 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 16, No. 1, March/April, 2011, pp. 19-25 Gunshot injuries: A Tanzanian experience in a Teaching hospital in the Lake Zone P.L. Chalya1, M. Mchembe2. J.B. Mabula1. E. S. Kanumba1, J.M. Gilyoma1 1Department of Surgery, Weill- Bugando University College of Health
Sciences, Mwanza, Tanzania Correspondence to: Dr Phillipo Leo Chalya: drphillipoleo@yahoo.com Code Number: js11003 Background: Gunshot
injuries (GSIs) are a unique form of trauma that are on increase all over the world and
contribute significantly to high morbidity and mortality. The aim of this study
was to evaluate the incidence, injury characteristics and treatment outcome of
GSI in our local setting and to suggest preventive strategies as well as
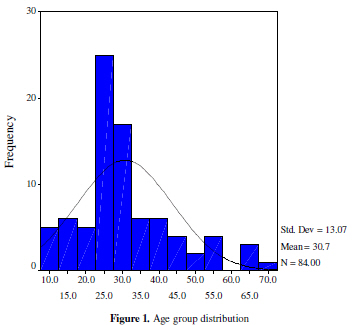
treatment protocols. Introduction Gunshot injuries (GSI) are a unique form of trauma that is potentially devastating and associated with substantial emotional, physical and financial burden on community and hospital resources 1. GSI causes profound morbidity due to prolonged hospitalization, high cost of heath care, loss of productivity and reduced quality of life and above all death1, 2. Globally, the incidence of gunshot injuries is on increase and has wide regional variations, approaching an epidemic level in other parts of the world 3-5. In the United States, approximately 115,000 gunshot injuries with 40,000 deaths occur every year 6. Similarly, in United Kingdom (UK) gun crimes are causing increasing number of severe injuries 7. In South Africa an estimated 127 000 people per year seek treatment for gunshot injuries at state hospitals and there are approximately 20 000 firearm-related fatalities annually – far exceeding the number of fatalities associated with motor vehicle accidents and resulting in enormous costs to the country 8. Tanzania, one of the countries in Africa that has maintained a history of peace and political stability since independence, has recently witnessed an increase in the incidence of GSI due to armed robbery attacks and violence 9. However, the national incidence in Tanzania is not known. Such rise is more glaring in urban areas especially in large and fast growing cities of which Mwanza is a typical example. The commonest cause of gunshot injuries in developed countries is suicidal attempt 10-12. However, armed robbery is the commonest cause of gunshot injuries in most developing countries 12,13. The rise in armed robbery and other violent crimes in developing world have been attributed to poverty, unemployment, political instability and unequal distribution of wealth 2, 13, 14. Civilian gunshot injuries usually are caused by low-velocity bullets and result in low morbidity and mortality, as compared with injuries from high-velocity missiles. However, recently, high-velocity weapons are used increasingly, causing more complicated injuries that task the experience of the attending surgeon15. The outcome of treatment of gunshot injury patients may be poor especially in developing countries including Africa where lack of advanced pre-hospital care system and trauma centers together with ineffective ambulance system for transportation of patients from the site if injury to hospital continues to be an area of neglect that prevents optimal trauma care 16. There is scarcity of information in most developing countries on gunshot injuries where greater emphasis has been placed on injuries related to Road traffic accidents, which are more common. This study was undertaken to evaluate the incidence, injury characteristics and treatment outcome of gunshot injuries in our environment and suggest preventive strategies as well as treatment protocols. Patients and Methods This was a five-year combined retrospective and prospective study of gunshot injury patients that presented to the Accident and Emergency of Bugando Medical Centre (BMC) between April 2006 and March 2010. BMC is a tertiary care hospital in Mwanza City that also receives patients from its six neighboring regions around Lake Victoria. It is a 1000 bed, consultant and teaching hospital for the Weill-Bugando University Collage of Health Sciences (WBUCHS) and other paramedics. The subjects of this study included all patients that presented to BMC with gunshot injuries during the period studied. The details of patients who presented from April 2006 to March 2008 were retrieved retrospectively from patient registers kept in the Medical record departments, the surgical wards, and operating theatre. Patients who presented to the A & E department between April 2008 and March 2010 were prospectively enrolled in the study after signing an informed written consent for the study. Patients with incomplete data and those who were brought in dead were excluded from the study. Ethical approval to conduct the study was obtained from the WBUCHS/BMC joint institutional ethic review committee before the commencement of the study. All recruited patients were first resuscitated in the A&E department according to Advanced Trauma Life Support (ATLS). From the A & E department, patients were taken into the surgical wards or the intensive care unit (ICU) from where necessary investigations were completed and further treatment was instituted. The information gathered from patients included; demographic data, circumstances leading to shooting, time and place of injury, time interval between injury and reception of care, mode of arrival in the hospital, anatomical site of injury, gunshot wound characteristics, type of injury, treatment modalities and outcome measures ( i.e. length of hospital stay, complications and mortality). The types of gun used were assessed according to the severity of the injury on clinical examination and the type of missiles seen on the radiographs and were classified into low and high –velocity weapons. Data was collected using a pre-tested coded questionnaire and analyzed using SPSS computer software version 11.5. A p-value of 0.05 was considered statistically significant. Results During the period under study, a total of eighty-four patients with 92 gunshot injuries (an average of 1.1 injuries per patient) were enrolled giving an average of 17 gunshot injuries annually. There were 79 (94.0%) males and females were 5 (6.0%) with a male to female ratio of 15.8:1. Their ages ranged from 9 to 71 years with a mean of 30.68 ± 13.07 years. The modal age group was 21-30 years (Figure 1). The majority of patients (59; 70.2%) had either primary or no formal education. Most of patients (68; 81.0%) were unemployed. The majority of the gunshot injuries were intentional in 78 (92.9%) and were caused by armed robbery in 66 (84.6%) and by assault in 12 (15.4%) patients. The remaining six (7.1%) patients had unintentional injuries as a result of accidental discharges either by the patients themselves or from others. There were no cases of suicidal or indeterminate intent. The majority of patients (80; 95.2%) were shot during night hours. Most cases of GSI were sustained on the road 47 (55.9%) and at home 26 (30.9%). This was followed by recreational 5 (6,0%), working places 4 (4.8%) and other places 2 (2.4%).The injuries sustained by 52 (61.9%) of patients were suggestive of low-velocity injuries and 10 (11.9%) patients had injuries suggestive of high-velocity injuries. The type of injury was not documented in 22 (26.2%) patients. Fifty-eight patients (69.1%) presented at the Accident and Emergency within 6 hours of injury, while sixteen (19.0%) and ten (11.9%) patients presented between 6 and 72 hours and beyond 72 hours of injury respectively. Regarding the mode of travel to the hospital, 57 (67.9%) patients were brought in by friends, relatives or Good Samaritans, 20 (23.8%) patients by the police, and only 3 (3.6%) patients by ambulance. The mode of arrival was not documented in 4 (4.8%) patients. The frequency of sites of injuries were as follows: Lower limbs 32 (34.8%), upper limbs 27 (29.3%), chest 14 (15.2%), abdomen 10 (10.9%) and lumbosacral spine 1 (1.1%). Fifty-six (60.9%) patients had only single entrance wound and thirty-six (39.1%) patients had multiple entrance wounds. Sixty-two (67.4%) patients had exit wounds and in thirty (32.6%) patients the bullet had remained lodged in the body. The majority of gunshot wounds were punctured wounds (52; 56.5%) and lacerations (22; 23.9%). This was followed by crush wounds and finger amputation in 5 (5.4%) and 2 (2.2%) of cases respectively. Soft tissue injuries (92; 100%) and fractures (42; 45.7%) were the most common type of injuries sustained. Haemopneumothorax, major vascular injuries and neurologic deficit occurred in 9 (12.5%), 4 (5.5%) and 1 (1.4%) of patients respectively Injury severity score (ISS) was recorded in patients who were studied prospectively. The overall ISS ranged from 1-45 with a mean of 18.00. The majority of patients had minor to moderate injuries (ISS < 16) and accounted for 62.9%. Severe injuries accounted for 37.1%. Twelve (14.3%) patients were treated conservatively with simple wound dressing, broad antibiotics, tetanus prophylaxis and analgesics and discharged through the Accident and Emergency department. The remaining seventy-two patients (85.7%) were admitted and underwent definitive surgical treatment. Table 1 shows details of treatment modalities. Sixteen out of the admitted group (22.2%) were admitted to ICU; of these, nine (56.3%) patients were subjected to ventilatory support. Table 1. Treatment Modalities
Abbreviations: ORIF = Open reduction and internal fixation, EF= External fixation, POP = Plaster of Paris, UWSD = Underwater seal drainage Table 2. Complications of gunshot injuries
Thirty-two (38.1%) patients developed 57 complications. Wound infection and complications of fractures were the most common complications accounting for 49.1% and 21.1% of cases respectively. The details of complications are shown in Table 2. The duration of stay in hospital ranged from one to 186 days with a mean of 34.2 days. Patients with limb injuries associated with long bone fractures were found to have longer hospital stays (p-value < 0.001). In this study, seven patients died giving a mortality rate of 8.3%. Three deaths resulted from head injuries, two from chest injuries and one each from tetanus and septic shock respectively in patients with lower limb injuries. Mortality rate was high among patients with head and chest gunshot injuries compared to gunshot injuries involving the limbs (71.4% versus 28.6%) and these differences were significant (p-value < 0.001). The mortality was also significantly high in patients who were admitted to ICU (p-value < 0.001). The outcome of gunshot wounds was good in 69 patients (82.1%), who were successfully treated and discharged. Six patients (7.1%) discharged themselves against medical advice. Two patients (2.4%) were referred to neurosurgeons because of severe penetrating head injury and spinal injury with paraplegia. Discussion Gunshot injuries constitute a global public health problem and pose therapeutic challenges to trauma and general surgeons all over the world 1-5. The incidence of civilian gunshot injuries has been reported to be on the increase globally 2, 17, 18. Increased incidence of GSIs in most developing countries has been attributed to poverty, unemployment, political instability and unequal distribution of wealth 2,13,14. This is reflected in the high rate of GSIs in our patients, majority of whom, were unemployed and uneducated. In the present study, an average of 17 gunshot injuries annually was observed during the five years of study. These figures were low comparable to that reported by other studies 2, 17, 19. These differences reflect differences in the rate of social and interpersonal violence from one country to another. The low figures in our study may actually be an underestimate and the magnitude of the problem may not be apparent because many cases are not reported for fear of been arrested by police. . Several other cases may also have been treated in private hospitals which were not included in the present study. Death at the scene of shooting and those who were brought in dead were excluded from the study and this may have contributed to the underestimation of the magnitude of the problem. In the present study, gunshot injuries were found to be most common in the third decade of life and tended to affect more males than females, with a male/female ratio of 15.8:1 which is comparable with other studies 2, 8, 14, 17, 19, 20. This observation can be explained by the fact that male youths are generally more adventurous and are more often involved in interpersonal violence and are indeed the principal perpetrators of civil conflicts and armed robbery. The majority of the gunshots in this study were intentional, mostly from armed robbery attacks and assaults during interpersonal conflicts and most of shooting occurred on the highways and in the home. The preponderance of armed robbery and assaults as causes of gunshot injuries in this study had been noted in previous studies 19, 21. The reasons for this observation may be due to harsh economic climate, rising unemployment rate and ineffective law enforcement and failure of successful poverty eradication programmes in Tanzania. We also noted that the majority of shooting occurred during night hours. Similar nocturnal prevalence had been reported by Weaver et al 22. Night may have afforded the armed robbers the cover of darkness to make their identification difficult, it was also a period when their targets are more likely to be at home. Low-velocity injuries have been reported to predominate in civilian practice 7, and we have found the same with 61.9% of our injuries being low-velocity. Similar finding was also reported by other studies done elsewhere 2, 7. In the civilian environment, patients are generally clean and present with low-velocity wounds (i.e. wounds from a handgun) and can often report the type of weapon used. This has lead to a conservative approach being adopted in the management of these wounds. The low incidence of high-velocity injuries in our study can be explained by the fact that these injuries are usually fatal and the majority of patients with these injuries usually die before reaching the hospital. The prehospital care of trauma patient has been reported to be the most important factor in determining the ultimate outcome after the injury 2, 16. None of our patients had pre-hospital care; as a result the majority of them were brought in by relatives, Good Samaritan and police who are not trained on how to take care these patients during transportation. Only three patients in this study were brought in by ambulance. This observation is common to many other developing countries1, 9, 13, 14, 16, 21. The lack of advanced pre-hospital care and ineffective ambulance system for transportation of patients to hospitals are a major challenges in providing care for trauma patients in our environment and have contributed significantly to poor outcome of these patients. This study showed that the lower extremities were mostly affected. This is in keeping with other studies which attributed this phenomenon to the intent to demobilize victims by gunshot injuries 2, 15, 17, 19, 20, 21. For the present study, a more likely explanation is that because most of the injuries to other body regions were immediately fatal, the patients who sustained these injuries may have died at the scene of shooting before brought to the hospital. This pattern is not surprising because of the uncommon suicide and attempted suicide gunshots in our environment in contradiction to countries with a high suicide rate such as the United States where the weapon is typically aimed at the head or heart. The low incidence of injuries involving the head, neck, chest and abdomen in our studies can be explained by the fact that injuries involving these sites are usually fatal and the majority patients with these injuries usually die before reaching the hospital. The increased rate of gunshot injuries to the limbs suggests the need for the attending surgeon to have adequate skill to manage vascular injuries which could occur in the gunshot injuries to the limbs. This will minimize or eliminate the immediate or chronic complications that that can follow such injuries. Most of patients in this study sustained soft tissue injuries and open fractures, and punctured wounds and lacerations were the most common type of gunshot wounds. Similar injury patterns were also reported by other authors 2, 17, 19, 20, 21. A good knowledge of the nature and type of gunshot wounds allows the clinicians to understand the type gun used and this is of great importance for medico-legal purposes and surgical treatment. Based on experience in other studies, low-velocity injuries can be managed on an outpatient basis provided there is no associated fracture or neurovascular injury. Patients with high velocity injuries usually present with severe tissue injuries which may be associated with neurovascular and fractures need hospitalization and are treated with a thorough tissue debridement with removal of all dubious and devitalized soft tissue and bones 7, 20, 21. In our study, 14.3% of patients with low-velocity were treated conservatively as outpatients with simple wound dressing, broad antibiotics, tetanus prophylaxis and analgesics and discharged through the Accident and Emergency department with no complications. Patients with high-velocity injuries were treated with a thorough tissue debridement with removal of all dubious and devitalized soft tissue and bones. Chest and abdominal injuries are commonly associated with severe blood loss and hypovolaemia necessitating blood transfusion and emergency surgical interventions. In a resource-poor setting like ours trauma surgeons depend on good clinical judgment; it is our practice to do mandatory prophylactic underwater seal drainage and exploratory laparotomy in all cases of penetrating gunshot injury of the chest and abdomen. We have not found the advocated selective conservative management useful in managing perforating gunshot wounds of the chest and abdomen. In agreement with other studies done elsewhere 7, 19, wound infections and complications of fractures were the most common complications of treatment of gunshot injuries. Therefore, early and meticulous wound care should continue to be instituted in the management of gunshot injuries. The mean duration of hospital stay in this study was found to be longer than that reported by other authors15, 19, 20. This can be explained by large number of patients with limb injuries associated with long bone fractures which usually need long duration of hospitalization. The current study had a mortality rate of 8.3%, which is comparable with that reported by Kalemoglu et al 15 and slightly higher than the rate quoted by Katchy et al 23. The highest mortality rate was recorded among patients with chest, intestinal and head injuries. Prolonged hospitalization, need for major surgeries and the cost of care were the major cause of morbidity in this study. These calls for urgent firearms control surveillance. The lack of efficient emergency health care services for pre-hospital care and rapid transport of injured victims to hospital which results in possibly ‘preventable deaths’ are also major factors contributing to increased morbidity and mortality in our environment. Conclusion and Recommendations Gunshot injuries have become a major cause of morbidity and mortality among young males in our society where resources for prehospital and hospital trauma care are limited, and armed robbery attacks and interpersonal violence are the major causes of these injuries. Inefficient firearm control, high rates of unemployment, poverty and substance abuse have been reported to be responsible for increasing incidence of youth restiveness, armed robbery and associated gunshot injuries in our society. Addressing the root causes of violence such as poverty, unemployment, and substance abuse will reduce the incidence of gunshot injuries in our environment. Establishment of efficient emergency health care services for pre-hospital care and effective ambulance system for rapid transport of injured victims to hospital will reduce morbidity and mortality associated with these injuries Acknowledgement We acknowledge to all members of staff in the Department of Surgery, Bugando Medical Centre who contributed to the study References
Copyright 2011 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js11003t1.jpg] [js11003f1.jpg] [js11003t2.jpg] |
| |||||||||

{kind=link}