 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 16, No. 1, March/April, 2011, pp. 74-79 Closed Mitral Valvotomy-a Life Saving Procedure in Facility Deprived Countries: Experience at Muhimbili National Hospital, TANZANIA. E.V. Ussiri1, E.T.M. Nyawawa1, W.B.C. Wandwi1, W. Jiang1, B.J. Nyangassa1, U. Mpoki2, E.R. Lugazia2, T. Waane3, P. Chillo3, M. Janabi3, H. Mwandolela3, G. Mlay4, S. Kubhoja4, P.R. Kisenge3, T. Shem3, J. Bgoya5, W. Mahalu6. 1Consultant
Cardiothoracic Surgeon, Muhimbili National Hospital, P. O. Box 65000 Dar es
Salaam, Tanzania. Correspondence to: Dr Ussiri EV, E-mail: eussiri@yahoo.com) Code Number: js11013 Background: Rheumatic heart disease
remains a major health cardiac problem in developing countries as the culprit
of rheumatic fever. Mitral valve stenosis is the most common complication of
valvular heart disease and its consequences of increase in pulmonary
hypertension, heart failure, pulmonary vascular disease and if untreated death
ensues. The management of this condition varies depending on availability of
expertise and resource; however in a facility deprived country with low
economic status closed mitral valvotomy remain the standard palliative
treatment! The aim of this study was to evaluate the clinical status of
patients with mitral stenosis following closed mitral valvotomy treated at
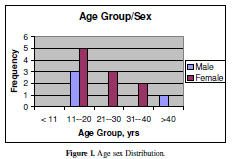
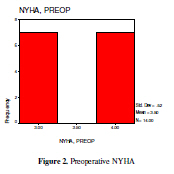
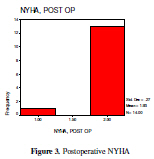
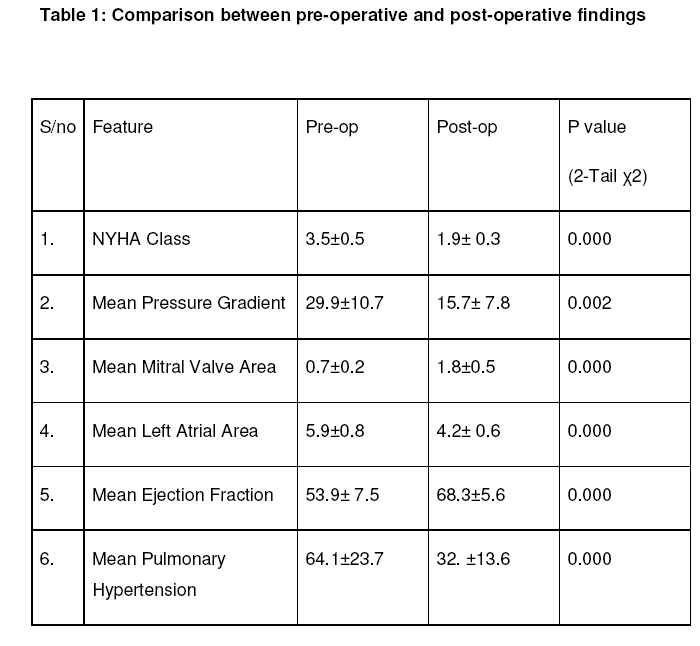
Muhimbili National Hospital, Cardiothoracic Unit. Introduction Acquired Mitral valve stenosis is the sequela of rheumatic heart disease due to rheumatic fever which is commonly seen in developing countries and no longer in developed countries1,2,3,4,5,6. Definitive treatment for rheumatic mitral valve stenosis is valve replacement which can be either mechanical or biological. Biological prosthetic valve is mainly applied for age group above 65 years and child-bearing females and not in young age due to its progressive degeneration leading to re-do operation. Mechanical prosthetic valve will require life-long anticoagulation with warfarin to prevent valve thrombosis as well as thrombo-embolic phenomenon1,3,7. Percutenous Balloon Mitral Valvotomy is the palliative modality of choice but, technically difficult, expensive and not easily available in most of the developing countries and therefore, closed mitral valvotomy remains the modality of choice in these low and middle income (limited resources) countries1,3,4,5,6. Closed Mitral Valvotomy is contraindicated if there is a significant mitral valve regurgitation of more than grade II, leaflet calcification, chordal thickening, endomyocardial fibrosis and presence of clot4, 8. The prospective study was done to evaluate the preoperative and postoperative status following closed mitral valvotomy in patients who had severe mitral valve stenosis at Muhimbili National Hospital. Patients and Methods A Prospective study on Closed Mitral Valvotomy was done at Muhimbili National Hospital for 18 months from May 2008 to November 2009. Fourteen patients including 4 male (28.6%) and 10 female (71.4%) were recruited. The mean age was 21.5± 8.8 years (range 11-41 years). The diagnosis was based on clinical and trans-thoracic 2D- Echocardiography findings. During echocardiography patients were evaluated for left ejection fraction and fraction of shortening to determine the ventricular function, the severity of mitral stenosis was assessed on the mitral valve cross sectional area and the mean pressure gradient across the valve. Any evidence of diastolic dysfunction was assessed using the E/A ratio. Patients with severe mitral valve regurgitation, and leaflet calcification were excluded from the study. Patients fulfilling inclusion criteria were counseled and explained about their disease process. They underwent laboratory investigations and were admitted for the surgical procedure. Surgical Technique All patients had general anesthesia with endotracheal tube intubation; patients were positioned in right lateral recumbent position, after skin preparation and draping with sterile towels the thoracic cavity was approached through Left Antero-Lateral Thoracotomy, and through 4th Intercostal space. Downward traction of the upper lobe of the lung was done and the pericardium was found. The vaso-phrenic bundle was identified and stay suture were applied anterior to the bundle and in parallel, the pericardium was opened and retracted and hence exposing the heart. The left atrial appendage was identified and a purse string suture was applied, a Satinsk forceps was then applied below the purse string taking care not to injure the left circumflex artery that was in close proximity to the base of the appendage. The appendage was then opened and with purse string controlled on the surgeons’ left hand the right index finger was introduced into the opening and onto the stenotic mitral valve while the assistant removed the forceps. Dilatation was only done using finger while monitoring the systemic pressure that was noted to dramatically increase and improve in waveform. Procedure concluded and left atrium doubly ligated. Pericardium opposed interruptedly, haemostasis controlled, thoracic drain inserted, Bupivacane intercostal block applied and chest closure done. After operation patients were admitted in the ICU and later to the ward. A short hospital stay was defined when the patient had stayed in the hospital for less than or equal to seven days and prolonged when it was more than that. After discharge home patients were followed at three month then six month intervals for eighteen months and during the follow-up period re-assessment of their general status and echocardiographic parameters were done. The data were entered into an SPSS program 11.5 version and data were analyzed Results Among the 14 patients studied, females accounted for 71.4% as compared to 28.6 males 28.6%. The The ages ranged from 11 to 41 years with a mean of 21.5±8.8 years. The peak was in the 11-20 years age group with a prevalence of 57.1% (Figure 1), and mean duration of symptoms was 58.8± 36.1 months ( range=5-120) with all patients presenting with NYHA class III and IV, each accounting for 50% (Figure 2). Majority of patients were school children (42.9%).The rest included unemployed (28.6%), housewife (21.5%) and employed- primary school teacher (7.1%) Post operative outcomes The ICU stay ranged from 2 to 21 with a mean of 5.7 days (std = 4.8). The hospital stay was between 5 and 16 days with a mean of 9.9 days (std=3.0). Short hospital stay was 50% and prolonged hospital stay was 50%. Post operatively there was a remarkable improvement in symptoms, all patients has NYHA Class I and II (7.1% and 92.9% respectively- Figure 3). Follow-up at 3, 6, 12 and 18 months were 85.7%, 50%, 42.9% and 14.3% respectively. No post-operative mitral regurgitation, re-operation or death in this study. Discussion Rheumatic heart disease still is common in Sub-Saharan African School-age children ranging from 2.7 to 14.3/1000 1,2. In this study student with chronic rheumatic heart disease accounted for 53.7% among which 19.4% has pure Mitral Valve Stenosis. Other studies found a high prevalence of pure mitral valve stenosis of 37.3% among all patients with chronic rheumatic heart disease1,2,3 Complications of chronic mitral stenosis include pulmonary edema, hypotension, thromboembolism, and right heart failure. Medical treatment for symptomatic mitral valve stenosis include a combination of diuretics and b-blockers but, if no response or congestive cardiac failure then intravenous diuretics, inotropic and Amiodarone or Direct Current cardioversion for Atrial Fibrillation3, 8. Palliative Surgical treatments for severe mitral valve stenosis include Balloon Valvoplasty, Open Valvotomy and Closed Valvotomy depending on local experience3. Definitive treatment is mitral valve replacement, either by Biological or Mechanical prostheses. Biological Prosthesis is not recommended in young age as it undergoes degeneration fast due to ongoing rheumatic activities. Mechanical prosthesis will require life-long anticoagulation with Warfarin and therefore close monitoring for International Normalizing Ratio (INR) is required9. Palliative Surgical treatment has been recommended in developing countries as a simple, economical and safe procedure with a good outcome as this does not require anticoagulation4,5,8,10,11. All patients with severe mitral stenosis presented with New York Heart Association (NYHA) class III/IV1. Similar findings were obtained in our study. Our study revealed a significant mean dilatation of mitral valve area from 0.69 ±0.17 cm2 to 1.75± 0.48cm2 p=0.000, NYHA improved significantly from class III/IV to II, p=0.000 (Figure 2, Figure 3 and Table 1). Clinically, it has been found that dilatation of mitral orifice (valvotomy) of ≥ 1.5cm2 has a remarkable improvement in the outcomes in terms of clinical and haemodynamic status4,11. Our study revealed a significant improvement of mean LA size from 5.9cm (std=0.8) to 4.2cm (std=0.6) p=0.000, mean PG from 29.9 mmHg (std=10.72) to 15.70 mmHg (std=7.8) p=0.002, mean EF from 53.9% (Std= 7.5) to 68.3% (std=5.6) p=0.000 and mean PHT from 64.07 mmHg (std=28.71) to 32.36mmHg 9std=13.59) p=0.000 (Table 1).Similar findings of Closed Valvotomy has been found in terms of size of the left atrium-LA, peak pressure gradient across the mitral stenosis-PG, ejection fraction-EF and pulmonary hypertension-PHT7,9. Complications following valvotomy include mild to severe mitral valve regurgitation, mitral valve rupture, chordal rupture, and re-stenosis. A study done in India by John et al8 on 3,724 patients of closed mitral valvotomy found mild mitral valve regurgitation = 18%, severe mitral valve regurgitation = 0.3%, re-do for re-stenosis = 6.7%, hospital mortality =3.8%, late death = 4.2%. Similar studies by Suri et al10 and Tutun et al12 on closed mitral valvotomy found that the mean interval between the first and second valvotomy ranged from 9.4 years to 12 years, hospital mortality ranged from 0.4% to 2.8%, trivial mitral valve regurgitation was 16.1% and moderate to severe mitral valve regurgitation ranged from 0.2% to 7.7%. Survival rate following valvotomy between 6 years to 30 years ranged from 94.0% to 49.1% 5,13 with re-stenosis rate of 4.2-11.2% per 1000 patients/year between 5 – 15 years5. Several studies compared early and late outcomes between closed mitral valvotomy and Balloon Mitral Valvotomy and found no statistical significant difference7,13,14,15. Our study revealed a favorable ICU and Hospital stay with no major complication or death though a short term results. Follow-up decline with time progressively as most of the patients resumed school and others were back to their district level since they had no complication. Conclusion There was an overall highly significant improvement in clinical stage of the disease, reduction in mean pressure gradient across the mitral valve, reduction in pulmonary hypertension and mean left atrial size. Similarly there was improvement in ventricular function in terms of ejection fraction and increase in mean mitral valve area. References
Copyright 2011 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js11013t1.jpg] [js11013f3.jpg] [js11013f1.jpg] [js11013f4.jpg] [js11013f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}