 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 16, No. 2, July/August, 2011, pp. 7-19 Blood Transfusion in Surgery in Africa P. Jani, A. Howard Correspondence to: Prof Pankaj Jani, University of Nairobi, Email: janipg@wananchi.com Code Number: js11024 Many changes have occurred in transfusion practices in Africa and in Western countries since this topic was first reviewed in 2005. Blood transfusion remains a key component in the resuscitation of surgical patients suffering, whether from operative losses, trauma, GI bleeding, or obstetrics. Nothing has replaced the lifesaving potential of appropriate transfusion. Increased clinical evidence surrounding appropriateness of transfusion, increased understanding of the risks of transfusion, and better ways of managing these risks have been active topics of discussion in the literature since 2005 and will be addressed in this review. Epidemiology of Transfusions and Need for Blood The World Health Organization reports large differences in the amount of blood collected and transfused worldwide. Annual rates of using blood are 45.4 units per 1000 population in high income countries, 10.1 units per 1000 population in middle income countries, and 3.6 units per 1000 people in low income countries. In high income countries 97% of the blood is processed and used as separate components (ie. Red cells, platelets, fresh frozen plasma or cryoprecipitate) whereas in low income countries only 28% of donated blood is used as component therapy, whole blood transfusion is the norm. Component therapy requires more expensive infrastructure and systems than whole blood therapy, but it makes more efficient use of a valuable resource - donated blood - by allowing a single unit to address specific needs of multiple patients. This efficiency pertains more to medical indications than to surgical indications, medical patients may have a specific anemia, thrombocytopenia, or lack of clotting factors whereas surgical patients are typically acutely losing large volumes of whole blood. The greater the blood loss the more necessary it is to restore all components (red cells, platelets, and plasma) in order to prevent coagulopathy and ongoing bleeding, leading to military protocols suggesting 1:1:1 transfusions or even fresh warm whole blood therapy in acute trauma. Blood transfusion in Africa will move towards blood component therapy as time passes, but from the perspective of blood for surgical use a larger and safer supply is probably the more pressing concern. Ten times less blood is available in Africa. Most African blood transfusions are used for medical indications, particularly to support children with Malaria. Africans suffer hugely greater burdens of trauma and obstetrical morbidity than do citizens of Western countries. These facts together mean that there is a huge, and largely unmeasured potential for improving outcomes in Africa by increasing the availability and appropriate use of blood for surgical transfusion. In the face of blood scarcity, the surgeon must know what to transfuse to whom and when. Needed transfusion saves lives. Unneeded transfusion puts a patient at risk of disease transmission and other complications, and denies another patient the benefit of a lifesaving resource. Surgeons need to understand blood transfusion in both its clinical and organizational aspects to fulfill their roles. Evidence Based Surgery and Blood Transfusion Millions of units of blood are transfused each year, providing ample numbers of patients in whom to study important clinical questions. Many randomized trials have been done regarding indications for transfusion, an early and influential one being the Canadian TRICC (Transfusion Requirements in Critical Care) study. The most useful output of the evidence based medicine movement, for the clinician, is a credible guideline which combines the best evidence from the literature in an unbiased and transparent manner. Many practice guidelines now exist regarding blood transfusion and where possible these will be referenced and form the basis of this review. A word of caution is necessary regarding practice guidelines. Look for guidelines from credible professional organizations which represent the interests of doctors and patients, and which have been created in a manner that:
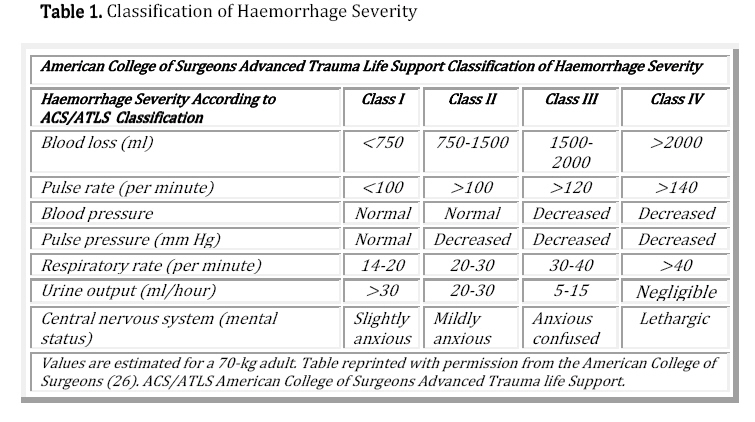
Avoid 'Guidelines' which present biased commercially driven results in the 'evidence based' language that doctors are being taught to look for. Expensive new drugs are often the subject of commercially sponsored trials and ensuing 'guidelines' which are not likely to be as unbiased and trustworthy as a guideline from a professional organization. The astute reader will notice that despite the availability of reviews and guidelines, there is no 'cookbook' to follow and, particularly in surgery, the evaluation of the need for transfusion can only be made by a complete consideration of the clinical status of the patient. Indications for Blood Transfusion in Surgery For about five decades it was commonly taught, practiced, and repeated that a patient needed a transfusion if the hemoglobin was below 10 grams per deciliter. This is not true, and it surprises younger surgeons to hear how unquestioningly this belief was held. The first randomized trial to seriously discredit this belief was the Canadian led TRICC (Transfusion Requirements in Critical Care) trial which showed that a 'restrictive' transfusion trigger of 7g/dL resulted in equally good outcomes as a 'liberal' transfusion trigger of 10g/dL among patients in intensive care units1. Patients who were less sick actually did better with the lower transfusion regimen. A review of ten randomized controlled trials of transfusion triggers2 showed that a restrictive approach to transfusion resulted in 42% fewer patients receiving transfusions, an average of .93 of a unit less blood per patient transfused, and no increase in mortality, morbidity, or length of stay - concluding that restrictive transfusion 'triggers' should be used. Red cells are important for oxygen delivery, as we all know, but the guidelines for massive blood loss issued by the British Committee for Standards in Haematology also point out the importance of red cells to hemostasis3. Blood with too little cellular material in it will not clot - but here the optimum is not actually known - and this is one reason that for a patient actively bleeding or at risk of a re-bleed, aiming for 9 rather than 7 may be appropriate. A recent Cochrane review on transfusion triggers reported:” Seventeen trials involving a total of 3746 patients were identified. Restrictive transfusion strategies reduced the risk of receiving a red blood cell (RBC) transfusion by a relative 37% (RR=0.63; 95% CI 0.54 to 0.74). This equates to an average absolute risk reduction (ARR) of 33% (95% CI 21% to 45%). The volume of RBCs transfused was reduced on average by 0.75 units (95% CI 0.20 to 1.30 units). However, heterogeneity between trials was statistically significant (P<0.001; I²≥74%) for these outcomes. Restrictive transfusion strategies did not appear to impact on the rate of adverse events compared to liberal transfusion strategies (i.e. mortality, cardiac events, myocardial infarction, stroke, pneumonia and thromboembolism). Restrictive transfusion strategies were associated with a statistically significant reduction in the rates of infection (RR=0.76; 95% CI 0.60 to 0.97). The use of restrictive transfusion strategies did not reduce hospital or intensive care length of stay”4. The use of restrictive triggers is supported by credible recent guidelines in anaesthesia, trauma, GI bleeding, obstetrics, and sickle disease. Clinical medicine is not that simple, however. The rapidly changing surgical patient presents much more than a haemoglobin to treat so it is worth considering each guideline in order. The Association of Anaesthetists of Great Britain and Ireland published a 2010 guideline entitled “Blood Transfusion and the Anaesthetist: Management of Massive Hemorrhage”5. This guideline addressed the event of blood losses exceeding 1.0 to 1.5 blood volumes. In such circumstances the role of the surgeon is often to stop the bleeding while the anaesthetist keeps the patient alive, but coordinated team care is key. This guideline emphasized the need for a coordinated response to massive blood loss including prompt and preplanned clinical, laboratory, and logistical aspects. They pointed out that only 16% of Emergency Departments in the UK have a policy detailing such a response. Recommendations from the guideline include warmed blood or blood components as the resuscitation fluid of choice, as well as immediate primary (pressure, tourniquet, dressing) and prompt secondary (operating theatre, angiography) measures to stop the bleeding. Administration of blood in cases of massive hemorrhage is guided by the patient's clinical response to blood as a resuscitation fluid, and not by laboratory parameters. Keeping the patient warm, and preventing coagulopathy by administering whole blood or maintaining a 1:1:1 ratio of packed cells to patients to plasma, are also emphasized. In African settings the basic messages of this guideline - ongoing clinical assessment to guide therapy, and preplanned team and institutional response, apply in any clinical setting from small hospital to large. Trauma Two recent practice guidelines have specifically addressed transfusion in trauma, one from the European surgical societies6 and one from the Eastern Association for the Surgery of Trauma (EAST) in the United States7. Both are worth reviewing in their entirety in order to understand all of the clinical questions related to transfusion resuscitation in trauma. Common to the guidelines is an emphasis on the clinical evaluation of shock as an indication for transfusion. Patients in class III or IV shock as a result of traumatic blood loss need blood as a resuscitation fluid. Measuring the hemoglobin or haematocrit during resuscitation takes time and is misleading due to haemoconcentration from shock, or haemodilution from fluids especially if running into the limb from which the sample was taken. Accordingly, the indication for red cell transfusion is persisting shock as evaluated clinically based on pulse, blood pressure, respiratory rate, urine output, and mental status. The ACS ATLS classification of shock (Table 1) is reproduced from the European guideline, for open access. The European guideline explicitly states that the haematocrit is not to be used as an indication of resuscitation level. A normal haematocrit can be drawn from a rapidly bleeding patient in extremis. It is only once the shock state has been treated, and the vital signs are stable, that hemoglobin levels enter into decisions about further transfusions. With a stable patient, the guidelines both prefer conservative transfusion triggers, with the European guideline stating that the target for RBC transfusion is to maintain a haemoglobin of 7 to 9 g/dL and the American guideline stating that a transfusion trigger of 7 is as effective as a transfusion trigger of 10. Clinicians know, of course, that the risk of ongoing bleeding, the patient's ability to tolerate an anemia, and the requirements for further surgery all enter into decisions around these guidelines or triggers. Both trauma guidelines emphasize the importance of surgical control of hemorrhage as soon as practical, and mentions 'damage control laparotomy' as appropriate in cases of massive abdominal bleeding. Both guidelines advocate ongoing management of bleeding and coagulation intraoperatively and with evaluation of tissue oxygenation. Acute Upper Gastrointestinal Bleeding The European guideline supports using a serum lactate or base deficit as a sensitive test for the adequacy of ongoing resuscitation, and suggests maintaining a platelet count above 75 109/L and a PT and PTT below 1.5 by the addition of platelet or plasma transfusions as needed. Warming fluids will help to prevent Coagulopathy related to hypothermia, which can happen to exposed traumatized patients even in warm environments An international consensus guideline was published in the Annals of Internal Medicine in 20108, and evaluated the literature according to quality and evidence standards listed in AGREE and GRADE. This guideline suggested blood transfusion for hemoglobin below 7 g/dL and rated the recommendation as based on a low grade of evidence in this clinical circumstance. The guideline advocated endoscopy for diagnosis and treatment, with clips, electrocoagulation, and sclerosants considered equivalent in effectiveness. Assessing and treating the haemostatic system (platelets and factors) and administering proton pump inhibitors were also supported by evidence, administering H2 receptor antagonists or somatostatin was not supported by evidence8. A Cochrane review recently evaluated the published literature on this common problem, seeking randomized and quasi-randomized controlled trials. There was insufficient evidence of high methodological quality in the literature to make any statements regarding the effect of red cell transfusions on mortality9. This is an example whereby lack of evidence of effectiveness does not equate to evidence of lack of effectiveness. Transfusion saves patients who might bleed to death - identifying them clinically from those who might not is challenging. Studying them in randomized prospective trials with consent is of course even more challenging. This is why professional organizations will issue practice guidelines even in the absence of high level evidence in a systematic review or a meta-analysis. The American College of Obstetricians and Gynaecologists published a guidline on evidence based management of postpartum hemorrhage in 200810. The guideline emphasizes the role of treating uterine atony with drugs or manipulation, removing retained products or placenta, and evaluating and treating coagulopathy. Red cell transfusion may play a role in the resuscitation of mothers in hemorrhagic shock, transfusions of red cells were used in 0.4 to 1.6% of cases of postpartum bleeding in the North American setting. African obstetrical reality is likely considerably different. Patients with sickle disease may have chronic anemia, and therefore may be adapted to and tolerant of lower hemoglobin. A Cochrane review evaluated the evidence surrounding preoperative transfusion for patients with sickle cell anemia undergoing elective surgery. Only two randomized trials were found which met inclusion criteria for the review. The first evaluated an aggressive preoperative transfusion protocol designed to decrease the proportion of HbS, compared to a conservative preoperative transfusion protocol designed only to raise the preoperative total hemoglobin. There was no advantage to the aggressive preoperative protocol, so transfusion to the desired hemoglobin endpoint was suggested. The second trial compared routine preoperative transfusion to standard care with transfusions given only as necessary in response to operative blood loss. No advantage to routine preoperative transfusion was noted. Both trials recorded mortality, complications, and infections none of which were influenced by a more aggressive or routine preoperative transfusion protocol. The conclusion from the Cochrane review and from these trials is that extra-ordinary steps are not needed for patients with sickle disease, but the strength of evidence and recommendations is weak based on the limited number of studies. Hemolytic Transfusion Reaction The most immediate risk of transfusion is acute hemolysis following incompatible blood. Incompatible blood is one of the top three fatal transfusion complications in the US, the others being transfusion related acute lung injury, and sepsis from bacterial contamination11. Most transfusion reactions are from incompatibility of the ABO type, and most reported reactions related to misidentification of either the patient or the bag of blood. The operating room is the most common area in which ABO incompatible blood is administered, likely due to the complexity of the team and the task11. However, it is unacceptable to have our patients die from what are essentially preventable clerical and logistical errors and so it is incumbent on surgeons to play an active part in ensuring blood safety in their institutions. Transfusion Related Acute Lung Injury This is a recently described and still poorly understood clinical syndrome but is the leading cause of transfusion related mortality in the United States. Perhaps one transfusion in 5000, but up to one in 400 for platelet transfusions, is an estimate of the clinical incidence. An acute lung injury, presenting in a similar manner to ARDS, occurs within six hours of the transfusion. Fluid overload must be ruled out in order to make the diagnosis of TRALI. The pathophysiology is felt to be related to white blood cell antibodies in the transfused blood reacting with antigens on the hosts white cells and causing injury in the microcirculation of the lung. The pulmonary infiltrate appears quickly on plain radiographs, and ventilatory support may be required. In distinction to ARDS, the infiltrate typically clears within 96 hours. Case fatality rate is estimated at 5% to 10%11. TRALI probably has the potential to occur in the African setting but may be underdiagnosed. Coagulopathy is not a complication of transfusion per se, but is a common accompaniment. Clotting requires a normothermic patient with adequate platelets and clotting factors, as well as a sufficient circulating red cell volume that the clot can form and stay. Attention to the patients temperature, PT and PTT, platelet count, and clinical signs of coagulopathy such as bleeding from venipuncture sites will allow administration of platelets and clotting factors where needed. Patients transfused with red cell concentrates are more likely to develop clotting problems sooner than those transfused with whole blood, in Africa both systems of blood banking are in place depending on the institution. Transmission of viral agents from donor to recipient is a widely discussed complication of transfusion. It is particularly relevant in Africa because of the high prevalence of HIV disease as well as other transmissible viral infections including hepatitis B and C. As well as a higher population infected with viruses, the some African blood systems use paid donors, which is felt to increase the risk of viral contamination compared with blood systems based on volunteer donors. Donor issues are further discussed below. Finally, testing of blood for viruses, although almost universal in Africa, may not be as complete or accurate. This is particularly true where 'rapid' tests are employed rather than enzyme immunoassays. Jayaraman et al12 published the results of a mathematical model predicting viral transmission by blood transfusion in Africa. They modeled 45 sub Saharan countries and estimated the prevalence of disease, the extent of testing, the accuracy of testing, and the susceptibility of recipients. They reported that “The median overall risks of becoming infected with HIV, HBV, and HCV from a blood transfusion in sub-Saharan Africa were 1, 4.3, and 2.5 infections per 1000 units, respectively. If annual transfusion requirements projected by the WHO were met, transfusions alone would be responsible for 28,595 HBV infections, 16,625 HCV infections, and 6650 HIV infections every year.” These risks are much more substantial than those in high income countries, estimated at one in 1.5 to 4.7 million for HIV, one in 31000 to 205000 for hepatitis B, and one in 2-3 million for hepatitis C. A safer blood system can clearly be established in Africa, and working towards this incrementally will save many lives. A particular problem is the poor performance of rapid tests for viral diseases, compared with enzyme immunoassays which approach 100% accuracy. The rapid test for hepatitis B evaluated by LaPerche et al was only 20% sensitive to contaminated blood13. Storing blood for long enough to allow for enzyme immunoassays, and ensuring that all blood is appropriately tested and tracked, will improve safety compared with relying on rapid tests. Bacterial contamination of stored blood is a significant risk because blood is, of course, an excellent culture medium for many pathogens. One African study tested 434 paediatric blood packs from a Kenyan blood bank and found that 38 of them, or 8.8%, grew bacteria on culture. 64% of the contaminants were gram negative bacteria and were felt to be environmental contaminants resulting from breaks in aseptic procedure in the blood bank14. Transfusion of contaminated blood can cause fulminant and fatal sepsis. Malaria is endemic in many parts of Africa, but donated blood is not screened for the malaria parasite in many countries. A mosquito can transmit malaria by inoculating as few as 15 parasites, whereas a single parasite seen on a blood film corresponds to approximately 10,000 parasites in a 450cc transfusion15. A systematic review found that the prevalence of malaria parasites on microscopy of banked blood varied from a low of 5% to a high of 50% in reports from different places in Africa, with a low outlier of only 1.7% in urban Nairobi13. However, the clinical consequences of transfusing blood with malaria are unclear and poorly studied. Detecting malaria in stored blood by means other than microscopy is difficult. Falade studied 391 consecutive blood donors and found a 20.2% prevalence of malaria by microscopy, higher in the rainy season. They evaluated two types of rapid tests for malaria, the optimal (which measures parasitic LDH) and the Clinotech (which measures a parasite surface protein). Compared with microscopy the optimal test was 16% sensitive and 98% specific, and the clinotech was 69% sensitive and 50% specific. Neither rapid test approached the performance of the time consuming gold standard of microscopy16. Additional work is needed to characterize the risks related to malaria transmission by transfusion, and the best means of testing blood to minimize these risks. It may be that certain populations, such as children without prior exposure, are at greater clinical risk. Autologous Transfusion Programs Autologous transfusion can be used for planned surgery, by having the patient pre-donate their own blood within the month before surgery, and receive that blood as the first unit(s) if transfusion is needed. This approach has little application in trauma. While these programs became popular in North America following public awareness of viral risks of donor transfusion, they are now less popular because of the expense, inefficiency, and limited clinical impact. Current guidelines suggest that the only circumstances where these programs consistently avoid donor blood exposure is in the relatively rare circumstance of planned scoliosis surgery in teens or young adults17. Guidelines for pre-donation suggest that it only be offered if the admission and operating time can be guaranteed, that the use of autologous blood decreases allogenic transfusion but increases the total risk of transfusion (by contributing to preoperative anemia), and that males with hemoglobin form 11 to 14.5 and females with hemoglobin from 13 to 14.5 be considered candidates. Iron supplementation should be given for patients who are iron deficient, prior to the collection of blood and also between collection and surgery. An autologous unit is not a 'safe' transfusion, the major risks of transfusion reaction from mislabeled or misidentified blood, and of bacterial contamination during storage, still exist17. A Cochrane review has found 75 trials comparing intraoperative cell salvage with conventional allogenic transfusion. Cell salvage has been shown to be effective in preventing exposure to allogenic blood in 38% of cases, with no adverse side effects18. The principle areas where this technique applies are elective orthopaedic surgery and cardiac surgery, and that is where the trials have been performed. The methodological quality of the trials has been considered poor because the clinicians involved have not been blinded to the intervention - a common problem with trials of techniques rather than drugs! Tranexamic Acid promotes the clotting cascade and is used to stop bleeding. Its use in trauma has been studied in a large multicenter international randomized trial involving over 20,000 patients. It decreased the risk of death due to bleeding after trauma, from 5.7% in the placebo group to 4.9% in the TXA group19. The reduction in death rates was time dependent, with the greatest benefit if TXA was infused within an hour of injury, lesser benefit if the TXA was infused between one and three hours after injury, and possibly a harmful effect when the drug was given more than three hours after injury20. Use of TXA as an adjunct to transfusion in traumatic shock has been recommended by the British Anaesthesia Society on the basis of this trial5. The use of tranexamic acid in Africa has been examined from an economic point of view. In countries where there is a blood shortage it would be lifesaving, and in countries where there is no blood shortage it would decrease exposure to donor units and the risk of blood borne disease transmission, both with favourable cost profiles21. Aprotinin is another pharmacological agent which promotes clotting, but it does not have randomized controlled trial evidence of effectiveness in surgical bleeding save for in very restricted circumstances related to cardiac surgery. In addition, there is a 1:200 risk of anaphylaxis. Current guidelines recommend not using it in acute surgical bleeding5. Hemophiliacs do not make this factor, which is now available as an expensive recombinant drug. Like all expensive drugs, there is a tremendous push to expand the indications and plenty of money for doing trials. A recent Cochrane review found eleven trials with over 2300 patients without hemophilia were randomized to factor VIIa or placebo to treat bleeding in well designed double blinded trials. There were no trials which showed factor VIIa to have an overall advantage, and it led to an increased risk of thrombotic events. Another fourteen well designed trials looked at prophylactic use among over 1100 patients with similar null results. Null results from randomized trials do provide convincing evidence that this drug is not effective for bleeding patients without hemophilia, and should not be used22. Agents to Increase Blood Production Recombinant human erythropoietin is an expensive drug which has found a place in the treatment of many anaemias associated with chronic diseases and medical causes. Acute blood loss in trauma is different. Robinson et al performed a systematic literature review and found few RCTs studying erythropoietin in trauma, but no evidence of effectiveness at improving patient outcomes or reducing transfusion requirements23. A further study found that when erythropoietin was removed from an institutional guideline, the use of the drug and its associated costs dropped dramatically but the patient outcomes were the same24. Last time this review was written (2005), we stated that active research may lead to red cell substitutes for clinical use, avoiding many of the issues related to allogenic transfusion. This has not changed, and there is still no substance able to replace blood, other than blood. The WHO guidelines (http://www.who.int/bloodsafety/en/) for all countries suggest that allogenic blood be collected only from unpaid volunteer donors, to decrease the risk of disease transmission from donors who are paid or otherwise 'coerced', for example by being related25. The WHO also suggests that blood services be centralized, and that component (rather than whole blood) therapy be used to maximize the availability of a scarce resource. Some African countries follow WHO guidelines, including South Africa, Botswana, Namibia, and Zimbabwe, but overall only 20% of national systems follow all of the WHO guidelines26. In high income countries most national transfusion systems follow this concept, and the risks of viral transmission are very small, estimated at one in 1.5 to 4.7 million for HIV, one in 31000 to 205000 for hepatitis B, and one in 2-3 million for hepatitis C12. Allain has shown that simple social inducements (collecting blood at a radio station and using music and entertainment) can generate and maintain a pool of repeat volunteer donors at little cost, in Ghana27. Replacement donors are commonly used in African blood banking systems, particularly those which are hospital based rather than centralized. When a patient needs a transfusion, the relatives are asked to provide equivalent quantities of blood for the blood bank to ensure ongoing supply. This system has been said to reflect African values of extended family support for the sick, it is also pragmatic, less costly, and easier to administer at a hospital level than looking for volunteers. Most replacement donor blood (>80%) is said to be screened before use25. Allain specifically compared the results of viral screening in 6640 first time volunteer donor units versus 4360 replacement donors in Ghana, and found prevalence of HIV ( 1.03% volunteer, 1.1% replacement donor) and hepatitis B (13.8% volunteer, 14.9% replacement donor) antigens was very similar. This elegant study provides evidence that replacement donors, currently the backbone of many African blood banks, may be more similar to volunteer donors in Africa than the WHO assumes28. There is concern, however, that some 'replacement' donors may in fact be paid individuals with no relationship to the hospital or the patient25. The correct balance between what works in Africa today, and what increases safety in a reasonable manner, will be made based on research and policy making occurring in Africa26. Cord blood can be banked at the time of delivery to provide for the transfusion needs of the specific neonate. While not making an impact on overall blood needs, this is an elegant solution for small volumes for babies and it has been demonstrated as feasible in Africa, with volumes from 40-130 mL preserved29. The safe transfusion of blood is a logistical exercise involving many parts of the hospital. As surgeons, we are among those who need blood the most quickly, and we also work in operating rooms which have the highest rates of errors in blood administration, placing our patients at higher risk. Surgeons should therefore be part of hospital transfusion committees which ensure blood safety for each institution. The safest transfusion is no transfusion so review of appropriate clinical use is an important function of such committees. A review by Tagny provides an excellent guide to the considerations required for a safe blood system - organization and management, selection of donors, elements of testing, whole blood versus component, component preparation, and quality management30. We need a sophisticated local system in each hospital to manage this life saving but potentially dangerous resource.
References
Copyright 2011 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js11024t1.jpg] |
| |||||||||

{kind=link}