East and Central African Journal of Surgery
Association of Surgeons of East Africa and College of Surgeons of East Central and Southern Africa
ISSN: 1024-297X EISSN: 2073-9990
Vol. 16, Num. 1, 2011, pp. 111-118
Basic Surgical Skills Corner
East and Central African Journal of Surgery, Vol. 16, No. 1, March/April,
2011, pp. 119-120
Basic Surgical Skills Corner
Chest Tube insertion – The
need for safe practices
S.A.
Salati
King Fahad Medical City,
Riyadh, Saudi Arabia. Email : docsajad@gmai.com
Code Number: js11019
Cases are regularly being
reported in literature regarding complications arising out of chest tube
insertion1-4 indicating the need to propagate and educate safe
methods of chest tube insertion. Careless approach by the medical practitioner
can cause morbidities and mortalities and guidelines and recommendations for
safer practice are being published from time to time 5. I would like
to stress the following factors related to chest tube insertion :
Consent: The importance
of informed and documented consent needs to be highlighted.In developing and
underdeveloped world, the consent in its true sense is usually neglected due to economic and educational backwardness
of the masses. The patient irrespective of his social status has the right to
know about his disease and the proposed procedure alongwith the possible
complications and alternatives.
Pre-procedure
preparation: The most important factor is to arrange an operator knowing the
procedure fully. In a published study from western literature where doctors
were asked to indicate where they would insert a chest drain, 45% indicated
they would insert the drain at a wrong site 6. Preoperative
preparation would also involve proper imaging (except in tension pneumothorax)
and to rule out conditions likely to cause complications like coagulopathy.
Site of
insertion: Immediately prior to the procedure the identity of the patient should
be verified and the site and side for
insertion of the chest tube confirmed by reviewing the clinical signs and the
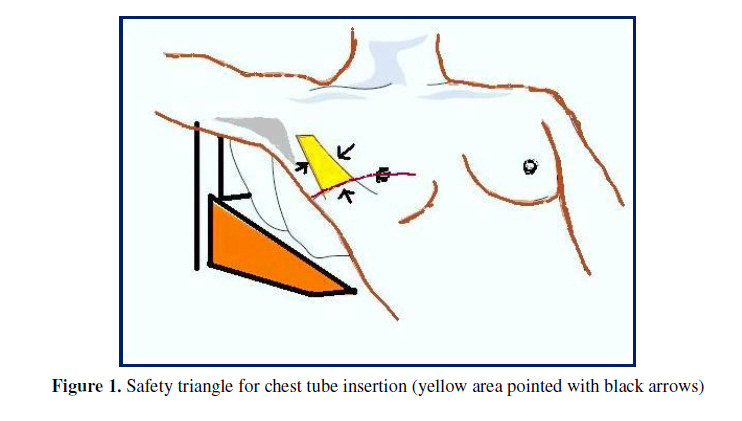
chest radiograph. Proper positioning needs to be ensured .For chest tube
insertion, the concept of Safety Triangle5 (Fig 1) needs to be
taught and it will be really helpful if this figure is hung over the walls of
emergency rooms along with other commonly used figures like Glasgow Coma scale
, Wallace’s rule of 9 etc. This is the triangle bordered by the anterior border
of the latissimus dorsi, the lateral border of the pectoralis major muscle, a
line superior to the horizontal level of the nipple, and an apex below the
axilla. This position minimises risk to underlying structures (eg internal
mammary artery) and avoids damage to muscle and breast tissue resulting in
cosmetically disagreeable scarring.
Aseptic Technique
: Chest tube insertion should take place
in a clean area using full aseptic technique. Empyema is a serious and
avoidable complication , the risk of which is greater with multiple attempts. Although
this is uncommon, estimations of the empyema rate following drain insertions
for trauma are approximately 2.4% 7.
Anesthesia and
analgesia: It needs to be stressed that chest drain insertion has been reported
to be a painful procedure. In one study 8, 50% of patients
experienced pain levels of 9-10 on a scale of 10. Furthermore pains and
discomfort can lead to sudden patient movements during procedure and resultant
complications. This analgesia needs to
be continued till the tube is in place.
Size of the tube: Size of the
chest tube to be used is at best debatable. Studies have shown that the smaller sized tubes are often
as effective as larger bore tubes 9 and are in fact more comfortable and better tolerated by the
patient. In the case of acute hemothorax, however, large bore tubes (28–30 F
minimum) continue to be recommended for their dual role of drainage of the
thoracic cavity and assessment of continuing blood loss 10.
Post procedure
care: The position of the chest tube needs to be verified by imaging. This
proper care needs to be continued as complications can arise which include
pain, malfunction, dislodgement and infection. Furthermore proper technique
needs to be applied for chest tube removal as complications including
pneumothorax and bleeding can occur at this stage when the patient has
recovered from initial cause of tube thoracostomy and these complications can
potentially prolong the misery of the patient. Traditionally, chest radiographs
have been done on all patients immediately after tube removal to detect
complications, but recently studies 11 have questioned the necessity
of such imaging and exposure to radiation. Palesty JA et al 11described
a retrospective review of 73 patients with tube thoracostomy. Out of these 73
patients, only 8 patients' radiology reports changed after the chest tube
removal. Of those, two required chest tube reinsertion (2.7%), but in both
cases the decision was based on clinical assessment rather than on
radiographic findings
References
Chad G. Ball, Jason Lord, Kevin B,et al. Chest tube complications: How well are we training our
residents? Can J Surg. 2007 December; 50(6):
450–458.
Bailey RC. Complications of tube thoracostomy in trauma. J
Accid Emerg Med 2000;17:111-4.
Gilbert TB, McGrath BJ, Soberman M. Chest tubes: indications,
placement, management and complications. J Intensive Care Med 1993;8:73-86
Deneuville M. Morbidity of percutaneous tube thoracostomy in trauma
patients. Eur J Cardiothorac Surg 2002;22:673-8
D Laws, E Neville, J Duffy .BTS guidelines for the insertion of a chest
drain. Thorax 2003;58(Suppl II):ii53–ii59
Griffiths JR, Roberts N. Do junior doctors know where to insert chest
drains safely? Postgrad Med J 2005; 81(957):456-58.
Millikan JS, Moore EE, Steiner E, et al. Complications of tube
thoracostomy for acute trauma. Am J Surg 1980;140:738–41
Luketich JD, Kiss M, Hershey J, et al. Chest tube insertion: a
prospective evaluation of pain management. Clin J Pain 1998; 14(2):152-54.
Clementsen P, Evald T, Grode G,
et al. Treatment of malignant pleural effusion : pleurodesis using a small bore
catheter. A prospective randomized study. Respir Med 1998; 92:593–96.
Parry GW, Morgan
WE, Salama FD. Management of haemothorax. Ann R Coll Surg Engl 1996;78:325–6.
Palesty JA,
McKelvey AA, Dudrick SJ: The efficacy of x-rays after chest tube removal.
American Journal of Surgery 2000; 179(1):13-16.
Copyright 2011 - East and Central African Journal of Surgery
The following images related to this document are available:


{kind=link}