 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 16, No. 2, July/August, 2011, pp. 32-39 Airway Foreign Body Aspirations in Children at Muhimbili National Hospital, Dar es Salaam - Tanzania. Li Xuechang1,2, E. Richard2, H. Swai2 1ENT Department, Weifang People’s Hospital,
Shandong Provinvce, PRC Code Number: js11027 Background: Foreign body inhalation is a life-threatening clinical situation worldwide
especially in those less than 3 years old. The purpose of this report was to
define the clinical characteristics of airway foreign body aspirations (FBAs)
in children and to analyze the reasons for delay in diagnosis so as to improve
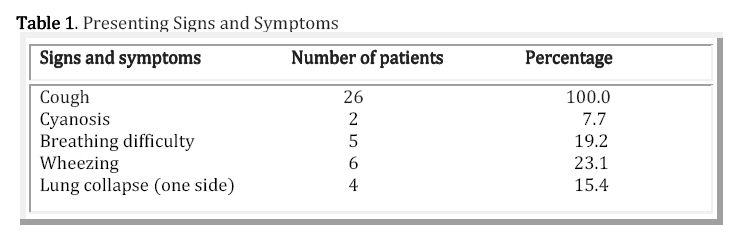
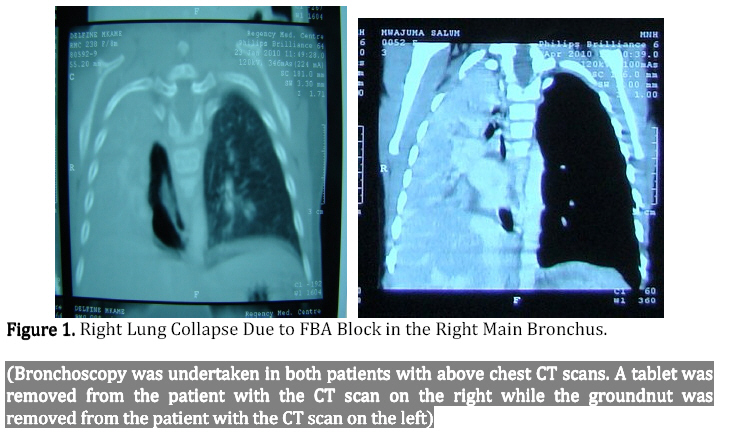
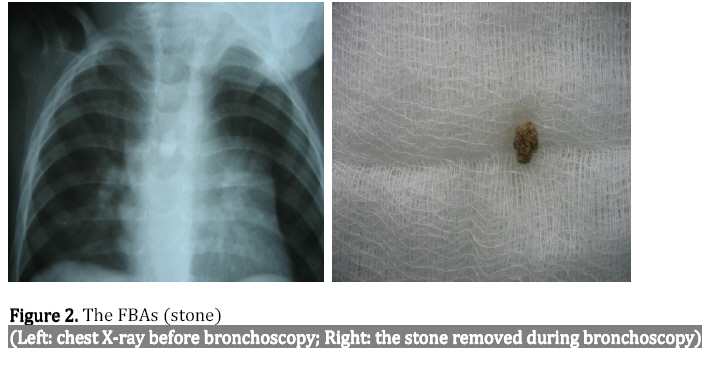
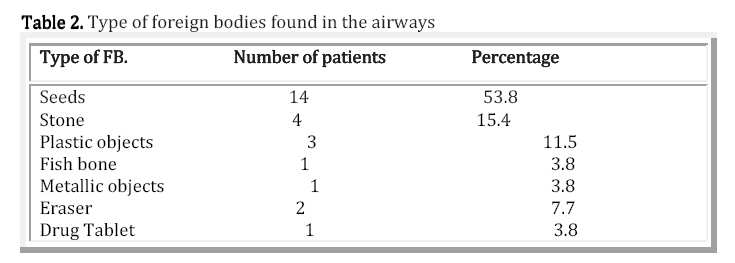
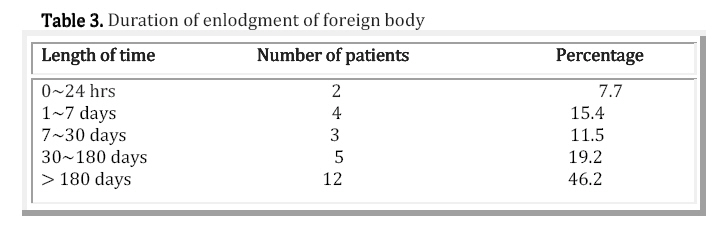
the treatment. Introduction Airway FBAs is one of the most common emergency in ENT department. It occur relatively frequently in young children, especially in those aged under 3 years1, being. Due to delay in diagnosis, a series of chronic pulmonary pathologic conditions may occur in cases without acute respiratory failure. The main clinical features associated with aspiration are cough, difficulty in breathing, wheezing and unresolved pulmonary infection. If these problems are noticed in time, the child will be immediately taken to hospital for further diagnosis and treatment accordingly. In Tanzania, there are no ENT doctors at the district or regional hospitals. The few available ENT doctors are at the tertiary hospitals. Because of a lack of knowledge on the disease presentation by the physician, FBAs are difficult to diagnose in children. If the above signs and symptoms are neglected by the pediatrician, the patient can be misdiagnosed and treated for other diseases such as bronchitis, bronchial asthma, tuberculosis (TB) and pneumonia2. Delayed arrival of a child with a suspected foreign body aspiration (FBA) at the hospital and delayed bronchoscopy were found to be related to a higher rate of complications3. The majority of airway aspirated objects are small things that the child can easily find and put into the mouth. In different countries and regions, the types of foreign body differ. Seeds are the most commonly encountered4,5. These include peanut and sunflower seed. The variation in types of organic materials can be explained by cultural, economical and differences in feeding habits of various regions. FBAs can range widely in the severity of the presentation. The time for removal of inhaled foreign bodies depends on the site of enlodgement. Laryngeal and subglottic foreign bodies need urgent intervention, for example, midnight bronchoscopy or tracheostomy6. Whereas foreign bodies in the main bronchus cause comparatively less airway problems and can wait until the morning for optimal circumstances for manipulation of the paediatric airway7. Rigid bronchoscopy under general anesthesia is the recommended and safest procedure in children with suspected FBAs8. This retrospective study was conducted to investigate the characteristics of FBAs and the morbidity caused by misdiagnosis in Tanzania. Also to spread awareness of FBAs including their prevention and treatment so as to improve the diagnosis and treatment of airway FBAs, with reduction of complications caused by prolonged enlodgement of foreign body. Patients and Methods This retrospective study was conducted at the ENT & Head and Neck surgery department of Muhimbili National Hospital (MNH) from September 2009 to March 2011. Patients with suspected history of airway FBAs that could not be identified on endoscopic examination and those who died before endoscopic procedures were excluded from this study. All patients with a suspected history of airway FBAs underwent bronchoscopy under general anesthesia (GA). All the patients under 2 years should be operated on by skilled ENT specialists because of the narrow airway and in case of respiratory failure. The surgeon chose the appropriate bronchoscope according to the age of the patient and used suitable forceps which could pass through the bronchoscope freely and hold the foreign body firmly. When the foreign body was found to be too big to pass through the glottis or too sharp so as to cause injury to the tracheal mucosa or vocal cords, tracheostomy under GA with the bronchoscope for ventilation was performed and the foreign bodies were removed from the trachea incision. Data was collected using a structured questionnaire. Items included in the questionnaire were: age, sex, the type of foreign body, anatomical lodgement of foreign body, signs and symptoms, misdiagnosis, duration of lodgement before confirmation and treatment by bronchoscopy with or without and FB removal. Data was analyzed using SPSS computer software version 15. Results During the period of study, a total of 26 patients with established foreign bodies in the airway were studied. 16 (61.5%) were males and 10 (38.5%) were females. Boys more easily aspirated foreign bodies than girls. The age distribution showed that children less than 3 yrs accounted for the majority (53.8%), the second highest incidence occurring during school age (42.3%), whose age ranged from 3 to 10 yrs. Rigid endoscopy with forceps under general anesthesia was performed to remove the foreign body. The foreign bodies were successfully removed in 92.3% of cases. We failed to remove the foreign body in 2 patients, both of which can recall a history of inhalation of an eraser. When they came to MNH, the foreign bodies had both been in situ for more than 1 year. The granulation tissue around the foreign body bled easily and this combined with profuse pus frustrated our attempt to remove the foreign body during bronchoscopy. The most common presenting symptom was coughing recorded in 100%. It was the most common symptom immediately after aspiration of a foreign body. Almost all the older patients aged above 5 years could recall a history of severe coughing after inhaling the foreign body. Wheezing recorded in 23.1% was the second most common symptom followed by breathing difficulty in 19.2%. Auscultation of the chest revealed reduced or absent breath sounds on the affected side (Table 1). Lung collapse on chest X-ray occurred in 15.4% of cases (Figure 1). Seeds were the commonest aspirated objects (53.8%) in this study, followed by stone (15.4%) (Figure.2), plastic objects (11.5%), and eraser (7.7%). Seeds and stone were easily found in children aged less than 3 yrs in Tanzania. However plastic objects and erasers were more easily aspirated by primary school students (Table 2). The most common site of foreign body lodgment was the main bronchus in 21 (80.77%) patients, especially the right bronchus. Followed by trachea in 4 (15.38%) patients and glottis in 1 (3.8%). The most dangerous site of foreign body enlodgement was glottis or trachea. The duration of enlodgment of foreign bodies ranged from less than 24 hours to more than 6 months (Table 3). This depends on the knowledge of the first-treating doctor and secondly on the awareness of the parents. According to our study, 23 (88.5%) patients were misdiagnosed one or more times. Two foreign bodies in our series were successfully removed by tracheostomy combined with bronchoscopy. One patient was a 1-year-old girl who aspirated a bean seed into right bronchus, another was a 5-year-old girl who inhaled a metal circle apparatus of a pencil and the foreign body blocked the subglottic region. Both foreign bodies could not be removed from the glottis. Discussion Foreign body aspiration is a life-threatening clinical situation worldwide. This study revealed that children aged three years and below are more commonly affected, which was consistent with other studies1,2. The reason why the younger children are vulnerable to airway FBA is because they like to put objects inappropriate for their age (small objects) into their mouth and when they are teased to cry or laugh, aspiration can occur. They cannot chew food well due to lack of grinding teeth. Poor cough reflex and hyperactivity also make it easier for young children to inhale foreign bodies1. The most common aspirated foreign body in our study was seed, followed by stones and plastic objects. This does not correlate with other studies1,10,11 which found that stones contributed the second most common foreign body. This may be partly due to the environmental and economic situation of Tanzania. Stones are the most available objects which rural children can find and put it into their mouth in Tanzania. Stationery objects like plastics and erasers are the foreign bodies most likely to be aspirated by school-going children. In this study we removed fragments of a tablet from one child with severe breathing difficulty who was suspected to have asthma or TB. The study showed that cough is the most common symptom in patients with FBA, followed by wheezing and breathing difficulty. Usually when the foreign body enters the airway, there must be a severe, dry, irritating cough and sometimes choking will occur due to the protective reflex of the airway. Following this there is a quiet period: the signs and symptoms may disappear or become minor. If still not treated correctly, the third period of irritation or inflammation appears: recurrent cough and symptoms of atelectasis or pulmonary emphysema. If the foreign body remains inside, some complications may occur. According to Chik5, 100% of FBA patients had the persisting cough, which was in agreement with findings in this study. Stridor is an audible sound caused by abnormal air passage during breathing. When ENT surgeons or pediatricians are faced with a child or infant with noisy breathing, they should determine the severity of respiratory compromise and the need for immediate intervention to prevent respiratory failure. Secondly, judgment should be made based upon detailed history and clinical examination whether a significant lesion (FBA) is suspected or not and the need for bronchoscopy. Thirdly, they should understand the consequences and management strategies of the underlying lesion and collaborate with other doctors from related disciplines for follow-up and subsequent management of the patient12. The most common site of foreign body enlodgment was the main bronchus, especially the right bronchus. The second site was the trachea. We also found a fish bone enlodged at the glottis in one male pediatric patient. However, the most dangerous site of foreign body enlodgement is the glottis and trachea. Almost all literature reviewed found that the right main bronchus was the most common site of impaction of inhaled foreign body. Foreign bodies in the trachea and laryngeal inlet are rare13. There are no clinical clues that can determine or rule out the diagnosis before entering the operating room for bronchoscopy. Bronchoscopy is the gold standard for diagnosis of FBA. The diagnosis of FBA is difficult and easily misdiagnosed. Many studies concentrated on this area; Shlizerman3 found that an adult witness of an aspiration episode (most frequent presenting symptom), a child under 2 years and an abnormal plain chest radiography are significant predictors of foreign body aspiration. If we manage each suspected patient carefully, we can find some important clues as to the diagnosis of FBA. In another study Asif14 found that the most consistent finding was decreased air entry on chest auscultation on the side of impacted foreign body which was present in 91.1% of patients. The second most consistent finding was audible wheeze on the side of impacted foreign body found in 53.2% patients. The most common finding on chest X-ray was emphysema found in 61.3% patients, followed by atelactasis in 28% of patients, while 9.7% of patients had normal chest x-rays. We can also find foreign bodies directly on chest X-ray as exemplified in Figure 2, if the foreign body is opaque or translucent. Some authors pay attention to the value of the clinical triad of cough, respiratory distress and stridor, or virtual bronchoscopy and three dimensional CT scans15-18. Most FBA patients in developing countries such as Tanzania, especially those from rural villages, cannot afford to pay for CT scans. We thought that the criteria for diagnosis of FBA should be:
These are practical and decisive factors for suspected FBA patients. According to our findings, 88.5% of patients were misdiagnosed once or more times and 76.9% of patients were correctly diagnosed 1 week after onset of symptoms. In a developed district of HongKong, only 41% of cases were correctly diagnosed one week after onset of symptoms5. The complications secondary to delay in diagnosis in our patients mainly manifested as tracheobronchitis, pneumonia, and granulation tissue formation in the tracheobronchus. After using antibiotics combined with steroids, all the foreign body-removal patients were discharged with improving symptoms. Organic foreign bodies and longer lodgment in the airway need longer antibiotics and steroids consumption. Although some authors insist fibreoptic bronchoscopy is the first choice of procedures to remove the foreign body19,20, we still believe that rigid bronchoscopy under general anesthesia is a safe and practical procedure for Tanzanian ENT surgeons. We are agreement with Singh et al6 that the indications for tracheostomy should include subglottic foreign bodies of long duration, sharp subglottic foreign bodies and foreign bodies that were larger than the glottic chink. The role of tracheostomy in airway foreign body removal is to avoid trauma to the vocal cords and make the retrieval of foreign bodies possible. Sometimes the large foreign bodies lodged at the entrance of the bronchus will be blocked by the vocal cords while passing through the glottis and drop into the trachea causing sudden upper airway obstruction. Facing this situation, we should push the foreign body to the bronchus immediately for ventilation. However prevention is always better than cure. Public awareness through mass media such as TV and newspapers can attract more attention of civil people to prevent FBA. This requires co-operation between ENT surgeons, public officials and reporters. References
Copyright 2011 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js11027f1.jpg] [js11027t2.jpg] [js11027t3.jpg] [js11027t1.jpg] [js11027f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}