 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 16, No. 2, July/August, 2011, pp. 25-31 Should Omphaloceles be Re-classified? J.O. Adeniran, L.O. Abdur-Rahman, A.A. Nasir Pediatric Surgical Unit, University of
Ilorin Teaching Hospital, Ilorin, Kwara State, Nigeria Code Number: js11026 Background: Omphaloceles are
presently classified into 'minor' and 'major' categories depending on the
diameter of the umbilical defect. In developed countries most 'major' cases are
treated with silo, parenteral nutrition and progressive compression. In
developing countries most cases are managed conservatively with honey
dressing. This may take 1-2 months for
proper eschar to form. Even when successful, most patients don't come for
secondary repair. The objective of this review was to re-classify
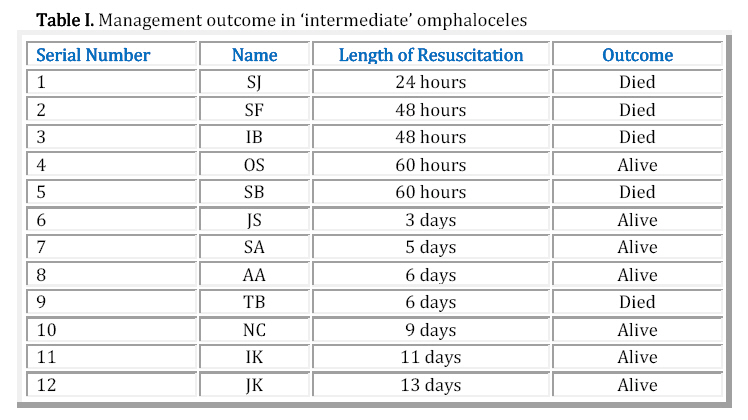
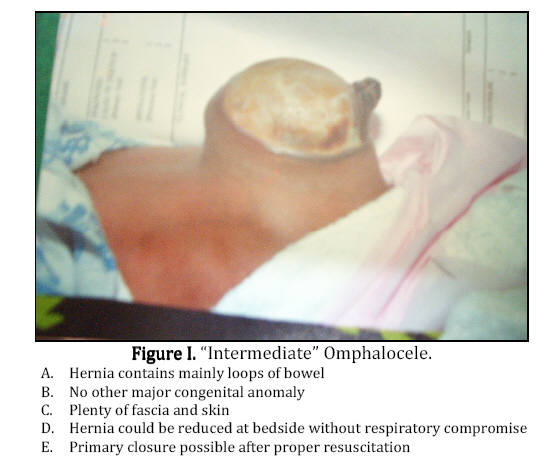
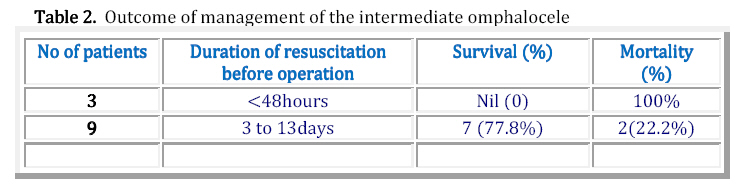
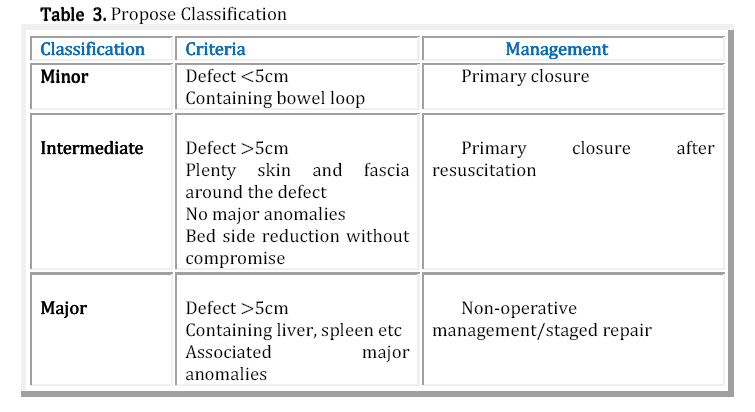
omphaloceles into 'minor', 'intermediate' and 'major' anomalies. Introduction Omphalocele is a congenital midline abdominal wall defect that results in herniation of intraabdominal contents covered by a lining of peritoneum and amnion. The severity of the defect often ranges from a minor herniation of the umbilical cord to a significant protrusion that includes large proportions of intestine and the liver1. Omphalocele are classified into 'minor' if the diameter of the umbilical defect is less than 5cm or 'major' if more. The definitive goal of surgical intervention is to provide complete fascial and skin closure without causing excessive intraabdominal pressure or abdominal wall tension. 'Minor' omphaloceles usually contain a loop of the midgut, the peritoneal cavity is adequate and there are no other major associated congenital anomalies. Most of the defects can be closed primarily. Operative treatment of omphalocele major is usually challenging for pediatric surgeons, which is reflected by the broad range of approaches described in the literature2-6. 'Major' omphaloceles have, in association with herniated gut, the liver, stomach and spleen7. Because the peritoneal cavity is inadequate, many of the cases of 'major' omphaloceles are managed in developed countries with the use of a silastic silo technique with staged closure when primary fascial closure is not feasible3. Early closure is usually facilitated by elective ventilation and parenteral nutrition4,8. Because of limited facilities in developing countries these cases are managed non-operatively by tulle-gras or honey dressing, and antibiotics. If successful, treatment takes 1-2months. In our experience, most patients die of infection or are discharged in frustration, by parents (against medical advice) who needed to look after the rest of the family. However, some children who presented with defects greater than 5cm were closed primarily. The result of that closure forms the basis for this discussion. Patients and Methods All cases of omphaloceles treated between 2002-2007 were retrospectively reviewed. “Minor' cases were resuscitated with fluid and electrolyte supplements and given parenteral antibiotics. The children were then operated when infections were judged to be controlled clinically. The decision to operate on the 'major' omphaloceles was at the instance of the consultant. No guiding criteria were set. Two patients presented with imminent rupture of the sac. Attempts at skin cover were made (Gross method), but unsuccessful. Patients whose diameter of defects were more than 5cm but successfully closed primarily were separated and analyzed. Age at admission, diameter of defect, length of resuscitation and final outcome were analyzed. Results Forty-four patients with anterior abdominal wall defects were seen during the period. There were 37 cases of omphaloceles, 4 bladder exstrophy and 3 gastroschisis. Of the 37 omphaloceles, 12 were 'minor' and 25 'major'. Twelve patients had defects that were managed conservatively. Of those, 3 died of sepsis and/or congenital malformations in the neonatal period; parents of 3 children discharged against medical advice within 2 weeks of admission to look after the rest of the family. None of them was seen in the clinic again. Two patients had attempted skin coverage for impending rupture but died shortly after operation. Four children formed proper eschar after a period of 4-6 weeks, but only one eventually came for secondary closure. Thirteen of the 'major' cases were planned for primary closure. One discharged for financial reasons. After exclusions and selection, the study group consisted of a cohort of 12 patients closed primarily. Size of the defects ranged from 6cm x 4cm to 10cm x 10cm (mean 7.5 cm x 6.3cm). There were 5 boys and 7 girls. There were no other major congenital anomalies detected in them. They all had plenty of skin and fascia around the hernia to encourage primary closure. All the defects could be reduced at the bedside without respiratory embarrassment to the patient. Three of them were operated within 48 hours, but all died. The other 9 were properly resuscitated and operated between 3 and 13 days. Only 2 died (Table 1). At operation the hernia contents were mostly loops of small bowel, which reduced easily into adequate peritoneal cavities. There were enough fascia and skin for complete coverage without tension. Discussion Omphalocele is due to failure of the midgut loop to return to the abdominal cavity, after the physiological herniation about the 4th -6th week of embryonic life causing failure of fusion of the abdominal wall7,9. Omphaloceles are classified to 'minor' or 'major' depending on the contents of the sac and the diameter of the defect10. Most 'minor' cases have diameters less than 5cm and contain mostly loops of small bowel. There are usually no other major congenital anomalies11. The peritoneal cavity is usually adequate and the defects can be closed primarily11. Major Omphaloceles may also contain the large bowel, stomach, liver and spleen7. Fifty-80% may have other congenital anomalies9,11-13. Detailed clinical, sonographic and radiological investigations should be done during postnatal- resuscitation stage to detect these anomalies9. Because the peritoneal cavity is not adequate in major omphaloceles, attempt at primary closure will cause three problems. Firstly, the tight closure will impair diaphragmatic excursion resulting in reduced lung extrinsic compliance and functional residual capacity9. Secondly, blood flow in the inferior vena cava will be impeded causing a decrease in cardiac output and pulmonary blood flow9. Thirdly, blood flow to the bowel, liver and kidneys may be compromised14. For these reasons, the introduction of viscera into the abdomen can lead to severe complications, contraindicating primary closure for major omphaloceles15. There are 2 options for the surgical treatment of major omphaloceles: staged closure and conservative management. Staged closure consists of gradual reduction of the external peritoneal viscera with increasing intra abdominal pressure causing a slow increase of volume of the peritoneal cavity. Many different techniques have been described in the literature to accomplish closure of this defect. Often, temporary applications of prosthetic patches are necessary to accomplish this task, and multiple operations are needed2. operative methods for closure include: closure with the use of silo with13, sequential sac ligation 5, definitive closure with an absorbable mesh16, alloderm graft over fascial defect6, staged reduction with the use of tissue expanders3,17, the use of Gore-Tex silo placement18 , staged visceral reduction and sequential clamp technique19. The staged closure may carry the same risk of primary closure by placing the abdominal contents under pressure20. However, Intragastric pressure , central venous pressure and intravesical pressure may be measured during reduction to prevent excessive intraabdominal pressure21. These procedures carry good prognosis with excellent long-term quality of life12,21,22. Average mortality of about 2.9-20% depends on size of defect, other major anomalies (especially cardiac) and respiratory distress at birth4,8,13,23, . Vacuum-assisted closure (VAC) device, which allows for improved results in these difficult cases have recently been introduced in the initial management of these patients24. This device is considered safe and effective alternative in treating complicated cases of major omphalocele until a more definitive closure method can be used24. Because all these facilities are not readily available in developing countries, patients with major omphaloceles are managed conservatively with honey, alcohol, silver sulfadiazine or sufratulle dressings 11, 25,26. Many of these patients die from infection before proper eschar forms. Many mothers feel frustrated by long periods of hospital admission and discharge against medical advice. Some workers in developing countries have covered the hernias with skin (Gross method) to create a ventral hernia which could be repaired later11,25. The success of this has been limited in our unit. Two patients with impending rupture had skin mobilization to cover the omphalocele. They died a few hours after operation as elective ventilation was not available. In the few cases when conservative treatment was successful, the parents did not bring the children back for secondary repair26. Conservative management for 'major' omphaloceles has therefore produced unsatisfactory outcome. This was also the experience in some other units in developing countries11, 25,26. But there was a set of patients with diameters of defects more than 5cm, had no other major congenital anomalies, had only loops of bowel in the hernia, and had plenty of skin and fascia around the defect (Figure.1). At the bedside, under aseptic conditions, the hernias could be reduced, and kept reduced for as long as possible without respiratory embarrassment to the babies. Those who were resuscitated and operated within 48 hrs died. Most of those who were properly resuscitated for more than 3 days lived (Table 1 and Table 2). We therefore propose that patients with defects more than 5cm should be reclassified. Those with sac containing liver, spleen etc, who also have other major anomalies will be difficult to close primarily and should be called 'major' omphaloceles. In the developing countries, these should be managed conservatively. Babies whose defects are more than 5cm, but the sacs contain mostly loops of bowel, have no other major congenital anomalies, and the hernia can be easily reduced at the bedside should be termed 'intermediate' omphaloceles. These patients, if carefully selected and properly resuscitated can have primary closure with satisfactory results. Conclusion Babies with omphaloceles must be examined thoroughly for other congenital anomalies (Beckwith-Wiedeman, pentalogy of Cantrell etc). Sonographic and radiological investigations should be done to confirm or rule out these anomalies. Patients should then be properly resuscitated with fluid support, protection of the herniated viscera, nasogatric drainage to minimize bowel distention, antibiotics and adequate warmth. Patients with defects < 5cm (minor omphalocele), if fit, can have primary closure. Patients with defects > 5cm who also have other major anomalies (major omphalocele) should have a staged repair or conservative management. Patients with defects >5cm, with plenty of skin and fascia and no major anomalies when properly resuscitated may be closed primarily when attention has been paid to infection, hypothermia, acidosis, hypotension and hypoxia. We propose that these be termed “intermediate” omphaloceles (Table 3). References
Copyright 2011 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js11026t3.jpg] [js11026f1.jpg] [js11026t1.jpg] [js11026t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}