 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 15, No. 1, Mar-Apr, 2010, pp. 96-101 Hearing Disorders in HIV-Positive Adult PatientsB.A Ongulo, H.O Oburra Department of Surgery, Kenyatta National Hospital Nairobi, Kenya. Code Number: js10016 Background: This study was aimed at determining the prevalence
and type of hearing disorders in HIV positive patients and any correlationship
with the CD4 counts/stage of HIV/AIDS in patients attending the comprehensive
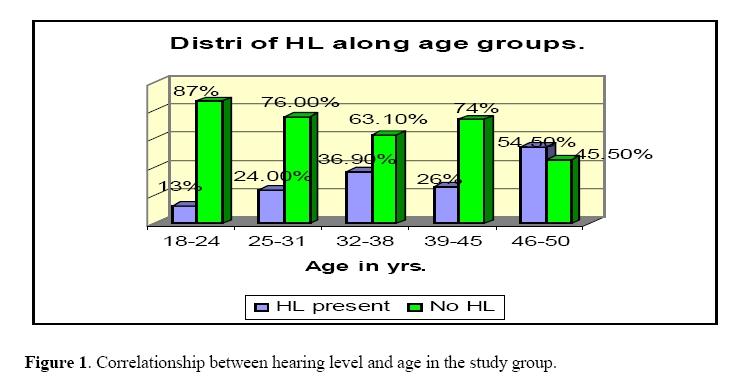
care clinic (CCC). Introduction Over 50% of HIV infected patients present first to the otorhinolaryngologist1. Of all the otorhinolaryngological manifestations, otological symptoms comprise at least 62%, yet many care-givers are unaware of these otological symptoms hence they are more likely to concentrate on other manifestations2, 3. Somefun et al3 looked at 98 patients at Lagos University teaching hospital and found that while only 17% of the patients were referred because of otorhinolaryngological (ORL) diseases, 80% of them actually had ORL/head and neck conditions. Numerous international studies have demonstrated a relationship between HIV/AIDS and auditory function. Kohan et al2 conducted a 5-year retrospective study to evaluate otologic disease in patients with AIDS at New York university medical center- Bellevue hospital. They found that 62% had hearing loss 2. Marra et al4 did a case control study of 99 HIV positive patients at the university of Washington HIV based clinic and found that 29% of the patients had hearing loss4. Hearing disability compromises the overall economic productivity of an individual and may render one an outcast. In HIV positive patients who are still stigmatized, it can lead to marked reduction of quality of life. In this study, the nature and degree of hearing disability in HIV infected patients presenting at CCC were determined. This will raise the awareness of care-givers and eventually improve the quality of life and productivity of HIV/AIDS patients. Patients and Methods This was a hospital based case control study done between January and April 2007, at the comprehensive care clinic and voluntary counseling and testing centre. A minimum sample size of 115 was required in each arm. The study subjects were adult HIV positive patients not on antiretroviral drugs aged between 18 and 50years recruited into the study from the CCC clinic whereas the controls were HIV negative subjects who were age and sex matched recruited from VCT centre. Patients who suffered diabetes, meningitis, head injury or cerebrovascular accident and those who had exposure to ototoxic medications were excluded from the study. Written informed consent was obtained from the subjects. Approval to carry out this study was obtained from the Ethics and Research committee of Kenyatta national hospital. A clinical history was taken followed by thorough physical examination, otoscopy and tuning folk tests, PTA and tympanometry. The WHO staging of the HIV disease and CD4 cell count were carried out in the study subjects. CD4 count was determined by the automated flow cytometry analyzer, FASCOUNT (benedict dick, USA). Data analysis was done using SPSS version 10.0 software and descriptive statistics were done. Results The study group comprised of 194 subjects who were HIV positive but not on ARVs and the control group were 124 subjects who were HIV negative. In the study group, males were 75 (38.7%) while females were 119 (61.3%). In the control group, males were 47 (37.9%) and females were 77 (62.1%). The age and sex in both the study group and the control were similar because they were matched for age and sex. The age ranged from 18 yrs to 50 yrs in both the study and control groups with a mean age of 36.09 and 36.4 yrs respectively and the median age as 35 yrs and 36 yrs respectively. The mode was 37 in both groups. Most of the patients were between 32 yrs to 38 yrs old. As seen below (table 1), the hearing loss was 33.5% in the study group and 8.1% in the control group. This is statistically significant. There was no gender bias in hearing loss. The hearing level when computed according to age groups showed that hearing loss worsens with increasing age as shown in Figure 1. This was statistically significant (P=0.022). Table 1. Hearing Loss in the Study and Control Groups.
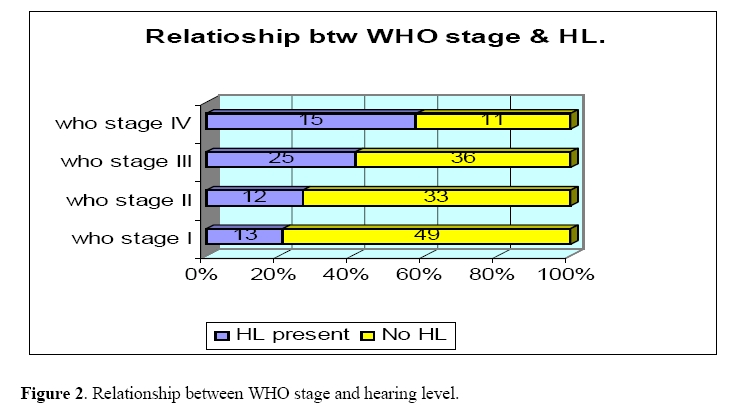
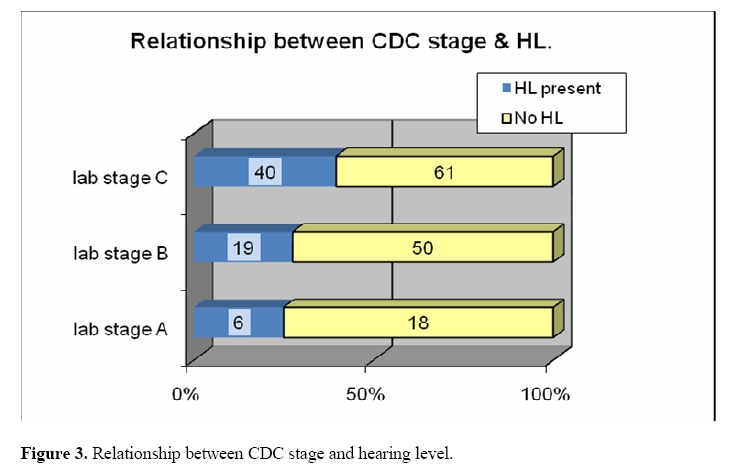
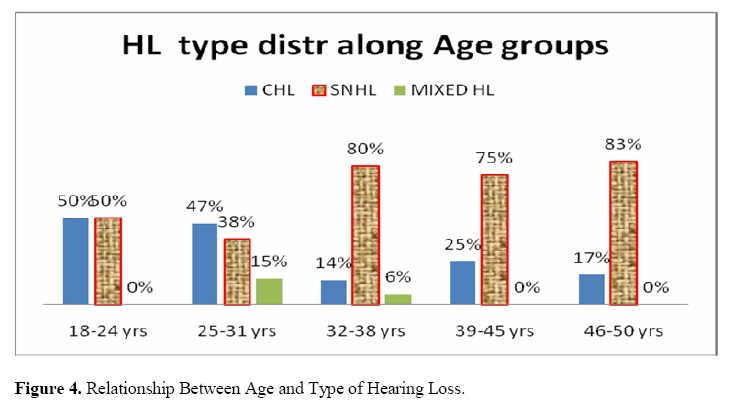
The subjects were classified according to the WHO clinical staging for retroviral disease and the hearing level determined. Results indicate that hearing loss worsens as the WHO clinical stage of the disease advances as shown in Figure 2. This was statistically significant correlation (P=0.004). The worsening of hearing level with advancement of the HIV disease was likewise confirmed when the CDC stage was correlated with the hearing level as shown in Figure 3. When the nature of hearing loss was assessed, it was found that 74% had SNHL, 22% CHL and 4% had mixed HL. As the age advances, the proportion of subjects with CHL decreases but those with SNHL increases as shown in Figure 4 below. Dscussion Hearing loss is a cardinal feature and disability in HIV/AIDS patients. In this study, 33.5% of HIV positive patients not on ARVs had hearing level above 25 dB in at least one of the hearing frequencies compared to only 8.1% in HIV negative normal subjects. Soucek and Michaels5 got 39% in a sample size of 65 subjects and Wang et al6 got 45.5% in a sample size of 350. There is a wide variation found in different studies and this could be due to the sample size and the cut off decibel for hearing loss. It has been shown that HIV positive subjects are at a higher risk of developing a hearing loss. Mandela in her study of the effect of streptomycin on the cochlear found that HIV positive patients on streptomycin are at a higher risk of sustaining sensorineural hearing loss than HIV negative patients on the same treatment7. Many other drugs commonly prescribed to treat various opportunistic infections as well as ARVs have been implicated in causing hearing loss4,8. This study found no difference in the HL according to gender. In both sexes, 33.45 % had a HL. This suggests that the sex of the subject does not play any role in the causation of hearing loss but males are the ones who mostly work in noisy environments and are therefore predisposed to noise induced hearing loss, however, such patients were excluded from the study. The HL gets worse with advancement of age and this was found to be statistically significant P<0.05 (0.022). Marra et al4 also got a similar finding. In this study, patients over 50 yrs of age were excluded to avoid the effects of presbyacusis since it is a known fact that as one ages, HL gradually develops especially after the age of 60 yrs. The elderly subjects in this study comprised the majority with HL compared to the younger population, this may indicate that HIV has more adverse effects on the hearing apparatus in the elderly population9, but this needs to be proved beyond question in a suitably designed study with hearing loss corrected for presbyacusis. The number of subjects with a HL increases with advancement in the WHO stage of the disease. This was statistically significant and it could be due to the effect of the HIV virus on the cochlear10, middle ear infections11 or CNS complications5. Patients with advanced HIV disease are more predisposed to infections including those that interfere with hearing. Michaels et al found that 60% had features of otitis media in temporal bones of patients who succumbed to HIV11. This may account for the increase in HL with advancement of HIV disease stage. Subjects who had HL mostly experienced SNHL (74%) followed by CHL (21.5%) and mixed HL (4.5%) was the least. Mild HL (26-40 dB) was the most common at 70% followed by moderate HL (24.5%), moderate severe HL (4.5%) and severe HL was 1%. There was no profound HL in the study population. This is the same trend found by Soucek5. The possible causes of HL in HIV disease could be divided into three, those due ototoxic drugs administered to these patients, CNS effects of the virus including CNS infections and tumours e.g. toxoplasmosis, meningitis, CMV, tuberculosis and lymphoma, and lastly the effects of the virus on the cochlear. Michaels et al found reduced otoacoustic emissions due to hair cell loss in temporal bones of HIV infected patients11. The higher frequencies i.e. 4 KHz and 8 KHz are the most affected while the middle frequencies are largely spared. Similar findings were gotten by Soucek5 where 6 KHz and 8 KHz were the most affected. This is thought to be due to changes in the cochlear mechanics5. Subjects with CD4 cell counts below 200/µl had the highest proportion of those with HL at 38%, followed by those with CD4 cell counts between 200 and 500/µl at 28% and those whose CD4 cell counts were above 500/µl at 22%. This means that as the CD4 cell count falls, the chance of developing a hearing loss increases. The absolute CD4 cell count was found to be statistically related to the development of a HL. Kohan and Giacchi12 found that the more immunocompromised AIDS patients had more advanced otologic disease. The markedly lower incidence of otitis media of 8% overall found clinically5 compared to that found at autopsy of 20% 11 might suggest that severe otitis media is a late terminal manifestation of AIDS, this supports the finding of HL being more common in advanced disease. Conclusion
References
Copyright © 2010 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js10016f2.jpg] [js10016f3.jpg] [js10016f1.jpg] [js10016f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}