 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 16, No. 1, March/April, 2011, pp. 26-30 Prevalence, Nature and Characteristics of External Congenital anomalies at Mulago Hospital J. Ochieng, H. Kiryowa, I. Munabi, C.B.R. Ibingira. Makerere University, Faculty of Medicine Department of Anatomy, P.O Box 7072, Kampala-Uganda Correspondence to: Dr. Charles Ibiingira, cibingira@yahoo.com Code Number: js11004 Background: Congenital
anomalies may be structural, behavioral, functional or metabolic defects
acquired before a baby is born and their nature and type are highly dependent
on the causative agent as well as the time when they are first diagnosed. There
was a need to identify the different defects present at birth among Ugandans in
order to appreciate the magnitude of each and its eventual effect on the
affected individual. The aim of this study was to determine the prevalence,
nature and characteristics of external congenital anomalies in live born babies
at Mulago hospital. Introduction Congenital anomalies may be structural, behavioural, functional or metabolic defects acquired in utero and their nature and type are highly dependent on the causative agent as well as the time when they are first diagnosed1-3. These disorders can affect almost each organ or organ system and their characteristics, incidence and prevalence depend on either genetic make-up of the individual, environmental factors surrounding the individual or a combination of both and their prevalence many times varies from region to region3-7. External and internal congenital anomalies like sickle cell anaemia, blindness, heart defects, limb defects, facial clefts and many others continue to be a challenge to the Ugandan health system and the general public as well although the magnitude of the different defects has not been adequately documented around the nation8. There was a need to identify the different external defects present at birth in order to appreciate the magnitude of each and its eventual effect on the affected individual with documentation hoping to aid effective and planned health service delivery to the affected individuals. This study was aimed at determining the prevalence, nature and characteristics of external congenital anomalies in live born infants at Mulago Hospital. Patients and Methods This was a cross sectional descriptive study conducted at the post natal ward and Special Care Unit of Mulago Hospital, Kampala Uganda. All new born babies over a period of four months were examined and evaluated for external congenital anomalies. This was by taking history from the mother just before discharge from the post natal ward, followed by a physical exam of all the baby’s systems to identify any external congenital anomalies which were eventually documented. Ethical review and approval was sought from the Faculty of Medicine Research and Ethics Committee and Mulago Hospital Research and Ethics Committee before the study was conducted. Informed consent was obtained from the mothers before their babies could be included in the study. Mothers of babies that needed specialized treatment were advised accordingly and referred for appropriate care. Results Out of 754 new born babies there were 52.8% males, 47.0% females and 0.2% hermaphrodite. The male to female ratio was 1: 1.12. Table 1. Distribution of External Congenital Anomalies According to Sex of Baby
Table 2. Types of External Congenital Anomalies in New Born Babies at Mulago.
Table 3. Types of limb anomalies
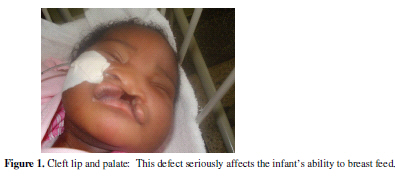
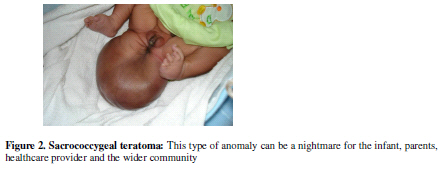
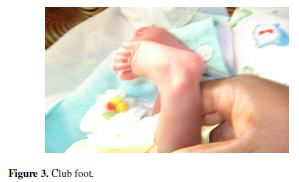
Thirty three babies had external congenital anomalies although the total number of external anomalies recorded was 35 because two of the babies had two external anomalies each. 20 of the babies with these anomalies were males, accounting for 5.02% of all males while 12 were females, accounting for 3.40% of all females. One baby was a hermaphrodite, accounting for 0.2%. The overall prevalence of live born infants with external congenital anomalies was 4.4%. The different anomalies involved limbs anomalies (45.7%), lips and palate (14.2%), spina bifida (8.5%), Omphalocele (5.8%), CNS (5.8%), and others included sacrococcygeal teratoma (Figure 1), hyperextended neck, paraphimosis, penile hypoplasia, mandibular hypoplasia, folded ear and a birth mark. Many of the anomalies were major while some were life threatening and required surgical repair at one point in the near future. As shown in Table 1, 52.8% of the babies were males and 47.0% were females. 0.2% was for the hermaphrodite. Of the 398 males studied, 20 had external congenital anomalies giving a prevalence of 5.02%. 12 out of the 355 female babies involved in the study had an external anomaly giving a prevalence of 3.4%. One baby was a hermaphrodite and accounting for of 0.2%. Thus the overall prevalence of the external congenital anomalies in all new born babies was 4.4%. There were a total of 33 babies with external congenital anomalies implying that 4.4% of all new born babies had an external congenital anomaly. Two of these babies had multiple anomalies, giving a count of 35 anomalies hence the total prevalence of all anomalies was 4.64%. Many anomalies involved limbs, accounting for a total of 45.7% and these included club foot (17.1%), polydactyly (11.4%), congenital hip dislocation (8.5%), hyper extended knee (2.9%), syndactyly (2.9%) and meromeria (2.9%) of all the observed anomalies. Club foot was one of the commonest congenital anomalies. Discussion Congenital anomalies constitute a high proportion of new born babies in this population which was 4.4% despite the fact that the study concentrated only on external anomalies, with a possibility of higher percentages if internal anomalies were reviewed. This is also true because, many external congenital anomalies have other associated internal anomalies and may occur as multiple defects in the same individual3. For instance a hermaphrodite may have non-functional gonads. Since the prevalence of anomalies was 5.02% among male and only 3.4% among females, this implied that among the research participants that were involved in this study, the chances of having an anomaly were much higher for males as compared to their female counterparts. The commonest single anomalies observed during the study was club foot which affected six children and constituted 17.1% of all the anomalies that where observed while other limb anomalies registered included polydactyl which comprised more that 11% of all the cases of congenital anomalies, congenital hip dislocation contributed 8.57% and a couple of others. It is therefore not surprising to have limb anomalies contributing more than 45% of all the cases recorded. This distribution is also comparable to other studies done elsewhere9. Cranio-facial defects have also been noted to be very prevalent contributing about 23% of all case of congenital anomalies and distributed as cleft lip and palate 14.3%, while hydrocephalus, mandibular hypoplasia and folded ears each contributed 2.9%. It should be noted that some of these anomalies particularly cleft lip and palate can be a big threat to the survival of the infant because normal breast feeding is affected. Meningeo-vertebral defects including sacrococcygeal teratoma and spina bifida had four cases contributing to 11.4% of all cases of congenital anomalies at birth. This is a big number given that many affected children end up with a very poor quality of life for ever. Urogenital disorders included penile hypoplasia, paraphimosis and hermaphrotidism all of which contributed 8.57%. These types of anomalies can be a nightmare for parents of children especially where sex determination is important for cultural practices including naming of a child, because hermaphrodite children may not have their sex determined till much later10. However, more distressful anomalies of the urogenital system such as bladder exystrophy and uretero fistulae were not registered by the study. The cases that needed most urgent attention included the two babies with omphalocele, cleft lip and palate, sacrococcygeal teratoma, paraphimosis and to some extent hydrocephalus. This implies that many of these anomalies are actually life threatening and if not adequately managed may result in death of the infant. Their occurrence is a strain on the health delivery system to be able to handle such cases as they come with utmost care and professionalism despite the chronic challenge of both financial and skilled human resources. Only one anomaly can be classified as a minor anomaly on the basis that it may not affect function or appearance, and may not require surgical intervention3. This anomaly was the birth mark and it contributed to 2.9% of all the anomalies. The remaining 34 (97.1%) anomalies were major anomalies on the basis that they have an effect on function as well as appearance. This is in contrast to previous studies that gave a prevalence of minor anomalies at 21% and major anomalies at 2%4-7. Thus, the prevalence of major anomalies in new born babies at Mulago hospital is by far much greater than the prevalence of minor external congenital anomalies. This total prevalence is high in a low resource country with a per capital expenditure on health which is less than US $20. Conclusion and Recommendations The most prevalent external anomalies were limb defects followed by cranio-facial anomalies both of which constituted more than 68% of all cases. If not well managed, majority of these anomalies can greatly affect the quality of life of the individual. Hence need for appropriate and timely care to reduce on the magnitude of suffering the anomaly would otherwise have caused to the individual, family and the wider community. Acknowledgement We appreciate the financial assistance by Sida/SAREC which enabled this study to be conducted. Our thanks go to the staff Department of Anatomy Makerere University and the staff of Department of Obstetrics and Gynecology Mulago Hospital. We also appreciate our participants the new mothers and their babies without which the study would not have been possible. References
Copyright 2011 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js11004f3.jpg] [js11004t2.jpg] [js11004t1.jpg] [js11004f2.jpg] [js11004t3.jpg] [js11004f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}