 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
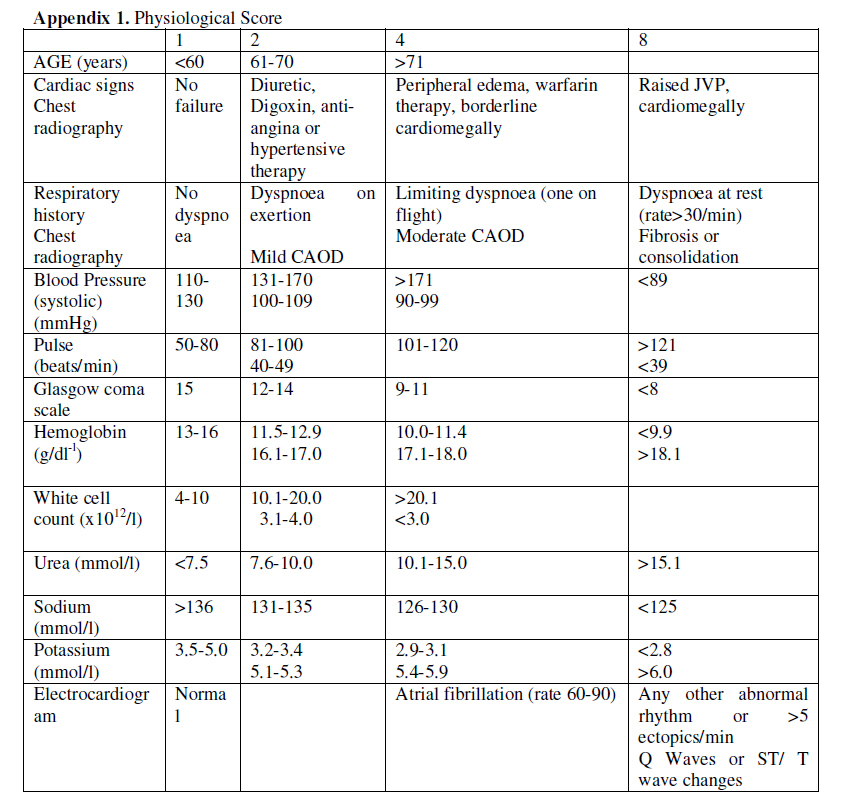
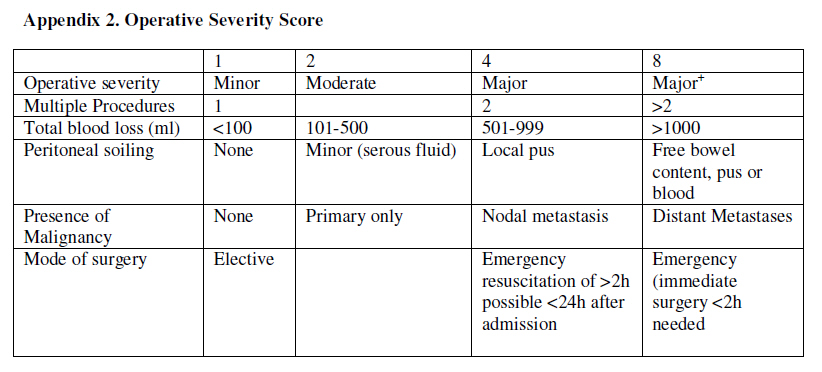
East and Central African Journal of Surgery, Vol. 15, No. 2, July-December, 2010, pp. 90-96 Original Article The Postoperative Complications Prediction in Mulago Hospital using POSSUM Scoring System DL Kitara, I Kakande, BD Mugisa, JH Obol Kampala, Uganda Correspondence Address:D L Kitara, Kampala, Uganda, klagoro@yahoo.co.uk Code Number: js10041 Abstract Introduction: Prediction of complications is an essential part of risk management in surgery. Knowing which patient to operate and those at high risk of developing complications contributes significantly to the quality of surgical care and cost reduction. The postoperative complications of patients who underwent Laparotomy in Mulago Hospital were studied using POSSUM scoring system. The main objective of this study was to determine the postoperative complications of Laparotomy in Mulago Hospital, between September 2003 and February 2004.Methods: Consecutive patients, who underwent Laparotomy in Mulago, were studied using POSSUM system for development of complications. For each patient operated, they were followed up in wards until discharge. When the postoperative complications were reported, they were reexamined by the surgeons, treated and followed up for 30 days postoperatively. Phone contacts were used for the follow up. Surgical reviews were conducted once a week in Mulago Hospital and the data obtained recorded in the data sheet for the patients. Results: Seventy-six patients were studied. The observed post operative complications were as follows: Respiratory tract infection (28.2%), wound haemmorrhage (18.2%), anaemia (15.5%), hypotension (14.1%), UTI (2.2%), Anastomotic leak (1.4%), Wound sepsis (9.9%), wound dehiscence (4.2%), Thromboembolism (1.4%). The postoperative nursing care significantly determined the outcomes. Conclusion: Postoperative complications can be predicted in the modern management of surgery especially while using a scoring system. Introduction Risk management is an important health care issue. Prediction of complications is an essential part of risk management in surgery. Knowing which patient is at risk of developing complications contributes to the quality of surgical care and cost reduction in surgery. [1] It is therefore essential to identify and make appropriate decision on those patients who are at high risk of developing serious complications [1],[2] . Postoperative complications are sometimes determined by the surgical procedures conducted. [1],[2] Postoperative complications delay patients discharge, mobilization and markedly reduce the patients′ income, increase hospital costs, increase absenteeism at work and reduced patients′ productivity. They create an unnecessary discomfort to the surgical team, stress, anger, and sometimes depression especially when the complications can not be easily corrected or takes long to be corrected e.g. enterocutaneous fistula. Various studies have been conducted in Uganda to assess the postoperative complications. None has been by use of a scoring system such as (POSSUM). This study showed that the development of the postoperative complications is not affected by the socio-economic status of the patient but rather the preoperative, operative and postoperative management of the patient. Patients and Methods This was a prospective descriptive study conducted over a period of 6-months in Mulago Hospital, Kampala, Uganda. The study population consisted of 76 patients aged 13 years and above admitted for elective and emergency surgery. Day-care surgery and those who died immediately before surgery were excluded.The patients were assessed preoperatively, operatively and postoperatively for any complications. 76 patients underwent Emergency or Elective Laparotomy in the Hospital Theatres. The patients were scored with the physiological component of POSSUM just before the induction of general anesthesia. All the individual scores were computed and summed up to produce the POSSUM physiological score for each patient. The operative procedures were conducted in the same manner and using midline incision. Intra-operative blood loss, type of surgery, the presence or absence of peritoneal soiling and intra-abdominal tumors were recorded and summed up to constitute the operative score for each patient. The closure of the abdomen was done using the same suture material and equal size. The Follow-up of the patients was done up to 30th postoperative day. Patients were reviewed weekly in Surgical Outpatient Department. Telephone contacts were used, where possible. When a patient died, post-mortem examinations were conducted by a pathologist and findings recorded and summarized for the purpose of this study. Morbidity was investigated and appropriate treatment administered to the patient as required. Statistical data analysis was conducted using the SPSS version 10.0 software. A student t-test was used to compare significant differences and chi-square/Fisher′s exact test was used in testing association of categorical variables. The quality control was ensured by making the principal investigator carryout all the pre-operative and postoperative assessment, clinical examinations and measurements of parameters using standard International units (SI) to avoid inter-observer error. Laboratory investigations were done by the same method and in standard unit. Results The patients′ ages ranged from 14 to 81 with a mean of 40.4 years. M:F ratio of 2:1. Peasant farmers accounted for (52.6%), Business (self employed) (27.6%), Civil servant (13.2%) and Students (6.6%). Intestinal obstruction comprised 19.4%, abdominal trauma (18.4%), peritonitis (18.4%) and abdominal malignancy (18.4%), appendicitis (13.2%) and surgical jaundice (11.8%). The majority (78.9%) of the patients investigated had no comorbid conditions. Hypertension accounted for 11.8% and the others accounted for less than 10%, sickle cell disease, peptic ulcer disease and Diabetes Mellitus each. A total of 55 (72.4%) of the operations were performed by the Senior Residents compared to 13 (17.1%) and 8 (10.5%) by Consultants and Senior Registrars respectively. The Senior Residents performed 86.3% of the emergency operations as compared with 9.8% by Senior Registrars and 3.9% by Consultants. For elective surgery, (44%) by Senior Residents, (12%) by Senior Registrars and 44% by consultants. The mean duration of postoperative Hospital stay was 8.46 days. Thirty two patients were discharged in the 1 st post-operative week while thirty (30) were discharged in the 2 nd week. The remaining fourteen (14) spent more than 2 weeks in the Hospital. The conditions associated with mortality included intestinal obstruction (45.5%), peritonitis (27.3%), intra-abdominal tumor (18.2%), and surgical jaundice (9.1%). The mean postoperative day of death was 12.4. All the patients died due to septic shock. Thirty-five patients had a mortality risk greater than 50%; twenty patients had risk (21-49%), nine patients had (11-20%) and fifteen patients had (1-10%) of death. This result shows a positive correlation and a significant relationship between death and physiological score (p=0.003).There was a positive correlation between death and the operative severity score p-value 0.012). [Table - 1] shows the ranks of the operating surgeons. The surgical residents (Senior House Officers) performed the majority of the procedures (72.4%), Senior Registrars (10.5%) and Consultants (17.1%). Most (67.1%) of the operations were done as emergencies. Electives operation were 25 (32.9%).The Senior House Officers performed the majority of the emergency operations of 44 (86.3%), Registrar 5 (9.8%) and Consultant 2 (3.9%). Elective Procedures: Senior House Officer (SHO) 11 (44%), Consultant 11 (44%), Registrar 3 (12%) The commonest cause of morbidity was Respiratory tract infection in 20 (28.2%) and commonly occurred on the 2 nd postoperative day, followed by wound haemorrhage in 13 (18.2%), anaemia 11 (15.5%), hypotension in 10 (14.1%), wound sepsis in 7 (9.9%), urinary tract infection in 2 (2.2%), anastomotic leak in 1 (1.4%), wound dehiscence developed in 3 (4.2%) and congestive cardiac failure. Discussion Assessing the postoperative complications following a Laparotomy is very important especially when using a scoring system (POSSUM). This was an effective method of assessing the risk of morbidity following Laparotomy in Mulago Hospital. The age, sex, tribe and religion of the patients did not significantly affect the development of complications following Laparotomy. A study in the USA indicated that increasing age was strongly associated with risk of complications but surprisingly, the risk declined for patients older than 79 years of age. The most likely explanation for the phenomenon was that there was a strong selection bias before hospitalization with older high-risk patients not being considered suitable for admission for surgery. [18] This observation was not made in this study probably because over 80% of the patients were below 40 years and so their age did not significantly affect the outcome. Nature of Surgery The nature of surgery had a significant effect on the operative scores for the patients. On average, the emergency operations had higher operative scores (23.39). There was a positive correlation (t=4.375) and a significant relationship (p=0.000) between emergency operation and the operative scores. Similarly emergency surgery had a higher average physiological score (25.63). The risk of morbidity was significantly increased by the nature of the operation. A study involving 232,440 surgical patients at 168 hospitals in the state of Pennsylvania, USA indicated that a higher patient to nursing staff ratios is associated with higher risk-adjusted postoperative mortality rate. [20] This means that nursing care alone can be shown to be a robust independent predictor of postoperative deaths. [19],[20] These results indicate that factors such as hospital resources, the availability and training of medical staffs have a significant impact on the postoperative outcome (mortality and morbidity). [5],[19],[20] . The Surgeons There were three categories of surgeons who carried out the surgical procedures: Consultants, Registrars, and Senior Residents (SHO). The consultants conducted 13 operations. All the patients had very good physiological status. There was a negative correlation and an insignificant relationship between the 2 variables (t=-1.643 and p=0.105). Similarly their mean operative score was low (17.62). For the Registrars, they conducted 8 operations. There was a negative correlation (t=-0.344) between the Registrar and the operative score. The majority of the operations were conducted by the senior Residents (55/76). In general, the Senior Residents conducted operations on patients with higher physiological scores (poorer physical condition). There was a positive correlation (t=2.765) and a significant (p=0.007) relationships between the physiological score and the Senior Residents. Higher- risk surgery performed independently by physician in training was shown to be related to poor postoperative outcome. [5] The UK government report, have drawn attention to the dangers of leaving high-risk procedures to trainee surgeons without supervision. [5] In general, there was a negative correlation between the surgeons and the risks of morbidity. The Physiological Score (PS) The average physiological score observed in the study population was 25.22. This value is comparable with other studies done in the USA and UK [5] The most frequently observed group were those between the ranges of 20-29. This score however, was found to have a positive correlation and a significant p-value with mortality (t=2.228 and p=0.029). This is consistent with the findings observed in the USA and UK [5] . The physiological score had a negative correlation (t= -0.019) and an insignificant value (p=0.436) with morbidity. The physiological score alone could not be used to predict the risk of development of omplications because there was other confounding factors observed. [3] The Operative Score (OS) The average score was 21.2. Again this average is comparable with other studies done in the UK and USA and other developing country such as Malaysia. [5],[10] Tribe, occupation, and diagnosis or co morbid conditions did not significantly affect the operative score. There was a positive correlation and a significant p-value for the relationship with mortality and morbidity and operative scores (t=3.280 and a p=0.00) and (t=0.197and p=0.044). This observation is consistent with the findings in USA, UK [5] and Malaysia. [10] Postoperative Hospital Stays (Days) The mean postoperative hospital stay was 8.46. This value was comparable with the findings in UK, USA [5] and Malaysia [10] . Olaro (1999) observed the postoperative hospital stay at Mulago Hospital was at10 days [11] . The postoperative hospital stay had a negative correlation (t= -2.894) to mortality (p=0.005). Furthermore, the postoperative hospital stay had a positive correlation (t=3.571) and (p=0.001) with morbidity. The Observed Mortality Eleven out of the seventy-six patients studied died. This gave a mortality rate of 14.5%.This mortality rate was comparable with other previous studies done in Mulago Hospital. Birabwa-male 1989(21.7%) and Fiedler et al 1986 in USA (17%), Mugisa (1988) and Kazibwe (1987) (10-20%) [4],[13] . The Laparotomy related to intestinal obstruction was the commonest cause of death (45.4%). similar findings observed by Olaro (1999) with large gut surgery being commonest cause of mortality 28%. [11] Peritonitis came second (27.3%). Surgical jaundice came third (9.1%) and carcinoma of the pancreas fourth (9.1%). All the emergency patients who died had very high physiological scores (>25). All the elective patients who died had high operative scores (>22). Diabetes Mellitus increased the risk of mortality. The observed Morbidity Fifty two point three percent (34/65) of the patients who lived postoperatively developed complications. The factors responsible were: operative scores (t= 0.193 and p= 0.044), surgical jaundice (t= 0.202 and p= 0.040), and Peptic Ulcer Disease (t= 0.308 and p= 0.003). The operative score directly affected both the risks of mortality and morbidity. [5] Surgical jaundice contributed to the development of complications (t= 2.654and p= 0.010). Those patients with the peptic ulcer diseases had higher physiological and operative scores. The Postoperative Complications Respiratory tract infection was the commonest complication (28.2%) observed. This occurred mainly in 2 nd and 5 th postoperative days. Those in second day were either due to aspiration pneumonia or hypostatic pneumonia due to poor ventilation. All those who developed respiratory tract infection experienced postoperative pain for most times. The pain therefore explains the cause of the poor ventilation and subsequent postoperative retention of secretions and development of respiratory tract infection. Andrew [14] in his study found that respiratory complications were common among those who had higher abdominal incision and this was due to atalectasis. He observed that, the main pathological changes observed was alveolar collapse of the lungs and this was observed in association with restriction of ventilation especially in those patients who had a very poor pain control [14] . indeed the evaluation of the treatment chart in Surgical department at Mulago Hospital confirmed that either the drug given was inadequate or irregular and that the pain reliever were not titrated against the pain experienced by the patient. In some instances, the quality of analgesics was not strong enough to relieve pain following the Laparotomy e.g. use of paracetamol (1000mg) three times a day in the 2 nd post operative day. Wound hemorrhage was the secund commonest (18.2%) cause of morbidity and this mainly occurred on the 1 st and 3 rd postoperative day. Mugisa [4] observed a rate of (10%) and mainly among patients operated by the Senior Residents (SHO). He attributed this finding to emergency patients being operated in a state of shock. They were usually inadequately resuscitated and therefore the failure to localize the abdominal wall bleeders [4] . Anaemia was 3 rd commonest postoperative complications accounting for (15.5%). The most reported cases were in the 4 th postoperative day. This mainly occurred in patients who had blunt abdominal trauma with ruptured intra-abdominal viscera. They were in most cases, found to have lost more than 1 liter of blood in the peritoneal cavity in the operative period. Mugisa (1988) observed a rate of anaemia in 11.3% of all the Laparotomy patients in Mulago Hospital. Wound dehiscence accounted for (4.2%) and Wound sepsis accounted for (9.9%). Wound sepsis was commonly seen in patients with pussy peritonitis between 4 th - 7 th postoperative days. Mugisa [4] in 1988 observed a higher rate of 15% for wound dehiscence. He attributed this to poor surgical technique among the surgeons. Rousellot [15] found that in USA, the incidence of wound infection was 15% and was the commonest complications experienced. This occurred between 4 th -7 th postoperative day clinically shown with a spiking fever. Thromboembolism was observed in 1.4% of the cases and this was in a sickler. This sicker experienced a painful crises in the postoperative period. Aagard [16] observed 15% prevalence of Thromboembolism in those above 50-years. This prevalence was higher compared to what was observed in this study population probably because the majority of the patients were younger and there were few cancer surgeries (a Thromboembolism promotion factor). Conclusion
Recommendations
References
Copyright 2010 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js10041t1.jpg] [js10041a2.jpg] [js10041a1.jpg] |
| |||||||||

![[Table - 1]](/showimage?js/photo/js10041t1.jpg){kind=link}
{kind=link}
{kind=link}