 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 16, No. 1, March/April, 2011, pp. 57-64 Bladder Tumours at Tikur Anbessa Hospital in Ethiopia. H Biluts1, E Minas2 1General Surgery unit, Department of surgery, MF, AAU. Correspondence to: Dr H. Biluts, Tikur Anbessa Hospital, P.O.Box 9086, Addis Ababa, Ethiopia E-mail: hagosisnow@yahoo.com, surgery@ethionet.et Code Number: js11009 Background: Bladder cancer is
the fourth to fifth most common cancer in men, and the eighth in women These
t umors are commonest in the 50
to 70 year age group The aim of this
study was to review the pattern and surgical management of bladder tumors at
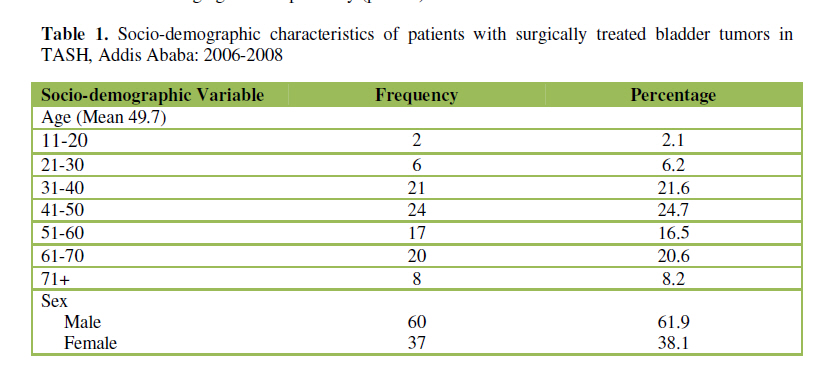
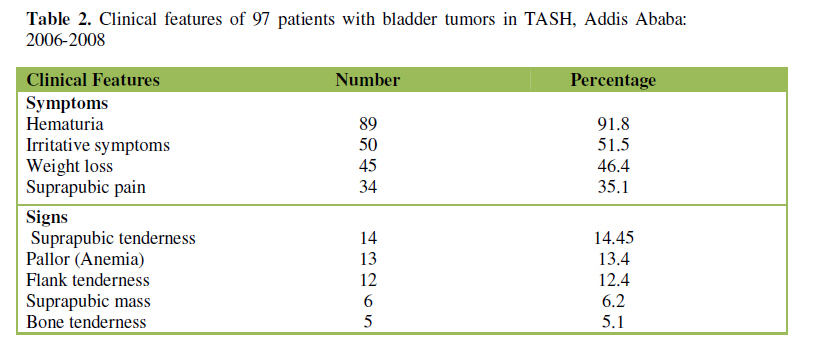
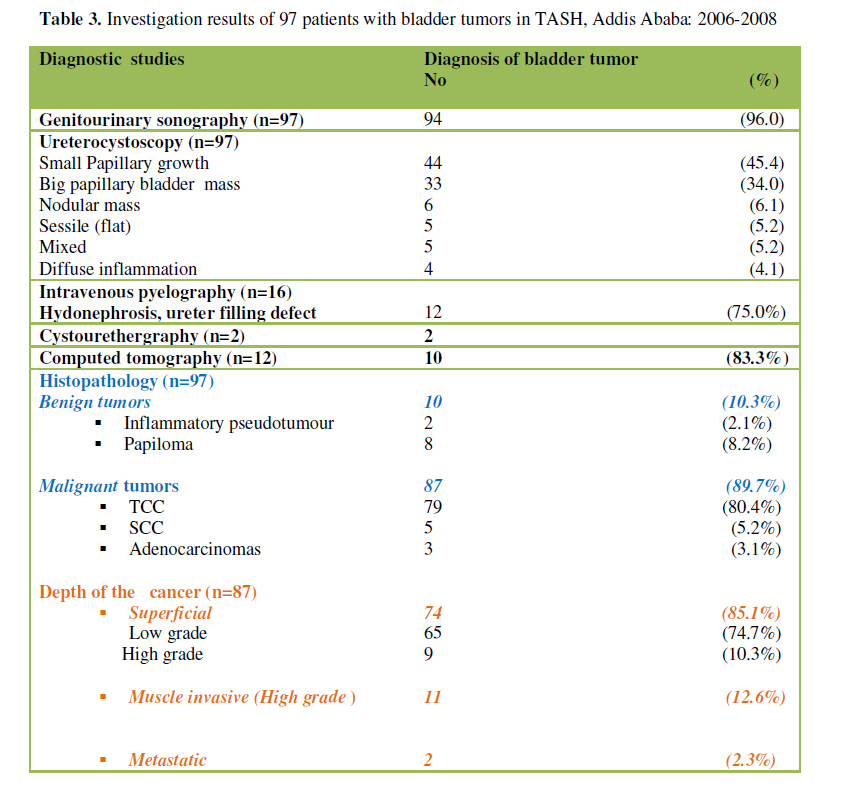
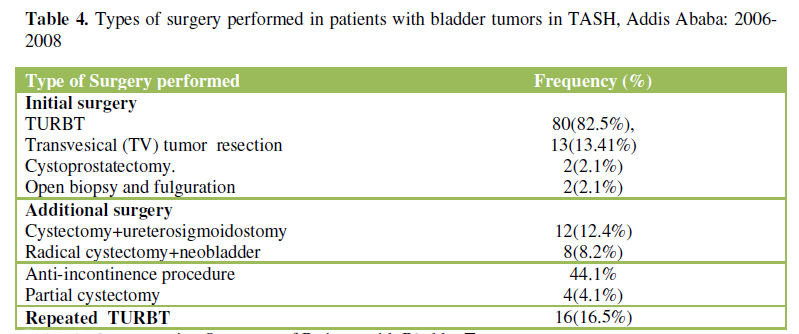
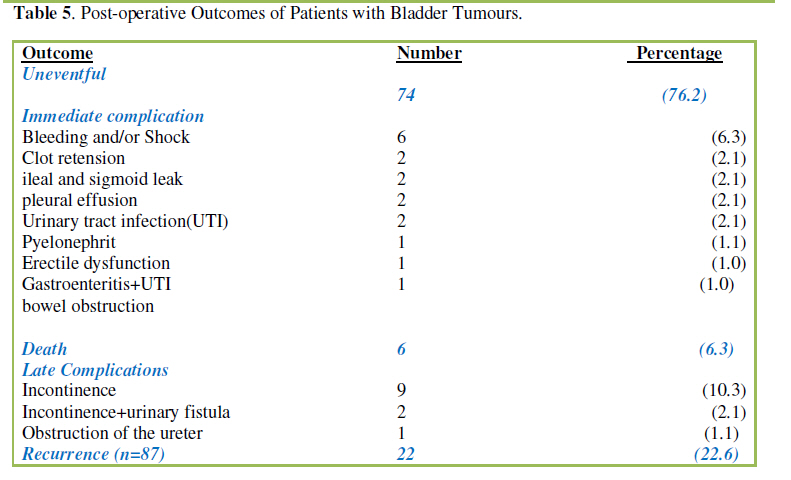
TAS in Ethiopia. Introduction Bladder cancer is a common urologic tumor, affecting about 1 in every 2,500 people per year throughout the western world. They are commonest in the 50 to 70 year age group, and are twice as common among men as women. Bladder cancer is the fourth to fifth most common cancer in men, and the eighth most common in women1-5. In developed countries 90% of bladder tumors are urothelial cell or transitional cell carcinoma (UCC or TCC).The other 10% of tumors are Squamous cell carcinoma(SCC)(5%), adenocarcinomas(<2%), sarcoma, small cell carcinoma and secondary deposits from cancers elsewhere in the body. but in developing countries 75% are SCC, mostly due to schistosomiasis6. Bladder cancer characteristically causes blood in the urine, and is often painless. Sometimes blood clots may form and cause pain or obstruction to the flow of urine. Other possible symptoms include dysuria, polyuria or urgency. Bladder cancer is rarely found during a physical examination. Occasionally, an abdominal or pelvic mass may be palpable3,7,9 The gold standard of diagnosing bladder tumors is urine cytology and transurethral cystoscopy. Cytology is very specific (a positive result is highly indicative of bladder cancer) but suffers from low sensitivity14. There are newer urine bound markers which are more sensitive but not as specific as urine cytology2,8,9. The treatment of bladder tumors depends on how deep the tumor invades into the bladder wall. Superficial tumors can be "shaved off" using an electrocautery device attached to a resectoscope. BCG instillation is also used to treat and prevent the recurrence of superficial tumors10,11. BCG immunotherapy is effective in up to 2/3 of the cases at this stage. Instillations of chemotherapy, such as valrubicin (Valstar) into the bladder can also be used to treat BCG-refractory CIS disease when cystectomy is not an option. Tumors that infiltrate the bladder require more radical surgery where part or the entire bladder is removed (a cystectomy) and the urinary stream is diverted. In some cases, a neobladder from a segment of intestinal tissue, but this largely depends upon patient preference, age of patient, renal function, and the site of the lesion7,8-13. A combination of radiation and chemotherapy can also be used to treat invasive disease. The objective of this study is to review the pattern and surgical management of Bladder tumors in Tikur Anbessa Specialized Hospital (TASH). Patients and Methods The study is a retrospective hospital based type. Of 121Adult patients admitted to the TASH for a surgical treatment of bladder tumors between January2006 and December 2008 the medical records of 97 (80.0%) patients were retrieved and included in the study. Data concerning their socio-demographic status, history and clinical findings during admission, laboratory examination, cystoscopic, ultrasonographic and radiological studies, intra-operative findings and operative procedures, post operative course and final out comes were collected using structured format prepared for this purpose. The operation theatre registry was also used to complete the data. Analysis was done using computer based statistical software SPSS version 11.0. Difference in proportions were examined using Chi-square test with its conventional criterion for statistical significance (p<0.05). We adopted the WHO 28 grading classification of bladder cancers as papillary neoplasm of low malignant potential (PNLMP), low grade (grade 1 and 2) or high grade (grade 3) and the 1997 TNM staging system37. We employed various surgical techniques for treatments of bladder cancer such as were transurethral resection of bladder tumor (TURBT), cystectomy, biopsy and fulguration. TURBT or fulguration was used for superficial tumors using an electrocautery device. Tumors that infiltrate the bladder required more radical surgery where part or the entire bladder is removed and the urinary stream is diverted such as ureterosigmoidostomy. In some cases, a neobladder was constructed from a segment of intestinal tissue, few had anti-incontinence procedure. Results Of the 97 patients, the majority of patients were males 60( 61.9%); the male to female ratio was 1.6:1 and in their 4th ,5th and 6th decades of life ,with age range between 20 and 79 years.( mean 49.7). Duration of complaints ranged between 1and 48 months with mean of 13.89(Table 1). The most common presenting symptoms were hematuria in 89(91.8%) which is often painless (p<0.001), irritative symptoms (dysuria, urgency and frequency) in72 (74.2%), obstructive symptoms in 38(39.2%) and suprapubic pain in 34(35.1%). Forty five, (46.4%) of the patients claimed to have weight loss, >10% of their body weight (Table 2 shows symptoms and signs). Genitourinary sonography and uretherocystoscopic examination of the bladder were the main modalities of investigation in the diagnosis of bladder tumors, in 94(96.9%) and 97(100%) patients (table 3). Uretherocystoscopic examination of the bladder revealed papillary growth in 77(79.4%) patients. Tumors were multifocal in 25(25.8%) of patients. Histopathologically, 87(89.7%) and 10(10.3%) of the patients had malignant and benign bladder tumors respectively (table3).Of the 87 patients with bladder cancer, 66(75.9%) and 21(24.1%) of the cases had low and high grades respectively (p<0.05), Surgical techniques employed for bladder tumors were TURBT in 80(82.5%), transvesical removal of the mass in 13(13.4%), open biopsy and fulguration in 2(2.1%), cystoprostatectomy in 2(2.1%) patients.(table 4) Forty-four (45%)patients had additional surgery such as repeated TURBT in 16(16.5.%) for recurrent and residual tumors, cystectomy+ureterosigmoidostomy in 12(12.4%) cystectomy+neobladder in 8(8.2%), anti-incontinence procedure(embedding) in 4(4.1%), partial cystectomy in 4(4.1%). Four (4.1%) patients took chemotherapy. In 74(79.4% %) patients the postoperative course was uneventful, whilst 17(24.7%) and 12(12.3%) developed immediate and late postoperative complications respectively (table 5).Most (74.4%) of patients with postoperative complications were treated conservatively and discharged with improvement. The mean and median duration of postoperative hospital stay was 12.09 and 7 days respectively (Range 1-70). Six patients died, making the postoperative mortality 6.2%. Cause of death being multiple organ failure (2), sepsis and septic shock (2), and myocardial infarction (2). Seventy-seven (79.4%) patients were discharged with improvement, while 8 were discharged in the same condition, 4 were discharged against medical advice. Of the 91 discharged patients (excluding 6 in-hospital mortality), 49(54.3%) and 36(39.6%) had follow-up for three and six months respectively, six had no follow-up at all. The follow up period ranged from 1 to 26 months (mean 3.7 months). In total, 22/71(31.0%) patients had recurrence of the tumor. Mean time of recurrence was 8 months (range 2-18 months). Among 87 patients with bladder cancers, 57(65.5%) patients had nonmuscle invasive tumours (stage Ta, Tis [carcinoma in situ; CIS], T1), 27(32.1%) muscle invasive (stage T2, T3), and 3(3.4%) metastatic; 56(66.7%) of the cancers were low grade or well differentiated, and 28(33.3) %) were high grade type. Discussion Tumors of the bladder are commonest in the 50 to 70 year age group, and are twice as common among men as women, but statistically insignificant (p<0.02).In agreement with other authors, our results showed the occurrence of the disease in same age groups with similar peak incidence and predominance of males over females2,9,22.Often painless hematuria that is gross in 80 to 90%, which is the classic presentation of bladder tumors, is in accordance to many authors. Superficial bladder cancer was rarely found during a physical examination 4,22,24,44. Similar to the reports by Steinberg et al and others, the diagnostic capacity of sonography and uretherocystoscopic to see how large the tumour in the bladder is, and to take a small sample from the tumour and CT scan of the abdomen to check for spread of the tumour to areas around the bladder were the golden standared investigations used in our patients2,9,44. The most common type of bladder cancer in the United States and UK is TCC 3,4,6.In developed countries about 90% of bladder tumors are TCC, in developing countries 75% are SCC, mostly due to schistosomiasis6,36,37.In accordance with West DA et al, Cheng L and others3,6-16,17 this review reflected the well-known dictum of the western countries that TCC is the most commonest type of bladder cancer in 77(80.0%) of patients, but in sharp contrast to the findings in developing countries. In Ethiopia, all three known schistosoma hematobium endemic area - in the middle and lower parts of Awash valley, in the lower Wabe Shebelle valley and along Sudanese border in Wellega are below 800m but majority of Ethiopians are highlanders15. Further study is highly recommended to ascertain the above finding. In our review, on cystoscopic inspection and intraoperative evaluation of bladder tumors, 77(9.7%), 10(10.3%) and 6(6.2%) patients had papillary, sessile or mixed and nodular type respectively, this finding agrees well with many reports28. At diagnosis only about 5% of patients have metastatic disease. Gary David Steinberg et al and others reported, 55-60% of patients have low-grade superficial disease, 40-45% high-grade disease, of which 50% is muscle invasive 3,19. Similarly, our review revealed low grade (75.9%) tumours were significantly predominant over high grade (24.1%) tumors (p<0.05). Over all around 25% have involvement of the muscle layer; the remaining 70% have superficial disease of which 10% is carcinoma in situ [9, 20, 30, and 31]. Our findings are also in accordance the above reports. The treatment of bladder cancer depends on how deep the tumour invades into the bladder wall. For superficial tumors (CIS, Ta or T1) TURBT is required. Immunotherapy in the form of BCG instillation is also used to treat and prevent the recurrence of superficial tumours 10, 23. In the present review, initial TURBT was performed in 80(82.5%) of the cases. None of the patients received immunotherapy, simply because the facility is not available at TASH. Only four patients had received chemotherapy, and tumors that infiltrate the bladder require more radical surgery and the urinary stream is diverted. In some cases, creation of a substitute bladder (a neobladder) from a segment of intestinal tissue is necessary29. Initial transurethral resection and fulguration, with or without immediate postoperative chemotherapy, followed by intensive cystoscopic surveillance are the most common conservative forms of management 19, 43. A retrospective series by Herr HW et al (1998) and others addressed the value of performing a second TURBT within 2 to 6 weeks of the first 25-27. A second TURBT performed on 58 patients with T1 disease found that 14 patients (24%) had residual (T1) disease and 16 patients (28%) had muscle invasion (T2). In agreement to our review the residual tumor rate on repeated TURBT was 25.8% in the transurethral resection 39, and found to have T1 and T2 diseases. Totally 47.4% of the patients with bladder tumours had initial or additional radical surgery. Patients that required more aggressive forms of treatment were those with extensive multifocal recurrent disease and muscle invasive stage of the tumour. For stage 2 and 3 (T2 and T3) the operation is radical cystoprostatectomy. An anterior pelvic exenteration is performed on women with disease involving the muscle layer. After removal of the bladder urinary diversions are created from various segments of bowel. An ileal conduit is the most commonly used9. Similarly, most common radical surgical techniques employed for higher stages and muscle invasive tumours were cystectomy+ureterosigmoidostomy,cystectomy+neobladder,anti-incontinence procedure, partial cystectomy and cystoprostatectomy in their order of frequency. A follow- up range from 2 to24 months (mean 3.7 months) is too short compared to 8 and 20 years30,31. This can be explained by simple fact that once patients are discharged, they cannot afford to come back for follow-up from very remote area due to economic constraints. Some others patients might have died at home. Recurrence is seen in 60-70% of non-muscle invasive tumors30,31,38 of which 20-30% progress to a higher stage or grade20,34.In a series of patients with Ta or T1 tumors who were followed for a minimum of 20 years or until death, the risk of bladder recurrence following initial resection was 80%3,32,33. Chen CH, et al (2007) reported a recurrence rate of 70% within 5 years40. Our study revealed an over all recurrence rate of 25.3% at mean follow-up duration of 3.7 months (16 local, 4 nearby area, 2 distant). This low recurrence rate of bladder tumours are underreported and don’t reflect the facts that is demonstrated by many authors32, 39 and could be due insufficient follow-up period. In this review, higher rates of mortality were noted compared to the perioperative mortality rate of 1 or 2% in total cystectomy9.An over all complication rate of 29.3% and urinary incontinence of 10% are comparable to the report by Steinberg G who reported that radical cystectomy has a complication rate around 25% and risk of daytime incontinence of 10%, rising to 15% at night9. Conclusion and Recommendation Consider all patients with gross haematuria and unexplained microscopic haematuria to have bladder cancer until proven otherwise (P<0.005).The most common type of bladder cancer in Tikur Anbessa Hospital is transitional cell carcinoma (P<0.05). The commonest procedure for bladder tumours was TURBT (p<0.001) Following TURBT, careful surveillance of subsequent bladder tumor progression is important. References
Copyright 2011 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js11009t4.jpg] [js11009t1.jpg] [js11009t2.jpg] [js11009t3.jpg] [js11009t5.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}