 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 15, No. 1, Mar-Apr, 2010, pp. 111-118 Cardiac Surgery: One Year Experience of Cardiac Surgery at Muhimbili National Hospital, Dar es Salaam, TanzaniaNyawawa ETM1, Ussiri EV1, Chillo P1, Waane T1, Lugazia E1, Mpoki U1, Luchemba R1, Wandwi B1, Nyangasa B1, Bgoya J2 Mahalu W3. 1 Muhimbili National Hospital, Tanzania, Code Number: js10018 Background: Establishing a cardiac unit in developing countries is usually
difficult as it is associated with many obstacles of both expertise and
financial constraints and more alarming is the mortality rate that may be high.
Even after success in the initial stage sustainability of such program is a dilemma.The aim of this study was to determine pattern of
disease profile, type of cardiac surgery done and the overall outcome. Introduction In view of the outstanding global heart disease that is expected the world population of 6.5 billion people is at risk of heart diseases1. While the developed countries estimate a population of one billion, the majority of people (5.5 billion) are found in developing countries. With emerging economy the backlog of patients with rheumatic heart disease, congenital heart diseases are immense. There is an epidemic rise of atherosclerotic coronary heart disease due primarily notable risk factors such as hypertension, hyperlipidemia, westernized diet, smoking, inactivity and change in life style2. Fifty-seven million people die each year on the planet with over 17 million from cardiovascular disease3. Non communicable diseases are clearly a greater cause of death than communicable disease and will continue to rise4. To the emerging countries the situation is even worse as there are few cardiac centers when comparing number of inhabitants per centre (Africa 1/33,000,000 as compared to Asia 1/16,000,000 Europe 1/1,000,000 USA 1/120,000)5. To worsen the situation in the developing countries there is lack of expertise and the frequent political conflicts. Establishing a cardiac centre especially in a developing country is usually difficult and associated with many obstacles6. Pezzela7 classified cardiac projects in developing countries as ; nonexistent but wanting to start, previously existed but failed, small or even larger existing programs now limited by financial and political consideration, ready to start but need financial and political support, already functional but needing academic support and various combinations of these. Even after starting the reputation mighty be lowered with an exceedingly high mortality rate that can be anticipated that may again retards the smooth running of the unit. Sustainability of such program in emerging countries is a problem again. If not well planned even the cadres of staff mighty be inadequate. If there good success particularly with regards to number of operation and having the staff acquired good skills and experience, moving of staff to green pastures is all what is anticipated due to low payment6, 8.With exception of south Africa and Egypt a few other African countries have far made progress in open heart Surgery if not fully established yet some are doing operations in collaboration with visiting cardiac team from else where9, 10. In Tanzania earliest plan to establish cardiac unit started in early 1970s but could not mature till 2005 when strong commitment by the government was taken including sending the team of staffs to train in various institutions that had composed all various cadres of staff required to make a complete cardiac team. Further more commitment was the necessity to acquire the tools that it managed successful. Since then the team was back by 2007 and appropriate measures was taken to officially start open heart surgery that by 21st may 2008 open heart surgery started and by June 2009 a total of 105 cases had been operated. And we here present our first one year outcome of open heart surgery at Muhimbili National Hospital in Dar es Salaam. Patients and Methods This was a prospective study that recruited all patients who underwent cardiac operation between May 2008 and June 2009. Patients’ details including age, sex and duration of symptoms were taken. The diagnosis as found from echocardiography and confirmed during operation and whether there was an associated cardiac lesion was recorded; the type of operation whether done on pump or off pump was coded and recorded. The pulmonary pressure was also determined during echocardiography and quantified to whether there was pulmonary hypertension or not. The ejection fraction combined with fraction of shortening were used to assess ventricular function simultaneously the diastolic function was assessed and whether cardiac dysfunction was present or not were recorded. During operation the time of aortic cross-clamp that was categorized into short if it was less or equal to 60 minutes and prolonged when more than 60minutes, total duration of conduct of bypass that was categorized into short if less or equal to 60 minutes, moderate when 61-100minutes and prolonged when >100minutes. Operation time that was counted from skin incision to its closure was recorded and categorized into short to average time if the procedure lasted to less or equal to 4 hours and prolonged when it was more than that. Patient was followed into the ICU while closely monitored for any complication that develops. Further noted was the total duration of intensive care stay. The duration of ICU stay was categorized as early stay if it was five days or less and prolonged when it was more. The duration of hospital stay known as post intensive care hospital stay was noted at the time of discharge of the patient from the hospital. This duration was categorized into short to normal when the patient stayed for less than or equal to two weeks and prolonged when it was more. Further noted were any complication the patient develops while in the ward. The final disposition of the patient as to whether recovered fully, partially or died was also noted. Data were entered into a master data sheet and then into SPSS 11.5 window program and analyzed accordingly. Results There were 105 cardiac cases of which 22(21%) were males and 83(79%) were females making1:4 male to female ratio. The mean age was 19.4±12.3 years, range 2-52 years. The mean duration of operation was 3.1±1.0 hours ;( range 1-5.5 hours). The mean duration of aortic cross-clamp was 64.4±25.4 minutes; (range 12-176 minutes) for 72 cases. The mean duration of cardio bypass was 94.0±33.6 minutes; (range 40-240 minutes) for 72 cases. The mean duration of intensive care stay was 4.5±2.1 days; (range 2-20 days). And mean duration of post ICU hospital stay 13.7±6.6 days ;( range 5-50 days) for 94 cases. Females (79%) had more cardiac disease as compared to males (21%). Majority of patients occurred in the ages between 7-16 years. (Table 1) Table 1. Age-sex Distribution
Table 2. Pattern of group of cardiac disease
Table 3. Distribution of Cardiac Diseases
Table 4. Presence of Ventricular Dysfunction and Patients’ Outcome
Table 5. Total operation time, ventricular dysfunction and postoperative complications
*= Total operation time, §= ventricular dysfunction, CCF= congestive cardiac failure, Techn.diff= technically difficult, PVS= paroxysmal ventricular systoles, Wound inf= wound infection, ARDS= Acute respiratory distress syndrome, Para’lysis= paralysis Table 6. Total operation time and duration of ICU Stay
χ2=13.7; df 2, p=0.001 Table 7. Outcome of Management
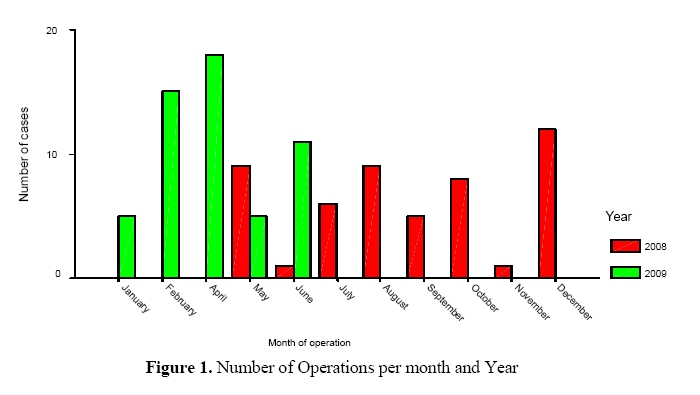
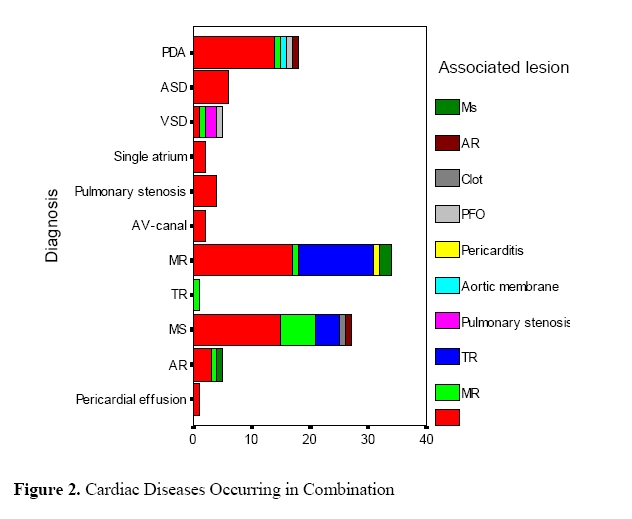
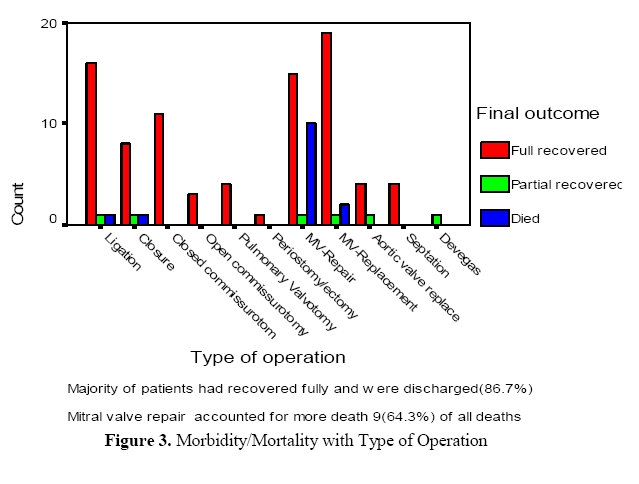
Operations started in may 2008 and we progressed to December (red bars) (Figure 1). Rheumatic heart diseases accounted for the large number of cases that were operated at the unit (47.6%) (Table 2) Mitral valve disease accounted for the majority of cardiac diseases (58.1%) (Table 3). Majority of cardiac diseases occurred with other associated cardiac lesions (Figure 2). There was statistical significant between duration of aortic-cross clamp and postoperative outcome (p<0.05). There was no statistical significant difference between patients with ventricular dysfunction and patient outcome (p>0.05). (Table 4). There was significant statistical difference between total duration of operation and emergency of complications (p<0.05) There was no statistical significant between ventricular dysfunction and postoperative complications (p>0.05) (Table 5). There was significant statistical difference between total operation time and duration of intensive care stay (p<0.01) (6) When comparing morbidity/mortality, majority of patients had full recovery and the mortality was probably within acceptable limits in a newly established cardiac centre (Figure 3). The overall mortality rate was 13.3% with 64.3% of all deaths occurring in the ICU. Nine (64.3%) of the deaths followed mitral valve repair, 3 patients died following mitral valve replacement, 1 patient died following VSD closure and one patient died following PDA ligation.(Table 7). Discussion The study showed that with initial setting of a cardiac unit in our centre majority of patients (86.7%) had fully recovery and were discharged. However the mortality of 13.3% is probably comparable to other settings11. The spectrum of cardiac disease found elsewhere is also found in our community8. Majority of our patients had Rheumatic valvular heart disease (47.6% Table 2) this high incidence noted in this study as compared to other cardiac lesions goes in parallel with the high incidence of the disease to any African country that is the result of the burden of rheumatic fever attributed to combination of lack of resources, infrastructure, political and economic instability, poverty, overcrowding and malnutrition12. Further the highest incidence of rheumatic heart disease is found in sub-Saharan Africa with a prevalence of 5.7 per 1000 as compared to 1.8 per 1000 in North Africa and 0.3 per 1000 in economically developed countries with established market economy 13, 14. Since the majority of cases were mitral valvular disease and in particular mitral regurgitation and patients who succumbed to death followed mitral valve repair it implies that mitral valve repair requires more skills and expertise. Nkomo VT, portrays that problem to valve repair or replacement for rheumatic heart disease with or without infective endocarditic in young economically disadvantaged patients are numerous12. The fulminant course of rheumatic fever, rheumatic heart disease and infective endocarditis coupled with delayed patient presentation results in a high incidence of heart failure at presentation15, associated with high in-hospital and late mortality even with surgical intervention16,17,18. Our patient had long duration of symptoms of mean 32±14 months (range 18.2-46.3) in rheumatic heart diseases and at presentation 80% were in NYHA class III and IV. Despite staying in the ward for 3 weeks to 3 months in some, for optimization of medication before surgery was undertaken, it was possible that some portions myocardial tissue could have undergone remodeling. The mere presence of suboptimal ventricular dysfunction is probably not a contraindication to cardiac operation. The duration of aortic cross-clamp and total operation time were determinant of postoperative outcome. This finding was similar to other series where ischemia time and total operation time was found to be determinant of early extubation and postoperative complications for prolonged operations 19, 20. However this study could not demonstrate any association with the total pump time. Garcia-Montes et al also could not find any similarity with total pump time while determining factors associated with prolonged mechanical ventilation in paediatric patients21. Conclusion Majority of patients who underwent cardiac surgery had full recovery. The diversity of spectrum of cardiac disease found elsewhere is also found in our community and therefore need to increase community awareness. Mitral valve repair deserve a special entity that requires skills and expertise. The mere presence of suboptimal ventricular dysfunction is probably not a contraindication to cardiac operation. The duration of aortic cross-clamp and total operation time were determinant of postoperative outcome. Acknowledgement We thank the government through Ministry of Health and Social welfare for having realized the need of its people and training the cardiac team. We also thank the administration of Muhimbili National Hospital for having supported the unit throughout the period since its establishment. We thank members of the task force who have played a big role since its early plans and for close monitoring of the project. References
Copyright © 2010 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js10018f2.jpg] [js10018f3.jpg] [js10018f1.jpg] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}
{kind=link}
{kind=link}