 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 16, No. 1, March/April, 2011, pp. 124-129 Glomus tumours of the Hand in Lagos, Nigeria B.O. Mofikoya1 , C.C. Anunobi2 , G.O. Enweluzo3 1Burns , Plastic
Surgery Hand rehabilitation units, Department of Surgery College of Medicine
University of Lagos , P M B 12003
Surulere, Lagos , Nigeria Correspondence to: Dr. BO Mofikoya, Email: bmofikoya@yahoo.com Code Number: js11021 Background: Glomus
tumours of the hand are uncommon intriguing tumours which cause significant
morbidity. Few reports have documented the epidemiology and presentation in the
West African subregion. The aim of this review is to identify the common
baseline demographics, the presentation, evaluation, diagnosis and treatment
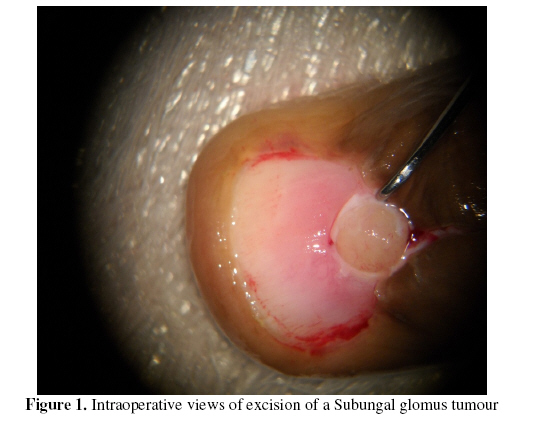
outcome of glomus tumours of the hand in Lagos, Nigeria Introduction Glomus tumours of the hand are said to make up between 1% and 5% of all soft tissues tumours in the hand1. Though first described by Wood in 1812, it was Masson that accurately described the histopathology that has puzzled surgeons for centuries in 19242. Masson recognized that the large polyhedral cells found are similar to those found in the coccygeal gland or glomus coccygeum and named the lesion glomus( latin for ball)1-3 . Glomus bodies are present in the statum reticularis of the dermis and occur all over the body. They are particularly concentrated around the tips of the digits and in the subungal region 4. The typical presentation of glomus tumour in the hand is that of pain which develops from contraction of the glomus cells, can be excruciating paroxysmal and aggravated by changes in environmental temperature particularly cold5 . On account of very few reports concerning this condition in our subregion we present a 10 year review of 11 operated cases at Hand rehabilitation clinic of the Lagos university teaching Hospital as well as a clinicopathologic review of literature. Patients and Methods We reviewed the records of all patients who had surgery for histopathologically confirmed glomus tumours of the hand at the Hand rehabilitation unit of the Lagos university Teaching hospital from July1st 2000 to 30th of June 2010. The case records were studied for age, sex, duration of symptoms, location of the lesion, type of treatment, final histopathologic diagnosis and early results. All patients had their diagnosis made clinically and surgery was done under digital block or intravenous regional (Biers ) block in a bloodless field under an operating microscope .Lesions over the volar digits were directly excised via an incision over the most tender spot. The subungal lesion were excised following an initial nail plate removal, matrix splitting careful tumour excision with the tip of size 15 scapel blade and a careful closure of the nail matrix with 6/0 vicryl and replacement of the nail matrix (Figure 1) . Surgery was done on outpatient basis in all cases. All patients were followed up for a minimum period of 6 months. Results Table 1. Characteristic Features of Patient
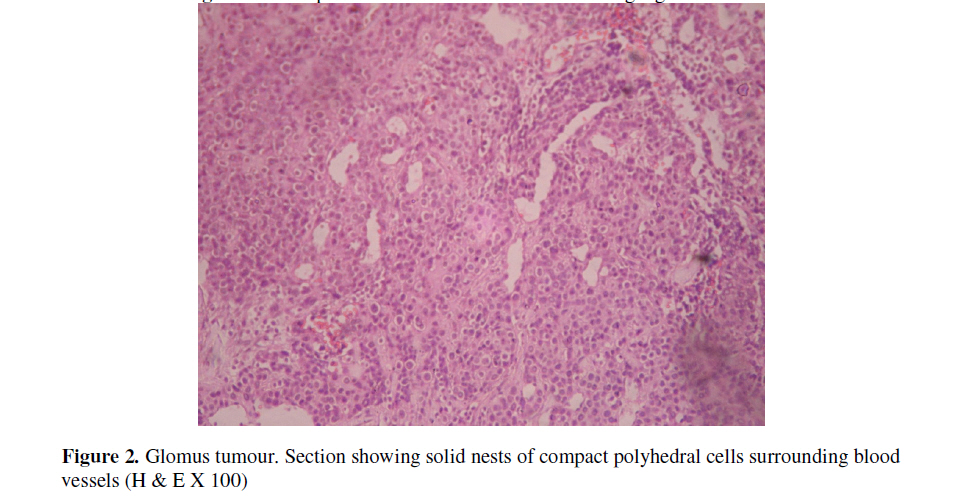
Eleven patients were studied over the stated period. All nine females and two males presented with marked unexplained pain over the various parts of the digits. The mean age of the patients studied was 41years. Six patients presented with lesions at the tip of the digits of which 3 were around the nail and one subungal. Four patients had pain along the lateral surface of the digits and one patient had painful lesion along the ulnar border of the little finger. Duration of symptoms ranged from 3 to 40 months. None of the patients seen had a correct diagnosis prior to presentation. There was no overt swelling in all but one patient. Four patients admitted to cold intolerance .All patients demonstrated a positive Love’s test. Hildreth’s test was not elicited in any of the patients. Only one patient demonstrated a lytic erosion of the distal phalanx . All patients were seen for up 6 months and were all symptom free . Longer follow ups were impossible on account of default. Discussion Glomus tumor- is an uncommon vascular tumour which is said to occur at any age , at any anatomical site but with a predilection for the subungal region. Over a third of these tumours occur- in the hands6,7. Aetiology and pathogenesis The normal glomus body is a contractile neuromyoarterial receptor that controls blood pressure and temperature by regulating flow in the cutaneous microvasculature8. Anatomically the glomus bodies are made up of an afferent arteriole, a vascular anastomosis ( the Sucquet-Hoyer canal), a collecting vein, an intraglomerular reticulum, (containing glomus cells, nerve fibres and interstitial cells) and a capsule9. The glomus cells are specialized smooth muscle cells derived from Zimmerman pericytes and they are concentrated around the dilated vascular space. Changes in temperature lead to contraction of myofilaments in the glomus cells resulting in an increase in intracapsular pressure that is transmitted by the unmyelinated nerve fibres leading to the perception of pain10. Glomus bodies are highly concentrated in the tips of digits, especially under the nail. So, the tumors are usually in the subungual area11. Nearly 75% of glomus tumors are localized in the hands, particularly in the nail apparatus12. Occasionally glomus tumours can occur in extracutaneous sites such as the gastrointestinal tract, bone, genitourinary system and respiratory tract.13 Although the cause of glomus tumour is unknown some authors have proposed that a weakness in the structure of the glomus body may lead to reactive hyperplasia following trauma or that they represent hamartomas in which the components are hypertrophied9. Classification Glomus tumors can be divided into 2 variants: solitary and multiple. Solitary glomus tumors are more common, usually occur in adults, and are predominantly found in the extremities, particularly the nail bed10,14. Multiple glomus tumors, also known as glomangiomas or glomovenous malformations due to their angiomatous appearance, account for less than 10% of all cases. Unlike the solitary forms of the tumor, these appear in younger patients and usually exhibit autosomal dominant inheritance with variable expression. Unlike the solitary forms, multiple glomus tumors tend not to be painful15. Histology Grossly isolated glomus tumors present as a small painful bluish nodule. The cut surface of the tumor could be firm and solid or cystic, and gray or grayish-red or grayish-white, or dark brown in color.16 Microscopically, the tumour is constituted by an afferent arteriole and vascular channels lined by normal endothelial cells and surrounded by a solid proliferation of round or cuboidal cells (figure 2)17,18. The glomus tumour cells are usually uniformly monotonous with oval to round hyperchromatic nuclei homogenous chromatin and scant eosinophilic cytoplasm19. The glomus tumours are made up of three components: glomus cells, vascular structures and smooth muscle cells. According to the World Health Organization (WHO) Classification of Tumors of Soft Tissue and Bone (2002)20, glomus tumour can be further divided into “solid glomus tumor”, “glomangioma”, and “glomangiomyoma” depending on the relative prominence of glomus cells, vascular structure and smooth muscle. The solid glomus tumours are made up of few vascular structures and few if any smooth muscle cells while the glomangiomas which are less well circumscribed contain prominent large vascular channels. The glomangiomas are variants that show a predominance of vascular structures and smooth muscle cells. No nuclear pleomorphism or mitotic activity is in glomus tumours generally. The tumours are usually well circumscribed but unencapsulated, and the background stroma may be fibrous or myxoid.21. Immunohistochemically they manifest reactivity for myosin, vimentin, actin and basal lamina components but not for desmin19,21. Endothelial markers are absent in the tumour cells21 According to the WHO Classification of Tumors of Soft Tissue and Bone20, “glomus tumor” should be defined as a malignant tumor when its size is > 2 cm and located at subfascia or viscera, with atypical mitotic figures or marked nuclear atypia and mitotic activity. However whether these tumours are truly aggressive biologically is a debatable point22 Our finding of eleven cases over 10 years in one major urban tertiary care center may reflect the uncommon nature of this tumor as this is comparable to the many reports23,24. Most studies24,25 show a clear female predominance of this lesion as documented in our findings of male : female ratio of 1:5 .Some workers have suggested that hand subungal tumours are commoner in females while extradigital tumours show a male preponderance 6,26. Our mean age incidence was 41 years generally reflecting our young adult population .Even though the duration of symptoms ranged from 3 to 40 months, the universal absence of a correct diagnosis prior to presentation demonstrates the low awareness of this condition among our health workers. This is similar to other reports3,26, Exquisite tenderness on localized pin head compression (Love’test) was positive in all patients seen by us .Our findings were same with that of Bhaskaranand and Navadgi27 i.e this test is 100% sensitive and specific for glomus tumor of the hand .Though high resolution MRI has been shown to clearly delineate the lesion, with tumor showing high signal intensity on T2 weighted spin MR images and strong enhancement after Gadolinium injection4. This modality is not cost effective for many of our patients as the cost of surgery is about 10% to 20% the cost of MRI. We tend to agree with Dahlin5 that exploration of a clinically painful fingertip is justifiable based on clinical suspicion of a glomus tumour. Our operative approach was direct incision over the most tender point and complete en bloc excision of the tumour under digital block. Transungal incision has been the approach for many decades, recently there have been approaches aimed at minimizing trauma to the nail bed .using the lateral approach11,17 , some have advocated the volar approach28 .Few centers use general anaesthesia because of the possible need to harvest a nail bed graft from the toe nail . We believe our 6 month follow up period is too short to be able make useful deductions from. However recurrence rates of between 1and 18 % have been reported in literature 23. Lesion reccurring within months of surgery is generally due to inadequate excision while that occurring more than 2 years after surgery is regarded as a true recurrence. Conclusion In conclusion Glomus tumours of the hand are uncommon tumors arising from glomus bodies which are numerous around the finger tips. Typically made up of glomus cells , vascular structures and smooth muscle cells ,they commonly present as pain and hypersensitivity in the digits. They can be a considerable source of morbidity when diagnosis is delayed. Surgical excision is usually curative. References
Copyright 2011 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js11021f2.jpg] [js11021f1.jpg] |
| |||||||||

{kind=link}
{kind=link}