 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 16, No. 2, July/August, 2011, pp. 20-24 Postoperative Pain Management: Clinicians' Knowledge and Practices on Assessment and Measurement at Moi Teaching and Referral Hospital. W.P. Kituyi1, K.K. Imbaya1, J.O, Wambani2, T.M. Sisenda3, R.T. Kuremu4 1Lecturer and
Anaesthesiologist, 2Associate Professor and Anaesthesiologist 3Lecturer
and ENT
Surgeon, 4Associate Professor and Paediatric Surgeon Code Number: js11025 Background: Pain is the cardinal symptom
common to diverse disease conditions and it is what drives many patients to
seek treatment. It, therefore, commands a central position in health seeking
behavior. In the post-operative period,
the main concern about pain is not only the suffering it causes, but also
because of its negative effects on the process of recovery. Its management has,
however, remained a major challenge. Numerous myths and insufficient knowledge
of pain assessment, measurement and treatment contribute to the challenges
encountered by health providers in their service to patients. This study was
aimed at determining the knowledge and practices among clinicians who manage
post-surgical pain in a hospital setting at The Moi Teaching and Referral
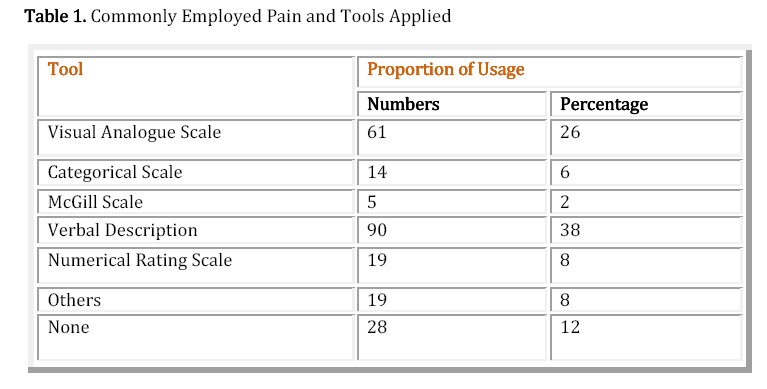
Hospital (MTRH) in Eldoret, Kenya. It was a cross-sectional survey. Introduction Pain is the leading symptom common to illness and is what drives the majority of patients to seek medical treatment for various ailments. Effective management of pain is, therefore, central in meeting the needs of patients. Knowledge of the evaluation and treatment of pain constitute the core elements of managing this complex experience1. Numerous myths, insufficient knowledge coupled with inadequate application of known principles contribute to its poor management. Pain being an inherently subjective experience influenced by multiple factors is difficult to assess and manage. Appropriate assessment tools come in handy particularly in children who cannot vocalize their pain experiences. It requires anticipatory and proactive interventional measures taken accordingly2. Training in the diagnosis and treatment of pain should overcome the major obstacle of inadequacy in the care of this ubiquitous symptom3.This study was designed to determine the knowledge and practices among clinicians who manage post-operative pain at the Moi Teaching and Referral Hospital (MTRH). Subjects and Methods The study was commenced after approval by the Institutional Research Committee (IREC). The post-operative care providers were sampled from surgical and gynecological wards to get a representative sample. Fischer's formula was used where a minimum sample of 200 participants was required. A questionnaire-based cross-sectional study was performed among 236 post-operative care providers who included doctors, nurses and clinical officers at the MTRH, the second National Referral Hospital in Kenya. The study instrument used was a questionnaire designed to collate the demographic data, knowledge and practices of pain assessment and measurement among clinicians. Data were then analyzed using the SSPS statistical software considering a p-value <0.05 as having been significant. Results Of the 236 healthcare professionals who were included in this study, 38 (16%) were doctors, 170 (72%) were nurses and 28 (12%) were clinical officers. On average the duration since they were engaged as healthcare providers was 9.3 years (SD=+ 6.7yrs). Two hundred and twenty seven (96%) confirmed that they routinely managed post-operative pain. A total of 208 (88%) of the respondents, indicated that they had the knowledge to manage post operative pain; however, only 103 (44%) indicated that they had knowledge on how to assess and measure post-operative pain. Among the doctors, 21(55%) indicated that they had sufficient knowledge to recognize and manage post-operative pain while the proportions of nurses and clinical officers were 70 (41%) and 12(43%) respectively. Of the participants 135 (57%) indicated that they had inadequate knowledge regarding the tools that may be employed for pain assessment and measurement. Those who had never had any formal teaching in relation to pain evaluation and management constituted 50 (21%) of all the participants. The duration of service among all the health care providers in the post-operative care units did not influence the respondents' knowledge and confidence in the evaluation and management of pain. (ANOVA (F (1) =0.045, p=0.832). Regarding availability of protocols, 59 % of the health care professionals reported that there were no protocols and guidelines on post-operative pain management at their work stations. The tools which the participants said were commonly employed by participants in the present study are shown in the Table. Discussion Optimal post-operative pain management is guided by its objective assessment and measurement4. There are several validated tools that apply in different patient categories which if implemented appropriately can improve the confidence of the health care workers in assessing pain4,5. The post-operative orders commonly used are mere guidelines and hence may not sufficiently address post-operative pain management for every patient operated on. Those who take care of the patients need to have the knowledge on post- operative pain management which should be applied appropriately in the immediate post-surgical period for the patients to benefit. Despite the majority (81%) of the respondents in our study indicating that they had the knowledge on how to assess and measure pain, most (73%) of them felt they had insufficient knowledge on objective pain evaluation using tools that have been tested and validated for this purpose. A further 21% said they had no knowledge at all on pain assessment tools. The Verbal descriptive scale had an application frequency of 38% while the McGill scale had a dismal 2% application. The use of pain assessment tools was extremely variable among the participating health care providers. Pain assessment tools used by health care providers elsewhere have produced optimal and satisfactory results in acute pain management4,5. From this study, it therefore follows that overall post-operative pain assessment and measurement in our institution is likely to be sub-optimal from the onset after surgery. This scenario is likely to prevail in the region specifically in sub Saharan region due to similarities of the institutions in terms of resources and personnel trained in similar circumstances. The feeling of knowledge deficiency as reported by the participants in our study can lead to lack of confidence and to low self -esteem when faced with patient in pain. This can as a result lead to a poor overall management of post-operative pain. One study showed that knowledge in the use and implementation of pain evaluation tools increased staff confidence in assessing pain in the non-verbal sedated patients from 57% before versus 81% after implementation and increased the number of pain assessments documented by the nursing staff for non-communicative patients in the intensive care unit per day (2.2 before vs. 3.4 after)5,6. Use of protocols and guidelines can greatly improve pain management7. In our study, approximately 59% of the study population said there were no protocols/guidelines on post-operative pain management at their work stations; hence none were employed in the routine patient care. For a referral institution at a tertiary level like MTRH, quality management systems based on evidence - based guidelines and protocols need to be in place and their use monitored for performance improvements for the clinicians to provide better post-operative care even though literature is not conclusive on the matter of availability versus adherence and improved care8,9. Nurses are multi-tasked in our health institutions performing various functions including post-operative pain management and the general nursing care of patients. A finding of concern in the present study is the fact that 41% of them felt that they had the least knowledge regarding pain management compared to 56% of the doctors and 43% of the clinical officers. Of all the clinical cadres, nurses spend more time with patients than the doctors and the clinical officers. Considering the overwhelming workload situation in our institutions, safety and general care for post operative patients is most likely compromised. The present study has highlighted the apparent gross deficiencies in the evaluation, measurement and management of pain among all the cadres of clinicians on self-report. The health care professionals cannot therefore be expected to approach patients in pain with confidence if they feel deficient in pain management. An overwhelming 96% of the respondents in our survey expressed need for training on pain evaluation tools even though some had said they knew how to assess pain. In a closely related study done in Malawi, most doctors indeed recognized that post operative management was important but they were not adequately trained to manage pain using validated tools consequently post operative pain after caesarian section was not optimally handled10. Notably, even a long duration of clinical service did not make experienced health care providers feel sufficiently knowledgeable to assess and measure pain. Other investigators11 were also unable to confirm the influence of expertise on pain management. Deep cultural beliefs by health care providers which have been shown to interfere with approach to pain management12,13 were not investigated in this study but may need to be looked into in follow up survey to establish other barriers to optimal pain management in this region. Conclusion Overall, a significant proportion of the participants indicated an inadequate knowledge regarding the objective evaluation and management of post-operative pain. We, therefore, strongly recommend that institutions endeavor to institute training programmes on the basic principles of wholesome pain management. Furthermore, continuous professional development should be strengthened for health care providers in all our health institutions. Acknowledgement To the administration of Moi Teaching and Referral Hospital for permission to carry out the study. The IREC for approving this study and all the health care professionals who participated in this survey for their time and effort. References
Copyright 2011 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js11025t1.jpg] |
| |||||||||

{kind=link}