno4 reported that 14.5% of all patients with long bone fractures were due to injuries sustained while riding while Lule5 found that bodabodas trauma accounted for 25.6% of all tibial fractures. This study was aimed at determining the magnitude and cost implication of injuries caused by bodabodas at Mulago hospital. The study also undertook to quantify the impact of these injuries to the provision of quality services at Mulago. Direct costs resulting from the injury and its management were derived. Patients and Methods This retrospective study included all patients admitted for trauma at the emergency surgical ward in the three-month period ending 30th August 2008. Patients’ files were analyzed for the demographic data, the cause of trauma, diagnosis on admission, duration of stay and operative procedures performed. An accident was deemed to have involved a bodaboda if the patient was a passenger, a rider or was hit by a bodaboda. The data was collected using a research tool designed for that purpose and later keyed in to a computer using MS Excel. The data was then analyzed. Details on costs associated with hospital stay were derived from the hospital statistician’s office. Costs were calculated based on the average cost of maintaining a patient in the ward per day, the costs of surgical procedures done and the cost of any implants used in surgery. Results Records of 921 (61.4%) of the 1500 trauma cases admitted during the study period were retrieved and analyzed. Road traffic crashes contributed 51% of all trauma patients seen. Of the 428 patients admitted after RTCs, 75 % were due to bodaboda accidents. The majority (80.6%) of the cases were males with a male to female sex ratio 4.2:1. The peak incidence was in the third decade of life. About two thirds of the patients were aged between 20 and 40 years and 85% of all patients were below 40 years of age (Figure 1). Table 1 shows the number of patients that required surgical intervention during the study period. Nearly half (49.7%) of them had sustained bodaboda injuries. Lower extremity injuries especially open fractures were predominant. Figure 3 shows injury sustained by a bodaboda passenger who was thrown off the motorcycle when it collided with a truck which then ran over her thigh. She suffered a traumatic amputation above the knee. A rare form of an obturator anterior hip dislocation (Figure 4) was among the victims. The patient was thrown off a bodaboda that had knocked down a pedestrian. He presented to hospital two weeks after the injury and underwent open reduction for the anterior Hip dislocation. Majority of the closed fractures of the femur were managed by open reduction and IM nailing using implants from the Surgical Implant Generation Network (SIGN) and some by skeletal traction. Table 1. Patients requiring surgical intervention
Table 2. Operations requiring implants
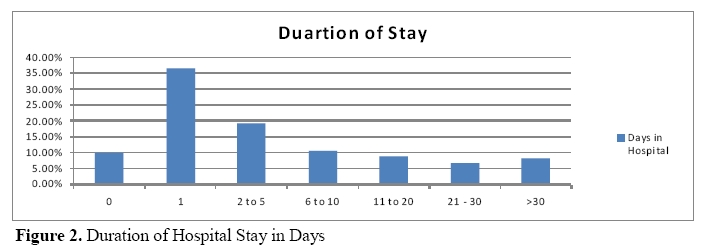
Of the 203 Patients requiring theatre about half were due to bodaboda injuries and of these 75% required the services of an orthopedic surgeon (Table 1). Table 2 shows the operation that required implants. The Duration of hospital stay of the patients ranged from 1 to 105 days with a mean of 8.3 days (Figure 2). The average cost of maintaining a patient in the wards was UGX 56,740. With an average length of stay of 8.3 days, the average cost per patient translates to Uganda Shs 470,942. The total costs for maintaining the patients in the wards were UGX 151,172,382. The total theatre costs attributable to patients with injuries caused by bodaboda were UGX 73,642,813. This was for the 101 patients who required operative management. The total costs added up to UGX 224,815,195 for the three-month period studied. This cost excludes rehabilitation costs, which we were unable to determine and quantify. The average cost of managing a bodaboda patient is hence calculated at UGX 700,359 (USD 369) Discussion Bodabodas were responsible for about 75% of all trauma caused in road traffic collisions. This is a very high figure when compared to other countries in the region. A study in Rwanda estimated that motorcycles were responsible for about 30% of all RTCs6. This difference may to a great extent be explained by the facts that in Rwanda there are strict laws governing bodaboda ridders and users that are strictly abided by. For instance, in Rwanda both the motorcycle rider and his passenger must strictly wear helmets which law, in Uganda, has not been enforced by the police. Most of the patients admitted due to injuries related to bodabodas were in the economically viable age group and at the prime of their lives. These injuries hence result in disruption of economic activities and a further drain in the incomes of these patients. Naddumba3 in 2001, found that majority of bodaboda accident victims were self employed and hence will not generate any income while they are in hospital and at home recuperating from their injuries. Most of the patients who were involved in bodaboda accidents tended to have more severe injuries and this may be due to the fact that most accidents tend to involve collisions with motor vehicles and the unprotected bodaboda riders and passengers bear the brunt of the impact3. The total cost of managing all inpatients due to bodaboda injuries is UGX 224,815,195 in the three-month period of the study. This translates to UGX 899,260,780 a year. Given the fact that that we were only able to collect data from about 60% of the files we anticipated, it can be postulated that the total cost is in the region of 1.5 billion shillings each year. When weighed against the budget allocation for the Directorate of Surgery of about 2.4 billion shillings annually, this translates to 62.5%. This is a colossal sum of money could have been used up by one aspect of the greater field of surgery. The costs attributable to bodaboda injuries comprise a significant 15% of the 10 billion shillings allocated to Mulago for health services and 4.2% of the total budget for Mulago for the year 2008/2009 (35 billion shillings). This is a colossal sum given that Uganda is a developing economy and these funds could be utilized in other areas. It should be noted that part of these costs were borne out by various donors most notably the SIGN organization that provides intramedullary implants and the Health Volunteers Overseas that provided most of the external fixator implants. A reduction in the number of trauma cases seen at Mulago hospital most of which are from bodabodas will free up space for the hospital to attend to other pressing matters. Trauma has overwhelmed the orthopedics department and hence skewed teaching of residents who require exposure in areas of adult and pediatric orthopedics. Conclusion
Recommendations Efforts should be geared towards prevention of injuries attributable to bodabodas. Regulation of training and operations of bodabodas will go a long way in ensuring that this mode of transport is safe to its users. The traffic regulations and the Highway Code should be strictly enforced by the police so as to reduce carnage on our roads. Health authorities should empower hospitals managing these injuries with the necessary resources to properly manage these patients. These will range from personnel, equipment and implants. References
Copyright © 2010 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js10009f3.jpg] [js10009f2.jpg] [js10009f1.jpg] [js10009f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}