 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 15, No. 1, Mar-Apr, 2010, pp. 81-86 Tracheostomy Decannulation: Suprastomal Granulation Tissue in PerspectiveFasunla JA, Aliyu A, Nwaorgu OGB, Ijaduola GTA Department
of Otorhinolaryngology, University College Hospital, Ibadan. Nigeria Code Number: js10013 Background: Suprastomal granulation tissue is a complication of tracheostomy which may make
decannulation difficult and presents a therapeutic challenge to the
Otorhinolaryngologists. The aims of this study therefore were to evaluate
tracheostomy in black African population, determine the prevalence of
suprastomal granulation tissue and provide updated information on it that will
enable the otorhinolaryngologists to better understand and manage the lesion. Introduction Tracheostomy is a life-saving surgical procedure which is indicated, more often, in relieving upper airway obstruction1. Other indications include mechanical ventilatory support especially in critically ill patients, tracheobronchial toileting and protection of lower respiratory tract from secretions during some head and neck surgical procedures or in a patient with risk of aspiration1,2. Although the increased use of tracheostomy has prevented many deaths from diseases which formally were inevitably fatal, it is not without challenges of complications. Suprastomal granulation tissue is a significant complication of tracheostomy1. It is an exophytic growth of granulation tissue at the tracheostome. It narrows the tracheal airway lumen, leading to recurrent pulmonary morbidity and difficulties with decannulation2. In the long term, an excessive or circumferential suprastomal granulation tissue may result in tracheal stenosis3. Although patients wearing tracheostomy tube desire decannulation at the earliest possible time, obstructive suprastomal granulation tissue will make this unsuccessful. This usually presents a therapeutic challenge, not only to the managing surgeons but also, to the patients wearing the tracheostomy. There is however paucity of literature on suprastomal granulation tissue as a late complication of tracheostomy among the black Africans, despite their innate tendency to develop exuberant granulation tissue4. This study therefore aimed to evaluate tracheostomy in black Africans, observe the pattern of indications and associated complications, determine the prevalence of suprastomal granulation tissue and provide updated information that will enable otorhinolaryngologists to manage tracheostomy better and prevent complications. Patients and Methods This was a 15-year retrospective review of cases of tracheostomy managed in University College Hospital, Ibadan, Nigeria between 1993 and 2007. The data collected from the medical records included demographic data, indications for tracheostomy, duration of tracheostomy, history of prior intubation, duration of orotracheal or nasotracheal intubation, frequency of tracheostomy tube changes, complications of tracheostomy, and antimicrobial usage. The results were presented in tables and simple descriptive forms. The statistical analysis was performed using statistical package for social sciences version 11. Results Two hundred and fifty six cases of tracheostomy were reviewed. There were 192(75%) males and 64(25%) females with a sex ratio (M: F) of 3: 1. The ages ranged from 2 to 68 years with a median and mean age of 36 and 43.2years respectively. The indications for tracheostomy are shown in Table 1. Of the 256 patients, 141(55.08%) had elective tracheostomy while 115(44.92%) had emergency tracheostomy (within 24 hours of presentation to the hospital). Of the 74 patients with laryngeal tumours, 65 (87.84%) were malignant tumours while the remaining 9 (12.16%) were benign tumours. Only the malignant cases had permanent tracheostomy as part of the treatment for their oncologic lesions. Of the 191 patients who had temporary traditional surgical open tracheostomy, 133 (69.63%) patients had prior orotracheal intubation for a period of 10 – 21 days before tracheostomy was performed. The remaining 58 (30.37%) had orotracheal intubation for less than 10 days or no prior oro- or naso-tracheal intubation. The duration of temporary tracheostomy ranged from 2 weeks to 4years in all the cases. Cuffed portex (polyvinyl chloride) tracheostomy tube was used initially for all the patients and 214 (83.60%) patients had their tube changed from cuffed to plain portex tracheostomy tube (with inner tube) within 48hours post surgery. Table 1. Indications for tracheostomy
Table 2. Complications of tracheostomy
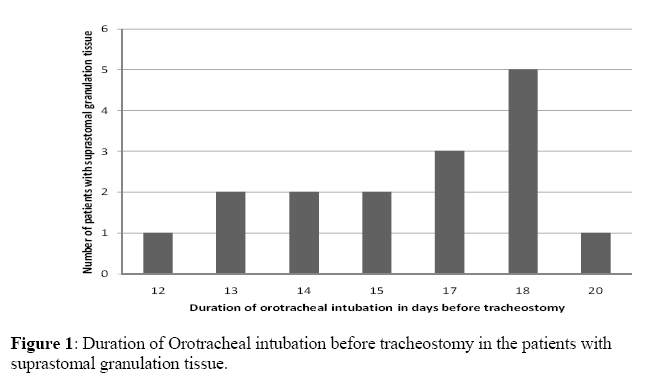
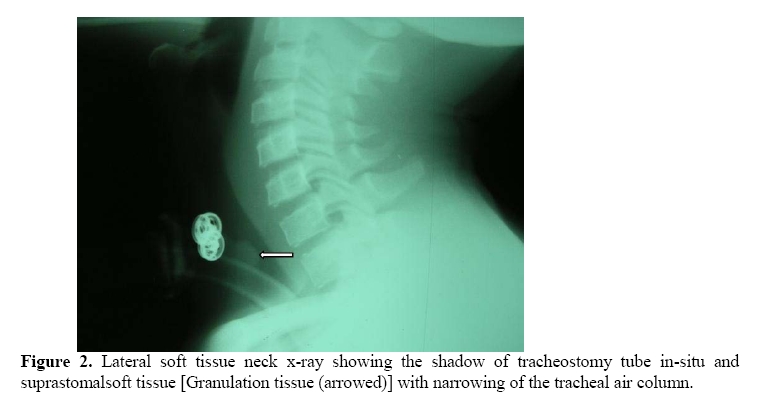
One hundred and sixty-two (63.28%) patients had their plain tube replaced or changed to a new one within two weeks of insertion. Three (1.17%) patients had premorbid history suggestive of gastritis. All the patients had prophylactic antibiotics post-operatively. Eighteen (7.03%) patients had difficult decannulation and this accounted for 60% of the complications. The complications observed are as shown in Table 2. Suprastomal granulation tissue was found in 14 (5.47%) patients and this accounted for 77.78% of cases of failed decannulation. All these patients had prior orotracheal intubations for 12 – 20days (Figure 1). The indication for tracheostomy in these patients with suprastomal granulation tissue were Severe head injury [12(85.72%)] and Tetanus [2(14.28%)]. Surgical decannulation was performed successfully in these patients. Difficult decannulation was also experienced in two patients with tracheal stenosis. Eleven (4.30%) patients had stomal infection and microbiological cultures from their tracheal swabs grew Staphylococcus aureus in 2(18.18%), Pseudomonas aeruginosa in 3(27.27%), Klebsiella spp in 1(9.09%), mixed organisms in 5 (45.45%) cases [Klebsilla spp and Staphylococcus aureus in 2(18.18%) and Staphylococcus aureus and Pseudomonas aeruginosa in 3 (27.27%)]. Discussion Tracheostomy is not psychosocially acceptable to patients because of the difficulty with phonation and the stigma associated with it by some uninformed people. Therefore, most patients with tracheostomy desire decannulation before being discharge into the community from the hospital. This decannulation process may sometimes be difficult especially in patients who had developed complication like suprastomal granulation tissue. Suprastomal granulation tissue is a late complication of tracheostomy that requires both preventive measures and surgical therapeutic methods for its successful management. Before a patient is considered for decannulation, it must be clinically and radiologically established that the concomitant airway lesion or the indication for which the tracheostomy was performed is no longer present. This should be followed by tracheostomy tube downsizing and then capping after 24hours if downsizing is tolerated. If the patient can maintain adequate ventilation over a 12 to 24 hours period with the tube capped, complete removal of the tracheostomy tube from the trachea is carried out and the stoma dressed with sterile gauze or stomal edges sutured together to achieve immediate closure5,6. This procedure may not be tolerated in a patient with obstructive suprastomal granulation tissue. The degree of granulation tissue formed during the process of wound healing varies from one individual to another. Formation of exuberant granulation tissue is due to an aberrant prolongation of the phase of granulation tissue formation in wound healing7. Factors such as foreign bodies, casts, chronic inflammation, wound location and motion, tissue involved, breed and repeated iatrogenic trauma have been implicated7. Polednak mentioned in his work that the blacks are more susceptible to form exuberant granulation tissue during wound healing4. Unfortunately, this study has no data to support and substantiate racial predisposition to formation of suprastomal granulation tissue. A comparative, prospective study of the black Africans and non-African subjects on suprastomal granulation tissue is however desirable. Fourteen (7.33%) of the 191 patients who had temporary tracheostomy developed suprastomal granulation tissue and this caused difficult decannulation. The indications for the tracheostomy in these patients were severe head injury [12(85.72%)] and tetanus [2(14.28%)]. The male preponderance with severe head injury may be due to the fact that males are more involved in risky, outdoor jobs and activities which make them usually more susceptible to injuries. All these patients with complication of obstructive suprastomal granulation tissue had prior intubation with polyvinyl chloride cuffed orotracheal tube for 12 – 20 days in the intensive care unit of our hospital before tracheostomy. There is a significant correlation between the duration of prior orotrachael intubation and suprastomal granulation tissue formation (p < 0.05%, p=0.000). Having orotracheal tube insitu for more than 2 weeks has been identified and implicated as a predisposing factor to tracheal stenosis, suprastomal and infrastomal granulation tissue formation8,9. The use of an appropriate size endotracheal tube will reduce the risk of developing any of these complications. Also, rough intubation by an inexperience anaesthetist or use of an inappropriately large size cuffed tube could cause a tear of the laryngotracheal mucosa. This may heal with polyp or exuberant granulation tissue if the mucosa overlying the cricoid cartilage was involved3,8-10. Tube granuloma is developed. The granulation tissue may then project into the laryngotracheal lumen and narrow the airway. When tracheostomy is in-situ, this will be unnoticed until during decanulation process which becomes difficult. An unconscious, critically ill orally-intubated patient may bite on or chew the tube during recovery thereby rubbing it on the mucosa. This may cause a tear of the mucosa, with resultant polyp or granulation tissue formation. A patient with severe tetanus may also have similar presentation during uncontrolled spasm. None of the patients who had prior nasotracheal intubation developed suprastomal granulation tissue or tracheal stenosis. When pre-tracheostomy intubation is desirable, we recommend naso-tracheal intubation with appropriate size tube especially in patients with severe head injury or severe tetanus not on muscle relaxants. The incidence of tetanus in the community however could be reduced by having a working policy of antitetanus immunization according to World Health Organization. Mechanical irritation and laryngopharyngeal reflux have been documented as critical factors in formation of suprastomal granulation tissue, subglottic and tracheal stenosis11,12. Polymicrobial colonization of laryngotracheal stents and tracheostomy tube by microorganisms such as Streptococci viridians, Streptococcus pneumonia, Klebsiella pneumonia, Neisseria species, Haemophilus influenza, Pseudomonas aeruginosa, Staphylococcus aureus etc have been reported. These organisms have been implicated in causing infection and inflammation around the tube, thereby promoting excess granulation tissue formation2,13-16. The organisms and /or their toxins continually irritate the wound leading to delayed wound healing. Three (18.75%) of the patients with severe head injuries who developed obstructive suprastomal granulation tissue had associated stomal infection. The organisms cultured from the tracheal swabs of these patients were similar to what had been previously reported. Although tracheostomy supposes to be a clean wound, we recommend that the stoma of the patients should still be routinely examined for evidence of infection. If this is present, early treatment with the appropriate antibiotic will reduce the risk of granulation tissue formation. The patient’s tracheostomy tube and tracheostomy dressings should be changed as frequently as required. Yaremchuk reported that if the tracheostomy tube is changed every two weeks, suprastomal granulation tissue formation may be prevented17. Tracheostomy tubes are expensive and also, not readily available in our community hence our patients cannot afford to have their tubes changed or replaced as frequently as he has recommended. This may be the reason while some of our patients developed suprastomal granulation tissue readily. Although only 3 (1.17%) of these patients had history suggestive of gastritis, none of them developed suprastomal granulation tissue. Gastroesophageal reflux has been reported has an important factor in the development of subglottic stenosis and hence, suprastomal granulation tissue10. The use of prophylactic proton pump inhibitor in all patients that had endotracheal intubation or tracheostomy for severe head injury and/ or tetanus for more than ten days will be an important part of their management protocol. Good surgical techniques which avoid the cricoid cartilage will minimize the risk of suprastomal granulation tissue formation18. The management modality of an obstructive suprastomal granulation tissue begins with investigation to confirm the presence of the lesion. In our centre, lateral soft tissue neck X-ray is usually done and the presence of a suprastomal soft tissue shadow which narrows the laryngotracheal air column is suggestive (Figure 2). Thereafter, flexible, optical direct laryngoscopy is performed to assess the suprastomal airway and confirm the presence of granulation tissue, its location and extent. Obstructive suprastomal granulation tissue requires operative intervention for its removal in order to re-establish a patent tracheal airway and successful decannulation. Various methods or techniques have been used. These include microlaryngoscopy and translaryngeal laser excision19, translaryngeal forceps excision or mechanical debulking, electrocautery, cryotherapy and trans-stomal endoscopically - guided excision with rongeurs4. The microdebrider, which is a powered rotary dissection device with suction assistance, is also effective in the removal of suprastomal granulation tissue20,21. In our centre, debulking of the obstructive suprastomal granulation tissue is performed during microlaryngoscopy by using trans-laryngeal forceps and electrocautery. The excision of the tracheostomy tract with any granuloma is also performed. There is no facility for laser excision or microdebrider in our centre. In cases of recurrence after excision, the patient would have the trachea splinted with an indwelling nasotracheal stent for 3 - 7 days after a repeated excision. This surgical decannulation protocol is similar to the practice reported by Al-Saati et al in children22. The stoma edges can be freshened and sutured together after the removal of tracheostomy tube in order to achieve secondary closure. Adjunct steroid therapy is also given. There were 3 patients that developed subglottic stenosis and could not be decannulated using this treatment method. Conclusion Suprastomal granulation tissue is a notable complication of tracheostomy but can be prevented with good surgical technique, sparing the cricoid cartilage during dissection. Stomal infection should be promptly treated and cuffed orotracheal intubation for more than a week in unconscious and tetanus patients should be avoided. References
Copyright © 2010 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js10013f1.jpg] [js10013f2.jpg] |
| |||||||||

{kind=link}
{kind=link}