 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 15, No. 1, Mar-Apr, 2010, pp. 102-110 Pattern of Surgical Diseases Based on Histopathological Findings: A 13-years Personal Experience in a Rural Hospital in KenyaP.M. Nthumba Department of Surgery, AIC
Kijabe Hospital – Kenya. Code Number: js10017 Background: Church/mission hospitals and other non-government health institutions in Kenya
provide 30% of the healthcare needs, providing affordable care to the rural
poor. This review presents the surgical pathology to which a general surgeon
working in a rural Kenyan hospital is exposed through training and beyond.
Additionally, some of the rarer surgical pathology, ‘rare birds’, encountered
during this period is
reported. Introduction Church/mission hospitals constitute most of the non-governmental health institutions that provide 30% of healthcare in Kenya. Many struggle to provide affordable care to the rural poor that they serve, and are largely dependent on foreign donor support. Church hospitals are administered by a local indigenous church, while mission hospitals are wholly administered by foreign organizations. Until 1995, these health institutions were not involved in medical education beyond elective terms for medicals students. The Ministry of Health, Government of Kenya (MOH), was the only institution at the time that provided employment with an assured sponsorship for post-graduate training, discouraging most Kenyan doctors from working in church/mission hospitals. These institutions were therefore forced to continue depending on missionary doctors, with a number collapsing upon the departure of these missionaries1. In 1995, the Kenya Medical Practitioners and Dentists Board (MPBD) approved medical internship training in 3 church hospitals. The same year, the MOH sent medical interns to these hospitals; the current author was one these. Subsequently, along with the internship program, some of these institutions became training sites for the Family Practice post-graduate program offered by Moi University, Eldoret. Training in general, orthopedic and pediatric surgery, under the auspices of the College of Surgeons of East, Central and Southern Africa (COSECSA); Pediatric surgery training under the Pan African Academy of Christian Surgeons and a general surgery rotation for University of Nairobi registrars are additional programs that evolved between 2004 and 2008. Thus training programs and surgical career development opportunities in some of these institutions have opened opportunities for training of more surgeons, as well as provided an impetus for improved surgical care in rural hospitals. The AIC Kijabe hospital has a well-developed surgical service, with a supporting Pathology department that also provides pathology services to 70 other hospitals in Kenya and the surrounding region. It processes more than 4500 specimens annually, and has maintained computerized pathology records since 1992. The main objective of this review was to present the range of surgical pathology handled by a single doctor from internship, and through training and practice in general surgery, while working in a rural Kenyan hospital. This review also reports on some of the rarer surgical pathology encountered over this period. Patients and Methods A retrospective review of pathology records of all the specimens submitted by the author between 1995 and 2008 was done. Data extracted from the Pathology department database included patient name, age, sex, clinical history, macroscopic description, microscopic description, diagnosis and comments. Although all the patients whose records were retrieved had been managed by the author, for the purposes of reporting, the records were then divided into the different specialties under which they would fall in large teaching centers: urology, general surgery, gynaecology, maxillofacial/otolaryngology and ‘others’. Some of the rarer pathologies encountered in each specialty are reported as ‘rare birds’, and briefly discussed. A search of the internet, including Pubmed and Medline databases did not yield comparable studies: a single author experience, detailing the surgical experience from internship through training in general surgery and beyond. Results A total of 1826 specimens were taken and submitted for histological examination during this period (Table 1). In 747 (44.8%) of the cases the specimens were from from females and 919 (55.2%) were from males. The constituted only about 25% of the surgical specimens but included all the prostate and appendix specimens. About 3.6% of the specimens analyzed had no abnormality, and it could be argued that this was unnecessary expenditure on the part of the patients. The converse however, is also true: some specimens not submitted may have had significant pathology and thus these patients failed to benefit fully the surgical intervention. Submission of specimen for analysis was for many years dictated by the clinical impression and the ability of the patient to pay for the examination, leading to a relatively low submission; transformation into a training institution has led to a reduction of dependence on clinical judgment and intuition. Specimens submitted in the first 6 years (Table 1) represented 18.5% of the total: these initially consisted of minor procedures, such as bone marrow aspirates and lymph node biopsies, with a gradual increase in variety and complexity of cases, drawn from different specialties (Table 1, 2 and 3). General surgical specimens constituted 48.4% of the total, while urology, gynaecology, maxillofacial/otolaryngology and ‘other’ specialties made up 34.6%, 7.8%, 6.7%, and 2.5% respectively (Table 3). Primarily cardiothoracic, neurosurgery and orthopedic specimen were grouped together under ‘others’ (Table 2). Table 1. Number of Specimens Submitted Between 1995 and 2008.
Total number of specimens submitted for histopathology between 1995 to 2008. Few or none were submitted during periods of training (1995, end of1998 to beginning of 2002, and mid-2006 to mid-2009). Table 2. Specialties grouped under ‘others’
Table 3. Specimen totals by specialty
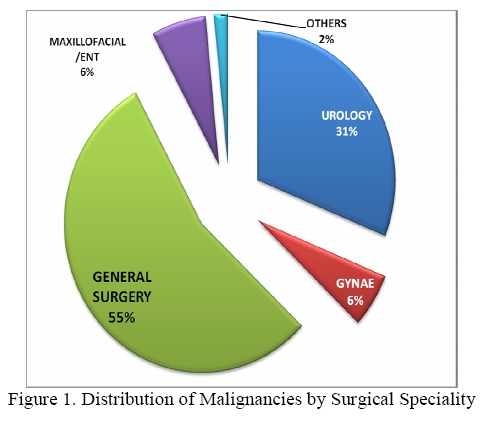
Table and pie chart of specimen totals by specialty. Specimens labeled ‘intermediate’ had dysplastic features, but no frank malignant features. Table 4. ‘Rare birds’. The Rare Conditions
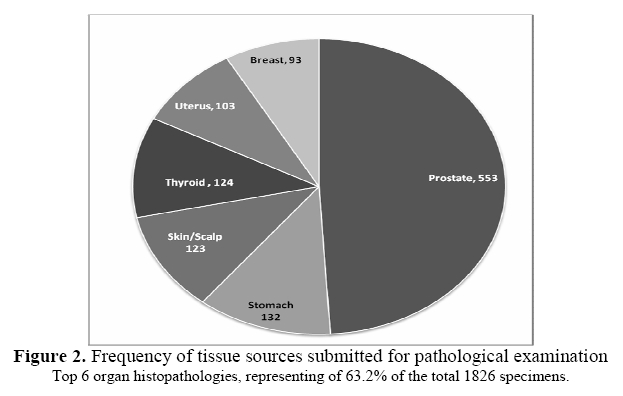
There were a total of 389 (21.3%) malignancies. Of these, 55% were in general surgery and 31.1% in urology. General surgery had the highest incidence (24.2%) of malignancy; maxillofacial/otolaryngology, urology, gynaecology, and ‘others’ had rates of 20.5%, 19.1%, 16.2%, and 13%, respectively (Table 3 and Figure 1). The prostate constituted the 30.3% of all organ pathologies (Figure 2). Rare Conditions in different specialties General surgery General surgery is an expansive specialty in rural Africa, and crosses into areas otherwise managed by different specialties in other environments. For the purposes of this review, gastrointestinal, pancreaticohepatobiliary, skin/scalp, thyroid and breast pathologies were classified under general surgery, totaling 838 specimens. Thyroid malignancy, hyperplastic and multinodular goiters made up 8.9%, 20.2% and 29.8% of thyroid lesions, respectively. One thyroid tumor was reported as tuberculosis; the patient had no evidence of tuberculosis elsewhere in his body. There were 60 appendectomies performed by the current author over the 13 years covered in this review, an average of five cases per year. Twelve (20%) had no histological abnormalities; 44 had appendicitis, while four had other pathologies, including carcinoid tumor, mucocele, adenocarcinoma and a periappendicitis. One case of acute appendicitis was associated with Taenia species (Table 4). Of 18 duodenal biopsies, three were malignant – two with high grade adenocarcinomas, and one a large cell malignant lymphoma. Amongst rare skin pathologies encountered was a large posterior trunk ulcer in an HIV negative patient that was reported as Kaposi’s sarcoma (Figure 1). A 55-year old female presenting with extensive keloids covering most of her body, simulating post-severe burn sequelae, was found to have acne conglobata on histopathology (Figure 2). A biopsy from another patient with a facial ulcer was reported as skin tuberculosis, acne vulgaris. Biopsies from a two year-old child with bilateral lower extremity lymphedema and abdominal masses were reported as lymphangiomatosis; an accompanying CT scan confirmed a diagnosis of systemic lymphangiomatosis. Urology Urology takes up a significant portion of the general surgeon’s practice in our environment, mostly as prostate pathology, which made up 87.4% of the urology specimens – 30.3% of the total specimens, in this review. ‘Rare birds’ included two cases of tuberculous prostatitis and one of spindle cell sarcoma of the prostate. Two females presented in acute urinary retention; both were found to have adenocarcinoma of the urethra on histopathology. Maxillofacial surgery A 61 year-old patient underwent a maxillectomy for a maxillary tumor; microscopic examination revealed a plasmacytoma, hence a clinical diagnosis of solitary plasmacytoma. A fine needle aspirate of a parotid nodule in a patient with a history of a previous parotidectomy that had been reported elsewhere as pleomorphic adenoma was found to be an adenocystic carcinoma, with a chest radiograph revealing canon-ball lesions. Orthopedics A patient presented with a large proximal leg mass with common peroneal nerve palsy; the excised tumor turned out to be a lipoma of the fibula. Another patient with progressive median nerve weakness and a forearm mass was found to have an intramuscular lipoma. Discussion Poverty and illiteracy, two vicious ills that bedevil rural communities, prevent healthcare-seeking behavior amongst the populace. Additionally, infectious diseases like malaria, pulmonary tuberculosis and HIV have permanently taken center-stage of both government and donor-support health policy and priority, relegating surgical diseases to the periphery1. Sustaining the provision of affordable health care to the rural patients such as the one the AIC KH serves continues to be demanding, and a cost-benefit consideration must be made before any given test, procedure or service is offered. Submitted specimens reflect a bias peculiar to our institution. Like many other church/mission hospitals in Kenya, general surgeons initially had to manage patients of different surgical specialties; however, in the last six years, AIC KH has developed well-staffed pediatric surgical, orthopedic, gynaecology and obstetrics departments to optimize care in these different specialties. While the current author’s preference was reconstructive surgery2,3 and the high-volume urology service was equally shared amongst three general surgery units4, one of the surgeons handled most of the breast pathology, reported elsewhere5. Many of the unusual pathologies encountered in this review form excellent bases for case reports6,7, but were reported in this review in order to give a complete account of the rich surgical pathology encountered in clinical practice in our environment. General surgery Thyroid cancer, hyperplastic and multinodular goiters made up 8.9%, 20.2% and 29.8% of thyroid lesions, respectively a previous study from the same institution found these to be: 11.7%, 13% and 47% respectively8. While the current study concentrated on the work of a single surgeon, previous studies reflect the work of the entire institution, and may be the reason for the discrepancy of results. Primary tuberculosis of the thyroid is a very rare disease, even in endemic regions9. Postmortem studies suggest rates of between 0.003% and 0.1%; with higher rates in military TB. This review found one patient with primary thyroid tuberculosis. Appendicitis in our setting is lower than that reported from urban settings, with an average of five appendectomies per year; consistent with an earlier report from our institution of 112 patients over a 5-year period10. Taenia species (adults and eggs), the cause of one case of acute appendicitis, is a very rare presentation11. The incidence of African/endemic Kaposis’ sarcoma (KS) is uncertain in the current era of epidemic HIV, however it is relatively rare. One of the patients was HIV-negative patient and had a huge ulcer reported to be KS (Figure 1). The most common type of KS is the epidemic (AIDS-related) type. Endemic or African KS generally affects patents younger than 40 years, and in children may present with an aggressive form. Other types of KS include the classic (Mediterranean) KS and the Iatrogenic (transplant-related or immunosuppressive therapy) KS12,13. The patient reported here had a giant aggressive variant of the endemic KS. Duodenal malignancy is rare – two adenocarcinomas and a lymphoma were found in three patients. Adenocarcinoma of the duodenum is quite rare, representing 0.5% of all gastrointestinal (GI) malignancies14. The two cases reported here represented 0.75% of all the GI malignancies in this review. Malignant lymphomas of the duodenum are similarly rare. In a review of 117 GI lymphomas, there was none from the duodenum15. Acne conglobata, found in one patient in this review, is the most severe form of acne, a rare chronic nodulocystic dermatological disorder that presents with comedones, pustules, abscesses and draining sinuses, most commonly in the face, arms, back and thighs16. Progressive scarring is due to repeated infections, and may cause severe disfigurement from the resultant keloids, leading to social isolation and functional impairment. It usually affects males17. This is the first report of acne conglobata from Africa, and likely the most severe case reported to date. Cutaneous tuberculosis is rare, representing about 0.2% of all dermatologic cases, and about 0.14% of all tuberculosis disease18. The clinical diagnosis in the patient reported here was lupus vulgaris. Systemic lymphangiomatosis, as reported in a child in this study, is a rare condition characterized primarily by skeletal system angiomatous lesions; concomitant skin, soft tissue and visceral involvement occurs in 50% of the cases is associated with poor prognosis19. Although benign, progressive growth of the lesions may cause pathological fractures of bones or cause compression of vital structures. Urology Of the 553 prostates examined, 19.7% were malignant; of these, adenocarcinomas constituted 97.2%. A previous study on suprapubic prostatectomies in the same institution found a 6.7% incidence of prostate malignancy4. While the current study included all prostatic specimen (including biopsies), the earlier study looked only at prostatectomy specimens, hence the apparent discrepancy in malignancy rates. Rare prostatic histopathologies included two patients with primary tuberculous prostatitis, a rare condition usually diagnosed histologically, after prostatectomy20. The high grade spindle cell sarcoma of the prostate represented 0.09% of all prostatic cancers in this review; adult prostatic sarcomas constitute less than 0.1% of all prostatic malignancies, in most studies21. Adenocarcinoma of the female urethra was found in two patients. Female urethral adenocarcinoma represents 0.02% of all female malignancies; most are at an advanced stage when first diagnosed22. Radical cysto-urethrectomy with uretero-sigmoidostomies was performed for both. Maxillofacial surgery Solitary bone plasmacytoma of the maxilla is a rare neoplasm. It most commonly affects males aged 50 to 60 years, with the male to female ratio of 3:1 23. Our patient, a female, had no evidence of systemic involvement. Adenoid cystic carcinoma of salivary glands constitute 10% of all the neoplasms of salivary glands. They are associated with poor prognosis due to local recurrences and distant metastases, usually pulmonary24. An initial misdiagnosis and an incomplete excision of the lesion most likely led to the ‘recurrence’ and metastases. Intra-osseous lipomas are rare lesions, accounting for less than 0.1% of all bony lesions. They affect both the axial and appendicular skeleton, and are found most frequently in the metaphysis of long bones, especially the proximal femur25. Pathological fractures and malignant degeneration have been reported26. In the patient reported here, cosmesis and common peroneal nerve compression were the main problems. Only unusually located lipomas or those of doubtful pathology were submitted for histological evaluation. Intramuscular lipomata are rare tumors, accounting for 1.8% of fatty tumors. These lesions are even rarer in the forearm; only three previous cases have been reported in English literature27-29. The patient reported here had median nerve paraesthesia that improved after surgery. Conclusion Church/mission hospitals provide a significant contribution to healthcare provision in Kenya. Training programs and surgical career development opportunities in some of these institutions have opened opportunities for training of more surgeons, as well as provided an impetus for improved surgical care in rural hospitals. A surgical career in these institutions, though demanding because of the breadth of pathology, is a rewarding educational experience, as reflected in this review. Acknowledgements The author is grateful to AIC Kijabe Hospital Pathology Department for the pathology specimen results. References
Copyright © 2010 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js10017f1.jpg] [js10017f2.jpg] |
| |||||||||

{kind=link}
{kind=link}