 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 15, No. 1, Mar-Apr, 2010, pp. 62-71 A Comparison of Kampala Trauma Score II with the New Injury Severity Score in Mbarara University Teaching Hospital in UgandaMutooro S.M, Mutakooha E, Kyamanywa P. Department
of Surgery Mbarara University of Science and Technology, Uganda; Code Number: js10010 Background: Road
traffic injury is of growing public health importance because of its
significant contribution to the global disease burden. The need to predict
outcome of injuries has led to the development of injury scores. The Kampala
Trauma Score II (KTSII) now recommended for use in resource-poor settings, has
not been compared with, the New Injury Severity Score (NISS) preferred by many
authors. We compared the performance, predictive power, sensitivity, and
specificity in predicting mortality at two weeks of the KTSII and NISS in
patients involved in road traffic accidents seen on the surgical ward at
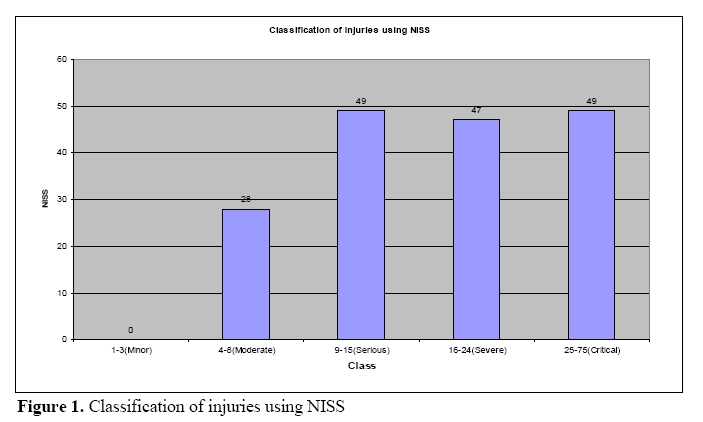
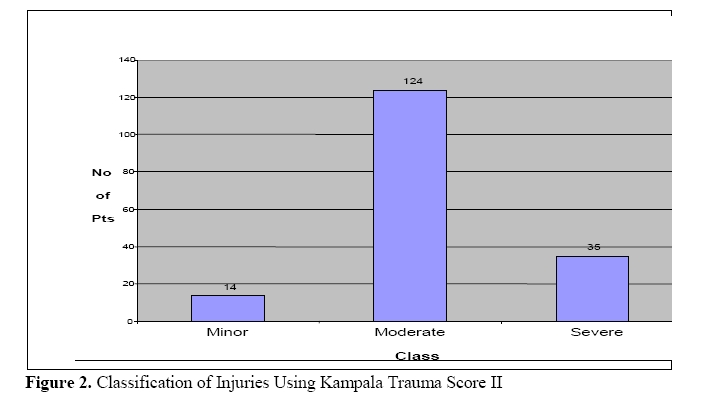
Mbarara Regional Referral Hospital (MRRH). Introduction The high rates of road traffic injuries and the complexity of management, focusing on the treatment and outcome of injuries, brought about the development of injury scores1. Injury scores quantitatively summarize injury severity and have played a major role in the management of road traffic injuries in the developed countries due to an improved triage. The improvement in triage has been shown to contribute to 28% reduction in fatality rates in some centres2. Injury-scoring systems are either anatomical, physiological or combined anatomical/ physiological scores. The New Injury Severity Score (NISS) introduced in 1997 is considered by some authors as the “gold standard” injury severity score3. However, the severity scores used in industrialized countries are complex and require extensive retrospective review of completed patient records. This has made such scores difficult to apply in resource poor settings. In 1996, the Injury Control Center – Uganda (ICCU) developed a new simplified trauma outcome prediction model; the Kampala Trauma Score I (KTS1). KTS I is a simplified modification of the RTS and ISS scores.4,5 The KTS I has been promoted for use in resource-poor settings for easy scoring of injury and prediction of outcome in trauma patients.6 The KTS I was revised in 2002, giving rise to the KTS II. Although KTSII is said to be a more simplified injury severity instrument for use by most health cadres it has not been validated for predicting mortality and need for admission. We set out to compare the KTS II against the NISS as a measure of injury severity and its ability to predict mortality and need for admission in road traffic injured patients. Patients and Methods Data was collected at the Emergency unit of the Surgical Department at Mbarara Regional Referral Hospital that also serves as the main teaching hospital for Mbarara University of Science and Technology. All patients aged 18 years and older admitted to the Emergency ward between June 2005 and August 2006 with road traffic injury in the preceding 24 hours, were eligible for the study. Additional inclusion criteria were: Patients who had sustained three major injuries involving any of the four body organ systems (integument, bone, nerve, and vessel); and patients with three minor injuries and one major injury involving the above organ systems. Patients referred to the hospital after initial surgical management, were excluded from the study. On admission, patients were resuscitated following trauma care protocol until they were hemodynamically stable. Patients’ demographics, details of the injury, initial clinical assessment and calculation of KTSII, NISS, were compiled by the same team of staff. The unconscious patients with no informants were identified as unknown until identified. All patients received the necessary medical care as per the injury(s) sustained in order to assess the predicted outcome by the two scores in the second phase. Surgical management was carried out wherever indicated. The second phase involved active follow-up of the patients for two weeks both on ward and as outpatients. Indications of severity of injury and complication were a hospital-stay longer than two weeks, requirement for re-debridement and death. All data was entered into the Epi-Info version 3.3.2 statistical packages and exported to Statistical Package for Social Scientists (SPSS) version 12.0 for analysis. Receiver Operating Characteristics (ROC) curve for NISS and KTSII as predictors of mortality at two weeks were constructed and the areas under the curve (AUC) based on non-parametric assumptions were generated for each KTSII and NISS, and compared (Appendix 1 for KTS II and NISS description). Similarly ROC curves for prediction of hospitalization at two weeks were constructed. The KTSII was compared to the NISS on the cohort database using logistic regression. Odds ratio and 95% confidence interval were computed for each model. The two scores were again compared at 90% sensitivity and 90% specificity for the performance of the corresponding sensitivity, specificity and a likelihood ratio for a positive test (LR+). McNemar chi-squared, (X2) test for paired data were used to test for the statistical significance of the differences. Results One hundred seventy three patients were recruited. There were 145 (83%) males, giving a male-to-female ratio of 5:1. Peasants and students were the most vulnerable of the of road users (22% and 15.6 % respectively) as per occupation. Passengers were the most commonly injured category of road user. On further analysis, passengers on motor-cycles accounted for 69% of the passengers injured. The productive age bracket between 18 and 45 years formed the majority of patients seen (80.3%), while those above 45years of age stayed longer in hospital. The majority of patients had penetrating injuries (58%) while 41.6% had blunt injuries. Seventy six percent of the study population sustained fractures. Patients who sustained cuts and bruises were 40.2%. Out of these, 60.4% had cuts and bruises more than 5cm wide, 42.9% underwent debridement of the wounds, only 8.7% had wound sepsis. Open fractures accounted for 36.3% of the musculoskeletal injuries seen. Closed fractures and dislocations accounted for 15.9% and 7.6% respectively. The head and extremities were the most inured body regions (Table 1). Using the NISS classification, most (84%) of the injured patients were classified as serious, severe or critical (Figure 1) while the KTS II classified most (71.7%) of the injured as moderate (Figure 2). At the end of two weeks, the outcomes were recorded as died, discharged and still in the hospital. 100 patients (58%) were discharged; 24 (14%) run away and an equal number were still admitted at two weeks. 25 patients (14%) had died over the two weeks (Table 2). Table 1. The Frequency Distribution for Body Region with Serious Injuries
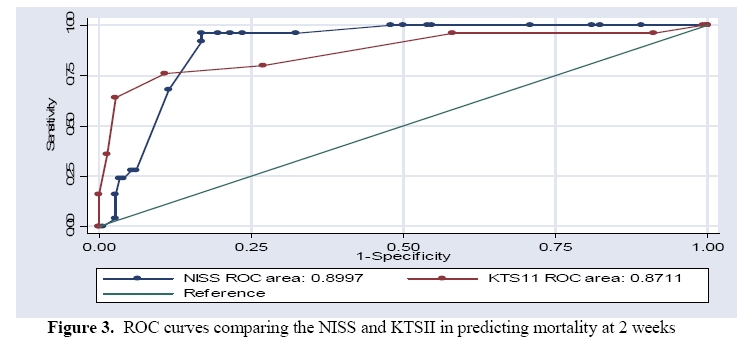
Prediction of mortality and hospitalization using NISS and KTSII The majority of the patients who died had NISS of 24 while those who were still hospitalized had NISS of 16. The KTS II scored such patients as having KTS II of 16 and 14 respectively. The performance of the two scores were assessed and compared in terms of mortality prediction and still hospitalized using the ROC. Figure 3 shows a comparison of KTSII and NISS in predicting short-term mortality. At 95% confidence interval of NISS as 0.852- 0.948, the KTSII has 0.791-0.951, both with P=000. Table-2 Frequency of deaths/hospitalization as classified by NISS/KTSII
At the end of two weeks, the outcomes were recorded as died, discharged and still in the hospital. 100 patients (58%) were discharged; 24 (14%) run away and an equal number were still admitted at two weeks. 25 patients (14%) had died over the two weeks (Table 2). Prediction of mortality and hospitalization using NISS and KTSII The majority of the patients who died had NISS of 24 while those who were still hospitalized had NISS of 16. The KTS II scored such patients as having KTS II of 16 and 14 respectively. nThe performance of the two scores were assessed and compared in terms of mortality prediction and still hospitalized using the ROC. Figure 3 shows a comparison of KTSII and NISS in predicting short-term mortality. At 95% confidence interval of NISS as 0.852- 0.948, the KTSII has 0.791-0.951, both with P=000. Table-3. The prediction of NISS and KTSII for short-term mortality New Injury Severity Score
Kampala Trauma Score II
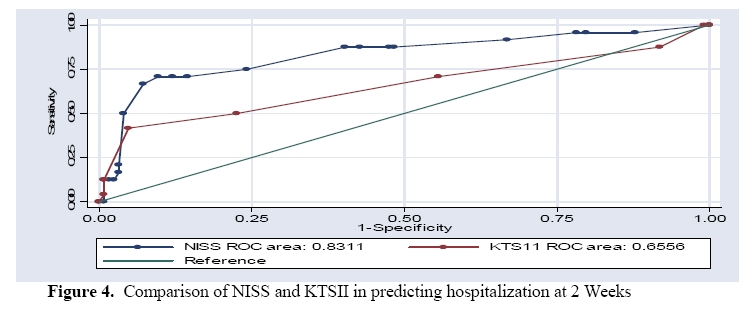
Prediction of status of hospitalization at two weeks Figure 4 shows the ROC for the predictive ability of the two scores for the status of hospitalization (still in the hospital). The ROC area under the curve for NISS (0.831) was compared at 95% confidence interval of 0.728-0.935, and KTSII (AUC-0.6556), at 95% confidence interval of 0.511-0.800, both with P=. 005. Comparison of predictive power of KTSII and NISS A two-predictor logistic model was fitted to the data to test the research hypothesis regarding the relationship between the likelihood that the two scores predict mortality equally. The variable (mortality) was then fitted in the logistic regression equation and the results are shown in table 3. The proportion of the variation in the mortality rate that can be explained by NISS was 0.304 while the KTSII showed a proportion of 0.383 (chi-square 49.7, p-value 0.00). NISS is statistically better than KTSII in prediction of mortality. Comparisons of sensitivity and specificity at cut off points for the NISS and KTSII in prediction of mortality at two weeks. The sensitivity of NISS and KTSII as predictors of mortality at two-weeks at cut-off points was compared. At a cut off of NISS 20, the NISS had a sensitivity of 96% and specificity of 78.3% (90%CI 4.44-0.05; OR 1.18; p-value 0.000). This is in comparison to 64% sensitivity and 60% specificity (90%CI 0.064-26.6; OR 0.35, p-value 0.00) for the KTS II at a cutoff score of 9. Comparison of sensitivity and specificity of NISS and KTSII in predicting stay in hospital at two weeks at a 90% CI was not statistically significant. The NISS had a sensitivity of 70.8% and specificity of 87.9% (90%CI 0.204-20.101), compared to a sensitivity of 87.5% and specificity of 69.0% (90% CI 0.950-2.196) for the KTS II. Discussion The demographic characteristics of the patients seen in this study and the proportion (37%) of injuries due to road traffic reflects the huge burden of road traffic injuries in our society. A similar pattern has been cited in other studies.5,7,8,9. The KTSII classified majority of injuries registered as moderate injuries while NISS classified them as serious and critical injuries. The difference between these distributions is due to the fact that KTSII is a combined score while NISS is anatomical score. The KTSII therefore classified the injuries less accurately than NISS since KTSII has less anatomical parameters.However NISS classified injuries in MRRH similar to other reported studies while there was a significant difference in the classification of injuries between MRRH and the hospitals in Kampala city reported by Kobusingye and Guwatudde8 using KTSI. Among the city Hospitals, Kibuli had a relatively higher proportion of injuries classified as moderate and severe (11% and 5% respectively using KTSI). In comparison with MRRH using KTSII, the proportion of moderate and severely injured patients was 71.7% and 20.2% respectively. The difference is as a result of using KTSII, a more accurate and specific score than KTSI. The bony pelvis and/or extremities were the most commonly isolated body region injured 48.5%, followed by head, 34.1%. In addition, the majority of patients sustained penetrating injuries. Mugabi10 and Odero7 reported similar findings and attributed it to failure to observe road safety precautions. Similarly most passengers, drivers and cyclist in this study, did not observe road safety precautions. In a study by MacLeod et al4, the highest number of deaths occurred with KTSI <14 while in the present study, the highest number of deaths occurred with KTSII <6. The difference in the scoring most likely arose from the upgrading of KTSI where the score for each phrase is reduced from 1-4 to 0-3 as in KTSII. The outcome at two weeks The highest percentage of patients who died (44%) as classified by NISS was almost double those assigned by KTSII (28%). The difference in classifying was statistically significant (p = 0.000) for NISS at 95% Confidence interval of 0.102-0.226 and -1.428 to -0.700 for KTSII. This difference is due to the fact that NISS assigns a score depending on the severity of injury(s). Whereas KTSII assigns a score whether the injury is present as one or not present which does not describe the severity of injury. The highest percentage of NISS & KTSII for survivors but still in hospital at the end of two weeks was compared, and KTSII was higher than NISS by 2%. This indicted that KTSII predicts survivors better than NISS. Neurological compromise continues to be a major underlying factor in the outcome of injuries and KTSII assesses central nervous system better than NISS. This supports studies by Mohammed et al11 that physiological scores predict survival better than anatomical scores. At 95% confidence interval, NISS had 96% sensitivity and 78.4% specificity, in discriminating those that died, from the survivors while KTSII had 87% sensitivity and 81% specificity to discriminate the two categories. This indicates that NISS correlates well in prediction of mortality than KTSII. The observed cut off point in this study was similar to the results obtained by Brennaman et al.12 Considering the 60.5% sensitivity reported previously during the development process of KTSII and the present study (87.0%), the upgrading of KTSI to KTSII improved the sensitivity of the score. This improvement in sensitivity followed the assigning of a lower score value to a more severe injury. Performance assessment of KTSII and NISS The ROC shows the ability of the two scores to predict mortality in the study population based on Area Under the Curves (AUC). The NISS (AUC 0.899) provided the better prediction of hospital mortality than the KTSII (AUC 0.871). Osler et al13 and Balogh et al14 reported similar findings of NISS in predicting mortality as the current study. The difference in KTSII performance as compared to NISS in this study was not statistically significant. The magnitude of the difference in AUC was marginal; hence KTSII would be used with confidence. The KTSII had limitations in scoring patients who were intubated and those under the influence of alcohol. KTSII also failed to score multiple injuries in the same body region. These limitations are identical to findings by Balogh et al14 who had reported such limitations associated with RTS and ISS, in predicting mortality. While the NISS was difficult to use at the bedside since it requires AIS dictionary. The KTSI performed better in predicting mortality than the KTSII in present study. The disagreement between the two scores as observed by Mugabi10 and may have been due to the fact that such limitations were not excluded in the present study. The patients were thus underscored by KTS II accounting to less prediction in mortality. Recent studies have shown that the component of ‘best motor response’ in physiological/combined scores adds more weight in predicting trauma mortality. KTSII lacks such components. The study population of 173 respondents included 85 (49%) patients with head injuries and 35.8% patients who had taken alcohol. The KTSII therefore underestimated the severity of these two major categories of patients in the study population, leading to a low predictability of mortality. Prediction of two weeks Hospitalization The NISS (AUC_0.831) predicted ‘still in the hospital’ better than KTSII (AUC 0.656) in this study, the KTSII predicted ‘still in the hospital’ similar to the reported findings in earlier studies.4,5,10 This indicted that the upgrading of KTSI to KTSII did not add predictive value to “still in the hospital” patients. The NISS predicted those who were hospitalized as having wound or fracture complications better than KTS II. This is due to the fact that the KTSII does not take into account the severity of a particular injury than only mentioning its presence. The KTS II behaves more less a physiological score similar to its parental score the TRISS, much as it is a combined score. Predictive power of KTSII and NISS The separation of the severity score value(s) for survivors versus non-survivors is a rough indication of the predictive power of the test.15 According to Wilcoxon non-parametric methodology, ROC judges the discrimination ability of different statistical models. Higher separation of score values for one test against the other indicates a higher accuracy and its discrimination ability. In this study, NISS predicted short-term mortality better than KTSII with a small difference, 0.899 and 0.871 respectively. Furthermore, the two scores accurately discriminated between patients to be discharged, and those still in hospital. The KTSII was observed to have an accurate discriminative ability to perform both tasks comparable to the gold standard score. Husum and Strada15 disagreed with findings by Osler et al13 and Brenneman et al12 that NISS performs slightly less in penetrating injuries while considering missile injuries. The present study population consisted of both penetrating injuries (58%) and blunt injuries (41.6%), with penetrating injuries being the majority, where the NISS performed with preference. Commenting on such disagreement however, needs a pure study population of road traffic penetrating injuries other than injuries caused by missiles. However, NISS and KTSII performed differently as prediction models different cut-off values. Where as the NISS almost approached sensitivity of one the KTSII was closing to a sensitivity of 0.8. This justified the fact that NISS has better performance in predicting mortality/still in the hospital, as compared to KTSII. However the KTSII was greater than 0.5, hence its predictive ability is not by chance. The NISS performance was slightly higher than that reported in an earlier study13. Comparing the predictive power of KTSI and KTSII (present study), the results indicated that KTSI nearly approached 0.7, where as KTSII approached 0.84. This stresses the improvement from KTSI to KTSII in prediction ability. Comparison of NISS and the KTSII at 90% sensitivity and specificity The NISS, at cut off point 16 and below was 88% sensitive in identifying those who died and 60% for those still in the hospital at two weeks, in comparison to 73% and 80% respectively for KTS II. In general, the two scores were sensitive at detection of mortality among the study population though KTS II was slightly less than the NISS. This was attributed to the improvement of KTSII, by assigning a small value to an injury, which corresponds with the severity of injury. This was opposed to the KTSI that would have assigned a higher value, which would indicate survival in a related injury. The McNemar value of 0.727 shows a statistically significant difference between the two scores. The difference is attributed to the fact that the two scores have different in-built anatomical/ physiological properties. Therefore, the two scores cannot be good at predicting mortality, survival and hospital status at two weeks with the same accuracy. Most scoring systems studied, have such characteristics of high sensitivity (prediction of mortality) and low specificity (prediction of survival). Conclusions The two scores quantitatively summarized injury severity and predicted the outcome though differently, as survival, death or long stay in the hospital. Furthermore, the KTS II was easier to compute given the fewer parameters and the simple addition of scores. This therefore will help to enhance quality medical service delivery to the injured in Mbarara Regional Referral Hospital through easier triage. The intensive care unit team will find the KTSII application helpful in providing objective information for prognostication. The scores especially the KTSII, may enhance appropriate use of ambulance services and timely transfer of severely injured patients to trauma wards. The classification and stratification of patients into comparable groups using scoring systems, is useful in clinical studies of the epidemiology of trauma. The ‘ease’ of the KTSII to predict the outcome can be used retrospectively to identify and control for differences in baseline injury severity between patient populations during epidemiological studies. Although developed in an urban hospital better equipped than MRRH, KTSII performs well as a triage tool on admission in rural set-ups. Furthermore KTSII performance was comparable to the NISS in this study. Appendix 1. NISS Description AIS Severity level Example
NISS = Square of (AIS) Source: Eur J Trauma (2002; 28:52–63) Kampala Trauma Score (KTS II) Description
References
Copyright © 2010 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js10010f1.jpg] [js10010f3.jpg] [js10010f4.jpg] [js10010f2.jpg] | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}