 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 16, No. 1, March/April, 2011, pp. 111-118 Risk Factors Related to Hospital Mortality in Kenyan Patients with Traumatic Intracranial Haematomas K.P. Kithikii1, K.J. Githinji2 1Department of Human Anatomy, University of Nairobi, Kenya Correspondence to: Dr Peter K. Kitunguu, E-mail address: pkitunguu@hotmail.com Code Number: js11018 Background: The aim of this study was to investigate the factors
which influence mortality of patients with traumatic intracranial hematomas
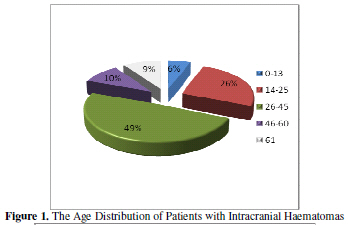
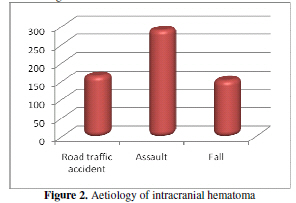
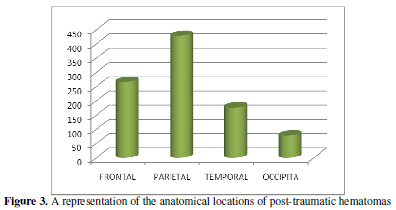
(ICH). Introduction Traumatic intracranial haematomas (ICH) are some of the most common traumatic neurosurgical emergencies which often require surgical intervention. It is estimated that intracranial haematomas occur in 25–45% of severe traumatic brain injuries, 3–12% of moderate cases, and approximately 1 in 500 patients with mild head injury1, 2, 3. Although there have been drastic developments and improvements in neurotraumatology, emergency medical service systems, neuro-intensive monitoring and treatment, ICH is still a disorder with a very high mortality rate and extremely poor prognosis among traumatic brain injuries4, 5, 6. Therefore, identifying reliable prognostic factors for traumatic ICH to improve the surgical results in these patients is important. However relatively few studies have focused on the factors that affect the outcome of patients with surgically treated traumatic ICH. In addition, to the authors’ knowledge there has been no other study that addressed Intracranial Haematomas among Kenyan patients. Kenyatta National Hospital is a national teaching and referral hospital with a bed capacity of 2000 and the largest neurosurgical unit in the Great Lakes region. Through this center, the great majority of neurosurgical referrals are managed. We reviewed records of patients who were diagnosed with traumatic ICH to elucidate which factors are related to mortality of this lethal disorder with a view to improve functional outcome. Patients and Methods Following ethical approval, the records of 608 patients who were admitted to the Kenyatta National Hospital and were diagnosed with traumatic ICH between January 2000 and December 2009 were reviewed. We categorized all variables which might have been related to the functional recovery and mortality into three groups : 1) clinical variables; gender, age, mechanism of injury, preoperative GCS scores, preoperative pupillary abnormalities 2) computerized tomography (CT) variables; location of hematoma, midline shift 3) surgical variables; type of surgery, time elapsed from accident to surgery. The GCS score is usually determined on admission and all patients were divided patients into three groups; those with GCS scores of 3 to 8, 9 to 13 and 13 to 15 for statistical analysis. For logistic regression analysis, patients were classified as having 0, 1, or 2 reactive pupils. Data was collected in pre-formed questionnaires, coded and analysis carried out using Statistical Package for Social Sciences (SPSS) version 11.5. Frequencies and means were computed for description of the various variables, discrete variables compared using the Chi-square test and continuous variables compared using the Students’ t-test. Logistic and univariate linear regression model were run to determine which variables are independently associated with functional recovery and mortality. A p value <0.05 was considered statistically significant. Results During the study period, 608 patients were admitted at Kenyatta National Hospital with a diagnosis of traumatic intracranial haematoma. Five hundred and forty three patients (89.3%) were male and 65 (10.7%) female. The mean age was 35.33 years (+/- 17.420) with a range from 6 months to 96 years. Majority of the patients (49%) were aged between 26 and 45 years while 5.6% and 9.4% were aged below 13 years and older than 61 years respectively. The most common cause of injury was assault (48%) with road traffic and falls accounting for 28% and 24% respectively. A total of 290 patients (47.7%) presented with an extradural haematoma and 259 (42.6%) with a subdural haematoma while 24 (3.9%) patients presented with both haematomas. Other post-traumatic lesions included intracerebral hemorrhage (126; 20.7%), subarachnoid haematomas (21; 3.5%), contusions (49; 8.1) and skull fractures (169; 27.8%). The parietal lobe was the most common location of intracranial hematomas accounting for 68% of the cases while the occipital lobe was the least common with 12.8%. Of the 608 patients in our series, 112 patients died while hospitalized and the overall mortality rate was 18.4%. The mean age of these patients was 38.37 years + 16.518 with a range from 2 to 96 years. Eleven contributory variables to death were analyzed separately in univariate analyses. Consequently, eight factors were found to be significantly related to death (Table 1). A significantly higher mortality rate of 23.3% and 26.3 % was observed amongst patients aged between 46 to 60 years and older than 61 years respectively (p=0.025). It was also observed that the mortality rate increased in direct proportion to an increase in age. With regards to sex, one hundred and six (94.6%) of the patients who passed away during admission were men while 6 (5.4%) were women (p=0.026). In addition, there was a higher mortality for patients with subarachnoid hemorrhage (43%) with the lowest mortality being observed among patients with extradural hematoma (15%). The admission GCS score was highly correlated with hospital mortality (p=0.000). Of the 148 patients with preoperative GCS scores of 8 or less, 83 (59.3%) died. By contrast, only 22 (11%) and 7 (3%) deaths occurred in the patients with scores ranging from 9 to 12 and greater than 13 respectively. Details of the various components of the Glasgow Coma score were available for 492 patients. The mortality rate for patients with a motor score of 6 was 4.8 % as compared to 72.7% amongst patients with a motor score of 1 (p=0.000). In addition, higher vocal and eye responses were associated with statistically significant lower mortality. Details of pupillary reaction to light were documented for 589 patients as follows: 466 patients (79.1%) had symmetrical reactive pupils, 69 (11.7%) had anisocoria but reactive pupils and 54 (9.2%) had homolateral unreactive mydriasis. When pupillary characteristics were cross tabulated with outcome, 70.4% of patients with unreactive pupils died as compared to 7.5% of patients with bilaterally symmetrical reactive pupils (p=0.002). Further, of the 406 patients with a history of loss of consciousness, 24.9% died during admission as compared to 5.4% mortality in patients with no history of loss of consciousness (p=0.000). A history of convulsions was associated with a higher mortality 26.6% as compared to 17.3% of patients who did not have such a history (p=0.157) Table 1. Factors Significantly Related to Death
Regarding the relationship between the haematoma location and mortality, our data showed a higher mortality rate for patients with posterior fossa haematomas (34.04%), although the statistical analysis indicated that the difference was not significant (p=0.072). In addition, there were 447 patients who underwent surgical evacuation of hematomas. There was a statistically significant increase in mortality in patients who did not undergo surgical intervention (26.1%; p=0.000) as compared to those who were operated (15.7%; p=0.00). The mean time elapsing from accident to surgery was 3 days. Patients who were operated on more than 4 days after the initial trauma had a mortality of 42.1% as compared to 9.3% for patients operated on within 24 hours. When the entire study population was subjected to logistic regression analysis, sex, age, pupillary reactivity, admission GCS scores and mechanism of injury were found to be significantly independently predictive of functional recovery. Among these patients, type and timing of operative intervention did not significantly affect outcome. Table 2. Results of logistic regression on factors affecting mortality among patients with intracranial haematomas
*Table 2 Variables are listed in order they entered forward stepwise selection process. Age was entered as continuous variable; Glasgow coma scale group as 1 (Glasgow coma score 38), 2 (Glasgow coma score 912) and 3 (Glasgow coma score 1315); systolic blood pressure as 1 (<90 mm Hg) and 2 (>90 mm Hg); †Factor by which odds change when independent variable increases by one unit; values <0 indicate that odds increase as explanatory variable increases and values >0 indicate that odds decrease as explanatory variable increases. Discussion In spite of more rapid diagnosis and aggressive neurosurgical intervention, the mortality rate of traumatic intracranial hematomas is still high in majority of series ranging between 39% 7, 8 and 75% 6, 9. In our series, the observed overall mortality was 18.4%. Although this figure may appear low, it must be interpreted in consideration of the admission GCS. Majority of the patients in this series 435 (74.6%) had an admission GCS above 9 and only 148 (25.4%) had severe head injury. Mwang’ombe and Kiboi10 reported an overall mortality of 56.2% amongst patients with severe head injury in a Kenyan population which is in accord with our observed 59.3% mortality of those patients in this series with severe head injury. It has been established in literature that increasing age is associated with a higher mortality from traumatic brain injury. Howard et al 11 compared 33 young patients (aged 18-40 years) with old patients (aged over 65) and they reported significantly higher mortality rate in the older group (74% versus 18%). Mosenthal et al 12 observed that the mortality from isolated traumatic brain injury for the geriatric population was twice that of younger patients. Munro et al 13 also found that patients aged 65 years and older had lower survival rates than patients less than 65 years old. Similar findings have been reported by other authors5, 14, 15. In the study by Wilberger et al 16, 17, the mean age of survivors was 41 years and of non survivors was 59 years. We observed a similar trend and found that age was an independent predictor of outcome in traumatic ICH. In our study, those patients aged younger than 13 years had a mortality rate of 5.9%, whereas patients above 61 years had a mortality rate of 26.3%. In addition, those patients older than 45 years showed significantly higher rate (OR=-0.12, p=0.035) of mortality by multivariate logistic regression analysis. The mechanism by which age has such an effect on outcome is unknown, but suggestions include a poor regenerative capacity of the older brain and predisposition to develop a more lethal injury11. Some of this increased mortality in the elderly may be explained by the intrinsic properties of the ageing brain, pre-existing co-morbidities and complications. Furthermore, the adverse effects of general anaesthesia and surgery may affect the respiratory and circulatory function of the elderly, increasing the severity of brain injury. Therefore, in addition to treating pre-existing diseases to decrease the risk of complications, improved long-term care should be emphasized for elderly surgical patients. The preoperative GCS score was another important predictor of outcome. Many authors reported that there is highly significant correlation between outcome and GCS score at admission14, 18, 19, 20. Of the 148 patients with preoperative GCS scores of 8 or less, 83 (59.3%) died. By contrast, only 22 (11%) and 7 (3%) deaths occurred in the patients with scores ranging from 9 to 12 and greater than 13 respectively. These findings confirm recent studies indicating that the severity of injury determines the outcome21. Further, Mwang’ombe and Kiboi10 also found that outcome in head injury patients was directly related to admission GCS. Pupillary abnormalities are associated with a significantly worse outcome. In our series, patients who had bilateral areactive pupils had a mortality of 70.4% as compared to 55.1% and 7.5% for one reactive pupil and bilaterally symmetrical pupils respectively. Many authors reported that patients with bilateral fixed pupils at surgery had a mortality rate from 64 to 93% 4, 5, 6, 16, 22. Kyu-Hong et al 21 reported that patients with one non-reacting pupil, had a mortality from 48 to 68%. This is in accordance with the findings of our series and is confirmed by other reports 18, 19, 23. In addition on logistic regression, pupillary abnormalities were strong predictors for mortality of patients with traumatic intracranial hematomas (OR= -1.179, p= 0.000). It has been postulated that pupillary dilatation is associated with decreased brainstem blood flow and that ishaemia rather than mechanical compression of the third cranial nerve is an important causal factor24. The time from the trauma until surgical decompression also affects the mortality. Some researchers have observed that the sooner surgery is performed in cases of acute head trauma, the better the final results are 25, 26. Seelig et al 27 in their study concluded that a delay from injury to operation was the factor of greatest therapeutic importance in traumatic ASDH. But the relationship between time to surgery and outcome is still controversial. Haselsberger et al 19 reported that 47% died and 32% had a favorable outcome among the patients operated within two hours after the onset of coma. On the other hand, Stone et al 23 reported no difference in patients operated within 4 hours of injury compared with those operated later. In our series, the mean duration before surgical evaluation was more than most reports but with a low mortality rate. In our study, only 9.3% of the patients undergoing surgery within 24 hours of the injury died, while those operated on over 4 days after injury had a 42.1% mortality rate. However in our series, due to the retrospective nature of the study, we were unable to analyse the length of the period of herniation or duration of operation as independent predictors. Conclusion We suggest that the patients in whom surgery is indicated, especially those with herniation, undergo surgery as soon as possible after trauma. Moreover, a rational surgical approach, effective removal of the haematoma and the avoidance of complications are key factors to reduce the postoperative mortality. References
Copyright 2011 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js11018f1.jpg] [js11018f3.jpg] [js11018f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}