 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 15, No. 1, Mar-Apr, 2010, pp. 72-77 A Comparision of Clinical Diagnosis and Knee Arthroscopy Findings at Mulago HospitalI. Kajja, L. Nguku, T.Beyeza Department of Orthopedics Makerere
University College of Health Sciences. Code Number: js10011 Background: Many patients present
to the orthopaedic surgeon with complaints of knee pain. In many such cases
making a diagnosis based on clinical examination is often difficulty and
frequently inaccurate. This study sought to document the common findings at
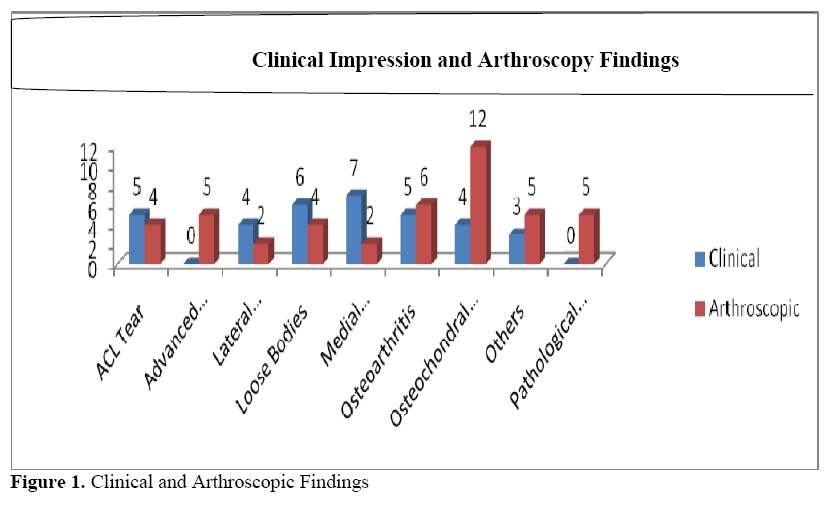
knee arthroscopy and how they compare with clinical impressions. Introduction Up to 28% of patients presenting to orthopaedic surgeon in an outpatient setting complain of knee pain (1, 2). The causes range from trauma, degenerative joint conditions, infections, inflammatory conditions to congenital lesions (3). In the diagnosis of the lesion in the knee, the surgeon has to obtain a thorough clinical history, examine the patient and do investigations as may be required. Arthroscopy is regarded as the gold standard among the investigative modalities (4-7). The commonly missed diagnoses in the knee are osteochondral fractures, partial anterior cruciate ligament (ACL) tears and loose bodies (8). Failure to recognise these has both medical and socioeconomic complications. The common medical complications include an unstable knee, chronic knee pain and post traumatic arthritis (9, 10). The socioeconomic complications include loss of income during the duration of treatment, high cost of medical care for procedures such as total knee arthroplasties and a perception of general poor health (11). At Mulago hospital, up to 2% of the patients presenting to the orthopaedic out-patients clinic have knee pain without a definite clinical diagnosis and require diagnostic arthroscopy to define the pathology. This study therefore intended to compare the correlation of clinical impressions and arthroscopic findings and therefore asses the sensitivity of clinical assessment. Methods A cross sectional study was conducted at the Mulago Hospital orthopaedic ward between September 2008 and Jan 2009. Thirty four patients were recruited in the study. All the patients were referred by an orthopaedic surgeon for a diagnostic knee arthroscopy procedure and thereafter the relevant management. We excluded any patient whose diagnosis was based on another investigative modality and patients who were suspected to have septic arthritis of the knee(s). The arthroscopy was performed by one surgeon in all cases. The procedures done under asceptic condition was performed either under general or spinal anaesthesia and used a A high thigh esmarch tourniquet. A 30o Aeusculap arthroscope with a 250w Aesculap light source was used. The portals used were the anterolateral for the arthroscope, anteromedial for the probe and if necessary the superolateral or superomedial for the probe. The diagnostic procedure was then performed. . The data collected was analysed using SPSS Ver. 12. The independent t test was used to compare the means of the male and female populations. The categorical variables were cross tabulated and subjected to the Fisher’s exact test to ascertain the statistical significance. Results were termed significant if the p value was < 0.05. Calculations for sensitivity, specificity, positive predictive value, negative predictive value, accuracy missed diagnoses and relevant p values were done using the following formulae: Sensitivity = True Positives x 100 / (True Positives + False Negatives), Specificity = True Negatives x 100 / (True Negatives + False Positives), Positive Predictive Value = True Positives x 100 / (True Positives + False Positives), Negative Predictive Value = True Negatives x 100 / (True Negatives + False Negatives), Accuracy = (True Positives + False Negatives) x 100 / (True Positives + True Negatives + False Positives + False Negatives) and Missed diagnoses = False Negatives x 100 / (False Negatives + True Positives). Results Of the 34 patients recruited, 23 (68%) were male and 11 (32%) were female. The mean (SD) age for the patients was 38.35 +/-9.43 years with a range of 8 – 81 years. There was a significant difference in the mean ages of the male and the female patients. The mean age for the male patients was 31.52+/- 2.65 compared to 52.64 +/- 7.23 years for the females (p = 0.016). Most of the patients seen were professional sportsmen, 12 (35%) having sustained the injuries in the course of playing (Table 1). The commonest preoperative diagnosis was a medial meniscal tear, while the least common was a clinical impression of knee pain. However at arthroscopy the commonest findings were osteochondral lesions in 12 (27%) and osteoarthritis in 6 (13%) (Figure 1). Nine patients had multiple knee pathologies (Table 2). Table 1. Patients' Occupations
Table 2. Multiple Findings at Arthroscopy
Table 3. True positives, true negatives, false positives and false negatives with reference to arthroscopic findings.
Table 4. Accuracy of Clinical Findings
P value obtained by the Fisher’s exact test The highest true positive clinical impression based on diagnostic arthroscopy as a gold standard was osteoarthritis (5 out of 34) while all clinical impressions had high true negatives.(Table 3). The clinicians’ impressions were most sensitive for looses bodies (100%) and most specific for osteoarthritis (100%) - (Table 4). Discussion The male population is usually at a higher risk of suffering traumatic knee pathologies. This has been proved by this study and others, both within and outside Africa (12-16). This could be due to the fact that males are more involved in active sports than females hence the higher risk of injury. The female patients on the other hand, having lived more sedentary lives tend to gain weight and later present with degenerative knee conditions. Brooks in 2002 (14) also noted that the were more elderly female patients than male patients, implying a higher incidence of degenerative knee conditions among females. Traumatic lesions comprise the commonest indications for knee arthroscopy. In their series, Terry had 197 of 216 patients, and Brooks 140 of 238 patients with traumatic lesions of the knee (14, 17). In this study about two thirds of the patients had such lesions. However, up to a third had degenerative knee lesions. Worldwide, meniscal tears constitute the largest group in the preoperative clinical impressions (17). The anatomical position of the menisci is between two hard structures, the femoral and the tibial condyles. This predisposes them to degenerative and traumatic injuries. The medial meniscus is less mobile as compared to the lateral meniscus due to its attachment to the medial collateral ligament, predisposing it more to injury. Three study patients did not have defined clinical impressions other than knee pain. Making a definite clinical impression is not easy especially in the presence of rare or multiple pathologies in the knee (8). At arthroscopy one was found to have a normal knee. In the remaining two patients, one had relatively rare multiple pathologies (advanced synovitis and a pathological synovial plica). Accuracy of clinical diagnosis has been suggested to be lower in multiple pathologies (8). The third was a lateral meniscal tear in a 30 year old housewife with no clear history of trauma, a factor that may have contributed to the physician’s inability to diagnose the lesion. While in other studies the commonest finding at knee arthroscopy is a meniscal tear (12, 14-17), in this study it was an osteochondral lesion. Mulla in Zambia found meniscal injuries to be the commonest arthroscopic finding (34%). He had no report of any osteochondral injuries (15). In his study of 1000 patients, Hjelle in Norway had a 57% prevalence of meniscal injuries and only 15% of his patients had osteochondral injuries (16). Terry in the US, in a study of 216 patients, had a 71% prevalence of meniscal injuries at arthroscopy. Osteochondral injuries were only seen in 1% of his patients (17). The discrepancy in the findings could be due to a larger sporting population in the cited countries. In this study’s sample, only about a third of our patients were involved in sports. The rest of the patients could have contributed in skewing the results in favour of non-sporting pathologies. In the criteria of this study, any patient who was suspected to have sepsis or a septic arthritis was excluded. At arthroscopy, one patient was found to have a resolving septic arthritis. This had not been suspected by the referring physician and the patient had been referred with a diagnosis of a medial meniscal tear. In the resolution stage of septic arthritis, the acute features of fever, knee pain, swelling and warmth are usually missing. Within the knee, there may also be arthrofibrotic changes. These factors could have made it more difficult for the physician to make the correct clinical impression. Correlation of clinical impressions and arthroscopic diagnosis Many studies have been done with the aim of assessing the accuracy or reliability of clinical examination in diagnosis of knee derangements. Some have been for general knee conditions (8, 14, 17-22) and some for specific lesions (12, 13, 23, 24). The accuracy of clinical diagnosis in these studies ranges from 21-83%. The overall accuracy of 87.2% rates higher than O’Shea’s figure of 83%, the highest noted accuracy (22). O’Shea’s study was conducted at a US army hospital and a total of 156 patients were seen. The high clinical accuracy obtained may have been primarily due to the inclusion of radiological findings in arriving at a primary clinical impression. The high accuracy in this study, however, may be due to the large number of easily diagnosed conditions of the knee that were seen. Up to a third of the conditions seen were relatively easy to diagnose by clinical assessment, namely: osteoarthritis, loose bodies and ACL tears. Most of the missed diagnoses were due to osteochondral lesions. This is similar to the findings of Yoon (8). Loose bodies and osteoarthritis, being rather easy to diagnose were less frequently missed. Of the eight misdiagnosed osteochondral lesions, four were diagnosed as medial meniscal tears, two as lateral meniscal tears and two as ACL tears, a pattern similar to that seen by Terry (17). In his study, all the six osteochondral lesions were missed: four patients were misdiagnosed as medial meniscal tears and two as lateral meniscal tears. The one misdiagnosed medial meniscal tear had been thought to be an ACL tear while the misdiagnosed lateral meniscal tear had been diagnosed just as knee pain. The one case of osteoarthritis that was missed on clinical examination had been diagnosed as a loose body in a 59 year old ex footballer. All the patients with loose bodies were correctly diagnosed by clinical examination. There were nine knees with multiple pathologies. In one of the nine, the referring physician made a correct diagnosis of two co-existing pathologies that were confirmed at arthroscopy. In four of the nine, the physicians made a correct diagnosis of one of the pathologies affecting the knee. In the remaining four of the nine knees the physicians missed the diagnoses. This proves what both Esmaili and Yoon have reported in their papers, that clinical accuracy decreases with an increased number of knee pathologies(8, 12). Patients with multiple knee pathologies will have an atypical clinical presentation making it difficult for the physician to arrive at a diagnosis. Furthermore the presence of multiple lesions in the knee makes eliciting signs specific to any one condition more difficult resulting in missed diagnoses. Conclusions Clinical examination is a useful tool in diagnosing knee pathologies. In Mulago, the accuracy of clinical examination for knee pathologies among the referring physicians is high. There are however a significant proportion of knee pathologies that are missed by clinical examination hence the need to strengthen training of medical personnel in diagnosis of knee derangements so as to reduce the missed diagnoses. References
Copyright © 2010 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js10011f1.jpg] |
| |||||||||

{kind=link}