 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 16, No. 1, March/April, 2011, pp. 12-18 Adult Chronic Rhinosinusitis: Spectrum of Clinical features and management in a Tertiary Health Institution and Literature Review A.J. Fasunla, O.G.B. Nwaorgu Department of Otorhinolaryngology, University College Hospital, Ibadan Nigeria Correspondence to: Dr Ayotunde James Fasunla, Department of Otorhinolaryngology, University College Hospital, Ibadan. Nigeria, E-mail: ayofasunla@gmail.com Code Number: js11002 Background: Rhinosinusitis is defined as inflammation of the
nasal and paranasal sinus mucosa. Chronic rhinosinusitis occurs when this
inflammation and the symptoms persist for more than 3 months. The objective of
this study was to evaluate the clinical features and management of adult
chronic rhinosinusitis in a tertiary health institution and to review the
literature for its current modalities of management. Introduction Rhinosinusitis is a common clinical condition which affects more than 16% of the adult population annually1,2. It is defined as inflammation of the nasal and paranasal sinus mucosa. Chronic rhinosinusitis occurs when this inflammation and the symptoms persist for more than 3 months. Osteitis of the underlying bone may occur3. Chronic rhinosinusitis is a multi factorial disease and obstruction at the osteomeatal complex usually accounts for most cases of chronic rhinosinusitis. This obstruction could be caused by nasal allergy, polyps, bacterial or fungal infection, anatomical abnormality like septal spurs/deviation, concha bullosa, enlarged ethmoidal bulla, tumors, immunodeficiency and mucociliary impairment4. There are two histopathologic categories; the polypoidal mucosal change with eosinophilia variant is usually associated with a more severe damage to the nasal mucosa than the submucosal serous gland hyperplasia category5-7. The burden of this disease on those it affects made it a challenge to the society. It impacts negatively on their quality of life thereby causing socioeconomic and academic loss. Although family physicians and pulmonologists are able to evaluate and care for some of these patients, they are usually faced with challenges of the disease recurrence, chronicity and complications. Good and adequate knowledge of the pathophysiology of this disease will bring about a better, effective treatment and good, satisfactory treatment outcome. Otorhinolaryngologists therefore have the responsibility of providing an accurate, efficient and accessible method of making diagnosis of chronic rhinosinusitis and also, providing an expanded knowledge about the disease process as well as developing better treatment modalities. The aim of this study therefore, was to evaluate the clinical features and management modalities of chronic rhinosinusitis in our center and also, to present a review of its current management modalities. Patients and Methods This is a 5-year retrospective study of all adult patients managed for clinically and radiologically diagnosed chronic rhinosinusitis at the department of Otorhinolaryngology, University College Hospital, Ibadan, Oyo State, Nigeria from 2003–2008. The diagnosis was made based on the consensus reached and created in 1997 by the Rhinosinusitis Task Force of the American Academy of Otolaryngology, Head and Neck Surgery (AAO-HNS) which was revised and amended in 2003 by the Sinus and Allergy Health Partnership (SAHP)8-9. Patients’ data collected from their medical records included demographic data (age, sex), presenting symptoms and their duration at presentation with examination findings. Reports of the skin sensitivity test and plain radiographs of the paranasal sinuses comprising the occipito-frontal (Caldwell), occipito-mental (Water's) and lateral views were extracted as documented by the radiologist. The associated complications and treatment modalities were also collated. Those with incomplete data were excluded from the study. The data collected were analyzed using simple descriptive method and the results presented in tabular forms. Results Chronic rhinosinusitis constituted 78.2% of the total adult rhinologic cases seen during the study period. There were 228 patients, 97(42.54%) males and 131(57.46%) females with a male: female ratio of 1:1.35. The age ranged from 18 - 67 years (mean =35.2). The five major presenting symptoms were nasal discharge 228(100.00%), nasal obstruction/congestion in 224 (98.25%), frequent hawking of throat 189 (82.89%), itching of the eye, ear, nose or throat in 138 (60.53%) and excessive sneezing in 136(59.65%) (Table 1). Table 1. Clinical presentations of patients with chronic rhinosinusitis
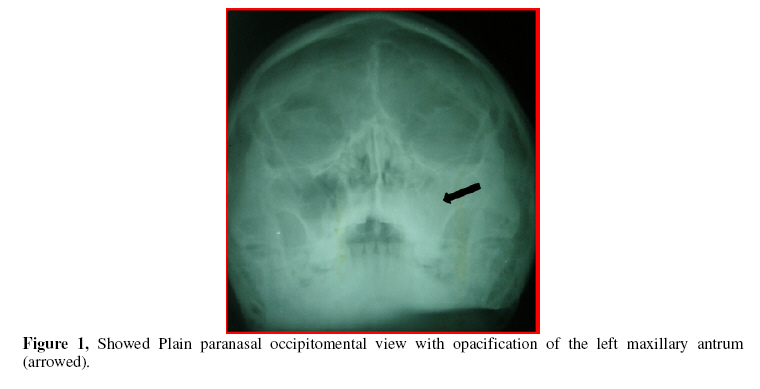
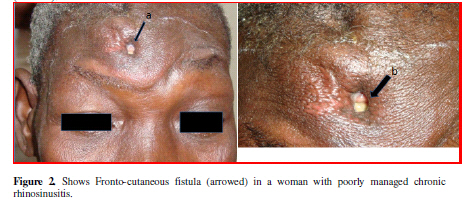
Note: All the patients had more than one symptom The clinical findings of the patients are presented in Table 2. Allergy accounted for the cause in 93 (40.79%) patients and nasal polyposis was seen in 13 (5.70%) patients. The diagnosis of chronic rhinosinusitis was further confirmed with plain paranasal sinus x-ray. The plain paranasal sinus radiographs of 34 (14.91%) patients appeared normal. The radiographic findings in the remaining 194 (85.09%) patients showed different abnormalities. There was involvement of more than one paranasal sinus in some of these patients and about 93% of the X- ray abnormalities showed involvement of maxillary sinuses (Figure 1). Mucosal thickening was found in 147 (75.77%) patients, soft tissue shadow in the nasal cavities suggesting engorged inferior turbinates were found in 139 (71.65%), opacification of the maxillary antrum in 39 (20.10%) patients, diffuse opacification of the nasal cavity (ies) in 28(14.43%), septal spur/ deviation in 19 (9.79%) patients and fluid level in 2 (1.03%) patients. More than one radiologic feature was seen in some patients. The complications included Frontoethmoidal mucocele in 8 (3.51%) patients, Frontocutaneous fistula in 2 (0.88%) patients, Potts’s Puffy tumor in 2 (0.88%) patients, blindness in 1 (0.44%) patient and intracranial abscess in 1 (0.44%) patient. Eighty one (35.53%) patients were successfully treated with medical treatments using nasal decongestant, ascorbic acid, steam inhalations and antibiotics. Medical and Surgical treatments were used in the remaining 147 patients. One hundred and seventeen (51.32%) patients were treated with intranasal inferior meatal antrostomy with or without inferior turbinectomy, 12 (5.26%) patients were treated with Caldwell-Luc operation and 18 (7.89%) patients were treated with external frontoethmoidectomy. All the patients had intranasal warm normal saline irrigations, ascorbic acid, antibiotics and decongestants post-operatively. Those with nasal polyposis had intranasal polypectomy and steroid therapy. Twenty one (17.95%) patients who had intranasal inferior meatal antrostomy had recurrence of symptoms within 3 – 8 months postoperative period. The patients with blindness due to sphenoidal mucocele and intracranial abscess had surgery via trans-nasal, external and skull base surgical approaches. Table 2. Clinical findings in patients with chronic rhinosinusitis
Note: All the patients had more than one sign. Discussion Chronic rhinosinusitis is a common clinical presentation to the otorhinolaryngologic clinic as seen in this study where it constituted about 78% of rhinologic diseases in the adult population. The transition of rhinosinusitis from acute phase to chronicity depends largely on the predisposing factors which may be host or environmental (infective and non-infective) in origin9, 10. Chronic rhinosinusitis occurs when the sinonasal mucosa inflammation persists for more than 3 months. This may result in defective ventilation of the paranasal sinuses when their ostia are obstructed. Irrespective of the etiologic factor, the clinical manifestations of this disease entity are similar11. The spectra of clinical features of chronic rhinosinusitis seen in this study (Table 1) do not differ much from what had been reported in similar studies in both developing and developed countries8-13. Prior to 1997, there was no consensus reached as guideline for the diagnosis of rhinosinusitis. Some common sinonasal symptoms and signs were organized into major and minor factors in order to create a uniform diagnostic paradigm for rhinosinusitis. This was the product of consensus reached and created in 1997 by the Rhinosinusitis Task Force of the American Academy of Otolaryngology, Head and Neck Surgery (AAO-HNS). This laid emphasis on patient’s history and limited physical examination findings which allow most patients to be diagnosed and effectively treated without an immediate need for further investigations. The diagnostic criteria for chronic rhinosinusitis require 2 or more major factors or 1 major factor and 2 minor factors8. Major factors for diagnosis include facial pain or pressure, facial congestion or fullness, nasal obstruction or blockage, nasal discharge or purulence or discolored postnasal discharge and hyposmia or anosmia. Minor factors were defined as headache, fever, halitosis, fatigue, dental pain, cough, and ear pain or pressure, or fullness9,14. However, facial pain or pressure alone does not constitute a strong history for diagnosing chronic rhinosinusitis in the absence of another major symptom or sign9,14. The physical findings in this study (Table 2) are similar to the findings from other studies8,9. Although these physical findings are important in chronic rhinosinusitis, they are not part of the diagnostic criteria initially created by Rhinosinusitis Task Force of the American Academy of Otolaryngology, Head and Neck Surgery (AAO-HNS)8. The use of patients’ symptoms alone in the diagnosis of chronic rhinosinusitis has a pitfall as it does not address the cause of the problem. Obstruction at the osteomeatal complex usually accounts for most cases of chronic rhinosinusitis4. Objective assessment measures aid in identifying the cause and the extent of the obstruction. A careful subjective and objective assessment measures are therefore the key to improving diagnostic accuracy. The anterior rhinoscopy, nasal endoscopy and Computerized Tomographic scan are objective measures that can increase the accuracy of chronic rhinosinusitis diagnosis15. The Sinus and Allergy Health Partnership (SAHP) reviewed and amended the subjective diagnostic criteria created by Rhinosinusitis Task Force of the American Academy of Otolaryngology, Head and Neck Surgery to include physical and nasal examination findings in addition to suggestive history13. These physical findings were divided into two groups namely; those accessible to all health care practitioners (examination of the face and anterior rhinoscopy) and to Otorhinolaryngologists (nasal endoscopy)13,15. The expected facial findings include swelling and erythema of the maxillary, ocular, orbital and frontal areas. The anterior rhinoscopy findings include hyperemia, edema, crusts, purulence and polyps. The findings of Anterior rhinoscopy is limited as it may not reveal the pathology like grade 1 polyps, secretions and anatomical abnormalities at the osteomeatal complex due to poor exposure and visualization. Endoscopic examination by an otolaryngologist is useful in the diagnosis of chronic rhinosinusitis. The nasal endoscopy findings include bluish discoloration of turbinate, generalized or localized erythema, purulent discharge from Osteomeatal complex/sinus ostia, polypoidal swelling or granulation tissue, septal deviation, concha bullosa and paradoxical turbinates13,15. The grading of nasal polyps was presented in the work of Lund and Mackay16. There is a high correlation between endoscopic findings and Computerized Tomographic examination15,17. The endoscopic observation of pus, polyps, or other significant mucosal derangements helps solidify the diagnosis. For areas that are not accessible to nasal endoscopy, Computerized Tomography can be useful in identifying disease. In our practice, examination of adult with chronic rhinosinusitis does not routinely involve nasal endoscopy. This is because the endoscopes are not readily available for use on the patients in our center. We therefore depend on the facial and anterior rhinoscopic findings in addition to the presenting symptoms in making diagnosis. Non usage of diagnostic nasal endoscope in our clinical practice would have resulted in some important clinical findings being missed thereby, resulting in incomplete clinical documentation of the disease. Radiological imaging is complementary to the clinical evaluation of patients with rhinosinusitis. Radiographic examination has evolved significantly over time. Computerized Tomographic (CT) scan has replaced plain-film radiographs as the standard for paranasal sinus imaging in health institutions in developed countries18,19. However, in most centers in the developing countries, patients are still being evaluated with plain radiographs of the paranasal sinuses (Figure 1) because of availability and cost. In our centre, it is often those who had complications or with doubtful diagnosis on plain radiographs that are re-evaluated with CT scan. This is because most of our patients are from the low socioeconomic class and can hardly afford the investigation. The plain radiographs of the paranasal sinuses have the limitation of many structures being superimposed on one another and not being able to define the osteomeatal complex18,20. CT scan of paranasal sinuses has the merit of better disease delineation and will show any anatomical intranasal abnormality especially at the osteomeatal complex and paranasal sinuses18. Since the advent of antibiotics, complication of infective rhinosinusitis is uncommon21-22. However, about 6.14% of our patients with chronic rhinosinusitis still presented with different complications. Fronto-ethmoidal mucocele is the commonest complication seen in this study. These patients commonly presented with frontal headache, scanty anterior mucoid nasal discharge and frontal swelling. Fronto-cutaneous fistula was seen in two patients (Figure 2). Self medication and delayed presentation for appropriate management were the factors identified to have contributed to the development of fronto-cutaneous fistula in these patients. The principles of management of chronic rhinosinusitis include treatment of the underlying cause, reduction of nasal mucosa inflammation and swelling, and restoration of ventilation of the paranasal sinuses23. In this study, medical treatment alone was successfully used to treat 36% of cases. This treatment includes the use of steam inhalation, nasal decongestant, ascorbic acids and antibiotics. Those patients with allergy and allergic nasal polyposis also had steroid therapy. The use of steroid in the treatment of nasal polyps has been reported10-11,23. All patients in this study had initial medical treatment and surgery was indicated only if the symptoms persisted or worsened and when there is an obvious growth or polyps in the nasal cavity. Surgical management of chronic rhinosinusitis is indicated when there is failure of medical treatment and when there is an obvious growth or anatomical abnormalities within the nasal cavity preventing drainage and aeration of the sinuses24. In this study, intranasal inferior meatal antrostomy with or without inferior turbinectomy was performed in 51% of the cases. This surgical procedure is usually performed with the intention of providing dependent drainage for the maxillary sinus which is believed to be the site commonly affected by the disease. Perhaps, this procedure is justified as about 93% of the paranasal sinus radiograph in this study showed involvement of the maxillary sinus. Recurrence of symptoms was seen in 18% cases within 3 – 8 months after the surgery in this study. When this fails to achieve the desire outcome and improvement then, removal of the entire maxillary mucosa is performed through Caldwell-Luc procedure25. Twelve (5.26%) patients in this study were treated with Caldwell-Luc operation. The invention and use of nasal endoscope has brought about better understanding of the disease pathogenesis and osteomeatal complex is now known to be more frequently involved in the disease. The inflammation in this area usually spread to obstruct the drainage of paranasal sinuses and produce repeated infection and hence, persistent mucosa inflammation4, 9-10,26. Surgical management that focuses on the removal of the obstructive pathology at the osteomeatal complex region has been efficacious and has provided a better improved surgical outcome of this disease24, 26-28. The goal of this procedure is to re-establish the patency of the paranasal sinuses natural ostia for aeration and drainage. This is thought to bring about a reversal of the damaged sinonasal mucosa to normal state27,28. Septoplasty should be performed to correct septal spur/deviation contributing to nasal obstruction. This was never part of the surgical management of these patients in this study. This may be the reason while some of these patients had recurrence of their nasal symptoms29. Conclusion In making diagnosis of chronic rhinosinusitis in adults, both subjective and objective measures should be employed for the purpose of an improved accuracy. Emphasis should be laid on the therapy that will remove the cause of the disease and restore the patency of natural ostia for improved sinus aeration and physiologic drainage. References
Copyright 2011 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js11002t2.jpg] [js11002t1.jpg] [js11002f2.jpg] [js11002f1.jpg] |
| |||||||||

{kind=link}
{kind=link}