 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 15, No. 1, Mar-Apr, 2010, pp. 130-134 Neurocritical Care Audit in A Tertiary InstitutionO.E. Idowu1, S.O. Oyeleke2, A.A. Olaoya1 1Neurosurgery
Unit, Department of Surgery and Code Number: js10021 Background: The ‘open’ intensive care unit (ICU) predominates in most low and
middle economy societies. This is associated with paucity of personnel and
cost challenges involved for its maintenance and smooth running despite the
great public demand for this service. Data on neurocritical care in scare in
Nigeria and the subregion as a whole. Our objective is to audit our
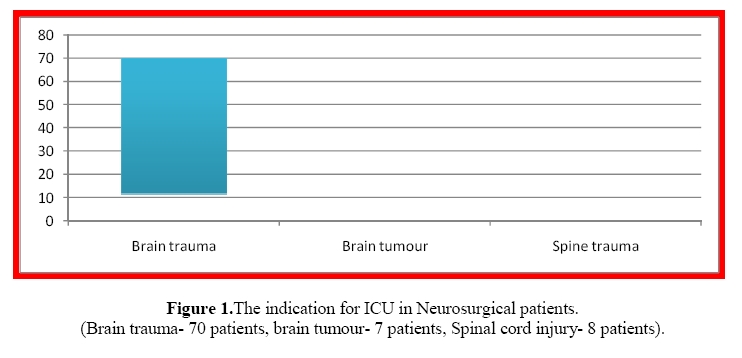
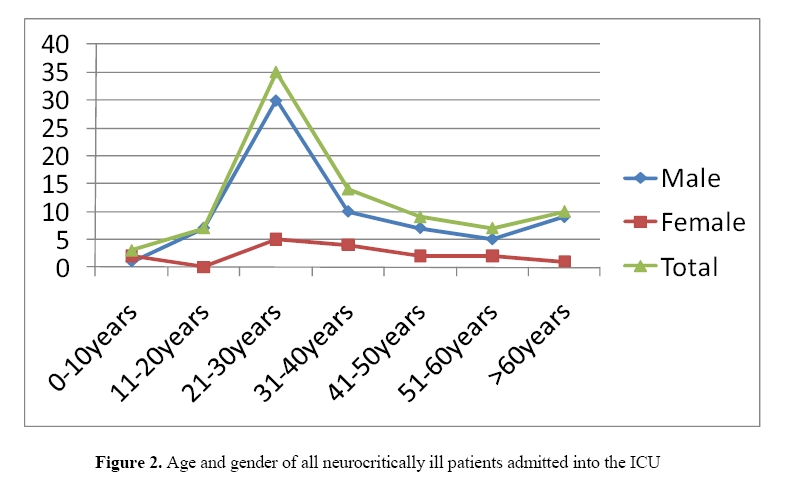
neurocritical care facility, human resources, patient admission and outcome. Introduction The critically ill patient pose a lot of management challenges to the managing physician especially in low income societies. This is truer in poverty stricken third world countries where limited facilities in terms of beds, drugs and equipment are a common scenario. The quality of care is directly related to manpower and equipment. Intensive Care has emerged as a distinct specialty in the world over the last 3-4 decades1. The original concept of the nursing legend, Florence Nightingale of rounding up all seriously ill patients in hospital matured to become recovery units for postoperative care in the early 1950’s. The importance of mechanical ventilation was mostly realized in the polio epidemic in Copenhagen in 1952 where the mortality rates reduced from 90% to 40% following its introduction2. This gradually led to the recognition of the importance of close monitoring and vital function support in the treatment of life threatening diseases. It is recommended that 15% of total bed strength of hospitals should be equipped for critical care; most countries have provision for only 1-2% of their total bed strength for critical care3. In Nigeria as a whole, ICU bed availability is substantially low, perhaps below 1% and there is no governing body or a planning institute that scrutinizes the standards of such units (personal communication). Alarmingly, in Nigeria’s most densely populated state there are just five functional ICUs- two government-owned ICU and four privately operated ICUs. All these are grossly inadequate for an estimated 14million population of the state. To make matters worse, some states in the country do not even have an ICU. Intensive Care Unit (ICU) is not only a medically important part of the Hospital, but is also a politically sensitive issue because of the costs involved for its establishment, maintenance and running despite the obvious public demand for this service. Data on intensive care services in the country and the subregion is rare. Our objective is to audit our neurocritical care facility, human resources, patient admission and outcome so as to find out areas that need adjustment to better improve the quality of our patient care practice. Patients and Methods We carried out a retrospective study of the patients admitted into one of our ICUs at the Lagos State University Teaching Hospital (LASUTH), Ikeja, Lagos, Nigeria, over a 12month period (January 2008- December 2008). All surgical and non-surgical patients were included in the study. Data were extracted from the Medical Records and reviewed. Data retrieved from each patient’s record included demographic data, date of admission, indication for admission, treatment (operative/non-operative), ventilatory support if any, and outcome (Alive or dead). Our institution has two ICU facilities, one of which is restricted to patients due to its high cost. The study was restricted to the relatively affordable ICU facility. The daily running cost is two thousand naira; this is due to major subsidization be the government. This ICU is a four bedded facility. It is a multidisciplinary station managing medical, surgical including obstetrics and gynecology, and pediatric patients. The resources and facilities available at our four bed ICU includes a nurse: bed ratio of 1:1, a centrifuge, one blood gas analyzer, a defibrillator, multiparameter monitor and ventilator for each bed, with facility and expertise for central lines. Data was analysed by simple frequency, percentages, Chi-square and Fischer’s Exact test as appropriate. P<0.05 was considered significant. Data collected was analyzed using SPSS version 13 computer software. Results During the study period a total of 129 admissions were made. The indication for admission was due primarily to a neurosurgical indication in 85 patients (65.9%). The main indication for admission was following significant head trauma (Figure 1). Majority of the patients were males (69 patients) with a male female ratio of 4.3:1. The age distribution is depicted in Figure 2 (range: 1.5 – 84 years; mean: 36.1 years; median:30 years). Table 1. Outcome of Ventilated compared with Unventilated Patients
The overall mortality was 22/85 (25.9%) while mortality of ventilated patients was 11/17 (64.5%). Mortality rate was not significantly affected by gender (p=0.170) but those that were ventilated were more likely to die (p=0.000). The ICU was fully occupied by patients most of the time. Only 11patients were admitted to the ICU following surgery, 3 of these were admitted following elective brain surgery while the remaining eight were already in the ICU prior to surgery. Most patients that needed ICU admission after surgery were not admitted due to lack of space. Facilities for mobile X-ray, intracranial pressure, trancranial Doppler and electroencephalography were absent during the study period. Likewise 24hour in house intensivist was epileptic. The proposed high dependency unit was yet to take off during the study period, putting more strain on the ICU. Discussion Current evidence support ‘closed’ ICU systems when compared with ‘open’ ICUs; this is in the context of better outcomes for patients4,5. Despite this, the ‘open’ type of ICU still predominates in most low and middle income societies due to paucity of intensivists, ICU teams and a relatively high cost to establish and maintain them compared with the ‘closed’ ICU. An open ICU has unlimited access to multiple doctors who are free to admit and manage their patients. A closed ICU has admission, discharge and referral policies under the control of intensivists. Improved cost benefits are likely with a closed ICU, and patient outcome may be better, especially if the intensivists have full clinical responsibilities6. Most ICUs are located in teaching hospitals, with the “luxury” of several specialized ICUs in each hospital. At present we do not have a specialized ICU. But our unit often has inputs from multiple specialties. Historically, the two most important milestones in critical care that made a significant impact on morbidity and mortality i.e. 24 hours resident medical officer and a nurse:bed ratio of 1:1. This is to be coupled with minimum monitoring standards which includes multiparameter monitor with ECG monitor at the bedside of each patient3. In this study we noted that the the medical officer coverage was not in-house. This is increases the response time to patient’s problems. In some centres, over 40% of intensive care unit admissions are for post – operative patients7,8. An unplanned admission to an intensive care unit within 24 hours of surgery is an event that most patients and physicians would consider to be an important adverse outcome. Such an unfavourable outcome results from an amalgamation of inherent risk factors surrounding a combination of coincidences and even misjudgements in the perioperative period. The multifactorial interaction of patient, anaesthesia and surgical variables determines the overall patient risk. Early recognition and intervention remains the key to avoidance of unfavourable outcome. In our centre this is the contrary as most patients had admitted were not pot-operative patients. Due to its small size, our ICU was usually full. This may explain the relatively low percentage of post-operative patient’s admission. Persistent occupancy of more than 70% suggests a unit is too small9. Occupancy of 80% or more is likely to result in non-clinical transfers, with associated risks. Too few beds may increase mortality or non-clinical transfers, while extra capacity may not decrease occupancy if patients of a lower dependency level are admitted, or there are problems discharging patients to other locations10. The problems identified in our ICU included non-availability neurocritical care equipments for intracranial pressure (ICP) measurements, etc. The absence of appropriate protocols for managing common ICU cases and common procedures was also the norm. There are times where communication breakdown results due to the diversity of the various specialties making use of the ICU. The high intake of Neurosurgical patients makes case for more facilities to serve these groups of patients. Current neuromonitoring techniques involve a range of tools that have evolved from the study of cerebral physiology and advances in the understanding of the pathophysiology of acute brain injury. These techniques have focused on the measurement of cerebral physiologic and metabolic parameters with the goal of improving the detection and management of primary and secondary brain injury in patients who have suffered head injury, stroke, subarachnoid haemorrhage, or have had neurosurgical procedures11-13. The development of new neuromonitoring techniques has been particularly important because standard monitoring techniques, such as ICP and cerebral perfusion pressure measurements, are sometimes insufficient in detecting subtle manifestations of brain injury or are poor surrogates for physiologic parameters of interest. For example, cerebral perfusion pressure may be an unreliable method to measure cerebral blood flow14,15. The more recently developed neuromonitoring techniques like cerebral blood flow monitoring techniques, brain tissue oxygen tension (P bt O 2 ) and jugular bulb venous oxygen saturation (SjVO 2 ) monitoring, and cerebral microdialysis, provide more detailed information regarding cerebral metabolic function. These measurements provide information that is of prognostic utility as well as help direct management of the neurocritically ill patient in order to improve clinical outcome. Even as many of these tools are now becoming integrated into regular neurocritical care, research is ongoing to determine the validity, reliability, and utility of these techniques in the clinical management of patients and in predicting and potentially improving clinical outcome12. Conclusion Neurological patients account for most of our ICU admission. Hospitals with ICUs should ensure that they have a proper high dependency unit. This will significantly reduce the strain on their ICUs. We also recommend that appropriate equipments and staff training in the area of neurocritical care be incorporated into existing ‘open’ ICUs in our environment. The use of protocol for ventilated patients and managing common ICU cases and common procedures should enhance treatment outcomes. A regulator for the maintenance of standards in the country will also help in achieving appropriate standards in the country. References
Copyright © 2010 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js10021f2.jpg] [js10021f1.jpg] |
| |||||||||

{kind=link}
{kind=link}