 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 16, No. 2, July/August, 2011, pp. 46-54 Comparing Aspiration and Non-aspiration Fine Needle Techniques in Cytodiagnosis of Thyroid Nodules 1Kiwoko
Hospital, 2Surgery Department, Mulago Hospital, 3Pathology
Department, Faculty of Medicine, Makerere University. Background: Nodular goitre remains a problem of
enormous magnitude with an estimated prevalence of 19 to 35% worldwide. Of all
thyroid nodules 5-10% are cancerous and require surgery. By identifying the
benign ones unnecessary surgery, the associated morbidity and associated costs
could be avoided. Fine needle cytology is recommended as the initial
evaluation of thyroid nodules. Its main limitations are inadequate cellular
harvest and indeterminate results. Aspiration (FNA) and non-aspiration (FNNA)
techniques were evaluated in this study for purposes of judging which technique
is better for cellular harvest. In
providing the standard amount of follicular cells for cytodiagnosis (SAFC). Nodular goitre remains a problem of enormous
magnitude with an estimated prevalence ranging from 19% to 35% worldwide.1
Thyroid nodules are evaluated to identify those that are cancerous, and account
for approximately 5-10% of nodules. These require surgery. By identifying
benign nodules unnecessary surgery is avoided.1, 2,3. In Uganda, at Mulago hospital, nodular
goitre accounts for about 82% of goitres.4. Kobusingye5
found a high incidence of cancer of 19.6% of nodules from histopathology
reports at Mulago. Fine needle biopsy
(FNB) is the most accurate, cost effective and simplest screening test for the
rapid diagnosis of the cause of thyroid nodules and it has become widely
acceptable as an initial test.2, 6, 7, 8-14. The main limitation of
FNB is inadequate specimen and indeterminate results3, 8. The
techniques of FNB used are aspiration (FNA), and non-aspiration fine needle
techniques (FNNA). Various studies comparing these two techniques have yielded
conflicting results regarding adequacy of specimen. Some have shown FNNA to be
simple and to significantly produce superior quality material with less pain
and discomfort to the patient compared to FNA.15-21. At Mulago
hospital, FNA, the commonly used technique, had about 50% inadequate results.22
The effectiveness of FNNA is unknown. If
FNNA is better, it will reduce the rate of both inadequate specimen and repeat
biopsies as well as the cost incurred thereof. There is a need to determine the
usefulness of FNNA compared to the conventional FNA in our environment in
providing the SAFC of thyroid nodules and ensuring safe, reliable and effective
screening of thyroid nodules. This cross sectional descriptive study was
carried out at Mulago Teaching and National Referral Hospital in Kampala,
Uganda over a 4months period. Patients were recruited from the surgical and
medical Endocrine units as well as Breast unit. The study population included
all patients who presented with thyroid nodules, fulfilled the inclusion
criteria and gave an informed consent.
They underwent the routine clinical evaluation by the attending
physician. Those with clinically palpable thyroid nodules were enrolled into
the study. Eligible patients were consecutively recruited, and then each
patient had both FNA and FNNA on their thyroid nodule The thyroid nodules, identified were
randomly assigned and measured their widest diameters in centimeters using
Vernier calipers and aspirated. The nodules chosen for biopsy were those which
were:
Equipment used included glass slides, cover
slips, antiseptic, disposable gloves, fixative (absolute ethyl-alcohol) in a
Coplin jar, swabs, French gauge 23(23 FG) hypodermic needles, and 10 milliliter
syringes.14Using a diamond pencil, one end of each slide was labeled
with the patients’ laboratory number. Slide labels with the initials A for FNNA
specimen, B for FNA specimen was also used. The biopsies were carried out on
patients lying supine on a couch supported by a pillow behind the shoulders.
They were instructed not to talk or swallow as the biopsy was taken. After gloving, the skin overlaying the
thyroid nodule was cleansed with antiseptic-ethyl alcohol in a swab. The nodule
was immobilized between the index finger and the thumb. In performing FNA, a 23
FG needle, attached to a 10ml syringe, was inserted into the nodule. The
plunger was retracted to create a vacuum in the needle for suction. Using
forward and backward movements under constant suction the needle was moved at
different depths and angles within the confines of the nodule thus sampling
multiple areas. The biopsy manoeuvre was terminated when fluid appeared in the
hub of the needle. The plunger was released to prevent aspiration of the
material into the syringe before recovering the needle from the nodule. The
needle was then removed from the nodule, and the syringe detached. The syringe
was filled with air and then re-attached to the needle. Using the air, with the
needle tip close to the slide, the sample was expressed onto the slide. With a
swab, the patient applied firm pressure over the biopsied area. FNNA Technique: For this technique, a 23 FG hypodermic needle, held directly
between the thumb and index finger of one hand, was inserted into the nodule.
The needle was repetitively moved back and forth and twirling it within the
nodule. The biopsy manoeuvre was terminated when fluid appeared in the hub of
the needle. The needle was withdrawn then using an air-filled syringe the
needle contents were expelled onto a labeled slide for smear preparation as in
FNA above. Using a swab the patient
applied firm pressure over the biopsied area for at least 5 minutes to reduce
the chances of haematoma formation. For each nodule, FNA and FNNA were
performed as far apart as possible Smear preparation: The aspirated material was
smeared on a slide labeled with the patient’s laboratory number. Another
labeled slide was placed on the smear to thinly and evenly spread the smear
between the two slides on pulling them apart. One slide was immediately
immersed into absolute ethyl-alcohol fixative while the other was air-dried. Staining and smear evaluation: The air-dried smears were stained
with a modified Wright stain (Diff Quik) The slides were examined for the
standard adequate amount of follicular cells for cytodiagnosis and the
cytodiagnosis made. The cytopathologist and laboratory technician covered the
slides with cover slips for preservation. The PI re-labeled each slide
according to the technique used as A for FNNA and B for FNA. The
cytopathologist was blinded to the biopsy technique used. The slides were then
presented to the cytopathologist to be examined for the number of groups of
follicular cells and for the cytologic diagnosis. All the smears were evaluated
by the same cytopathologist. Cytology results were categorized into the four
groups suggested by the Papanicolaou Society of Cytology as non-diagnostic,
benign, indeterminate, and malignant.33 Smears with insufficient
number of follicular cells were considered non-diagnostic. Results were
recorded in another register. Ethical
approval was sought prior to commencement of the study. Analysis Data was corrected and entered
into SPSS version 12. At univariate analysis data was analyzed for frequencies
and proportions. Bivariate analysis was done using odds ratios and p-values.
Where the data was not normally distributed, the Wilcoxon Signed Ranks test was
used to compare paired medians of the same sample. The two techniques were
analyzed as matched pairs for each nodule. For the paired samples in which one
technique gave the SAFC and the other did not, analysis was done using
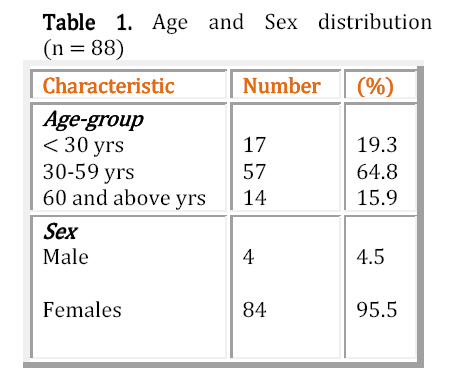
McNemar’s test statistic. Odds ratios were calculated for discordant pairs. The study involved 88 patients, in whom 100
nodules were biopsied. The
patients’ age range was 19 to 70 yrs (mean 43yrs) and 95.5% were females. Table
1 shows the age and sex
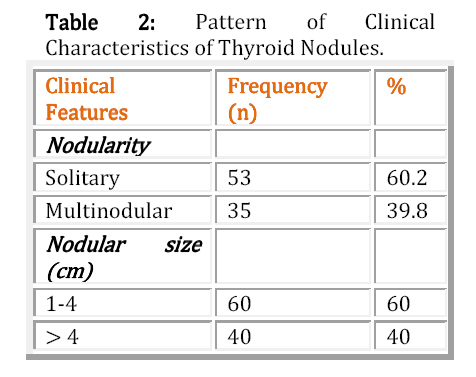
distribution. Table 2 shows the pattern of
clinical characteristics of thyroid
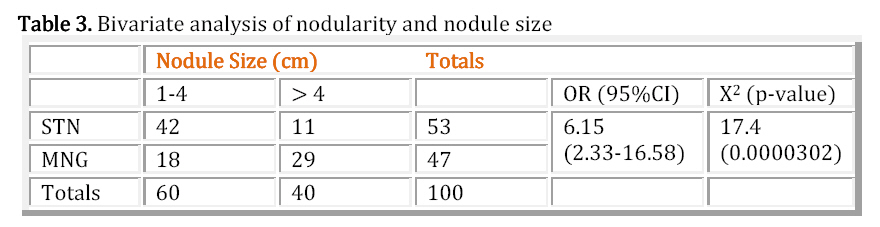
nodules. Table 3 shows the bivariate analysis
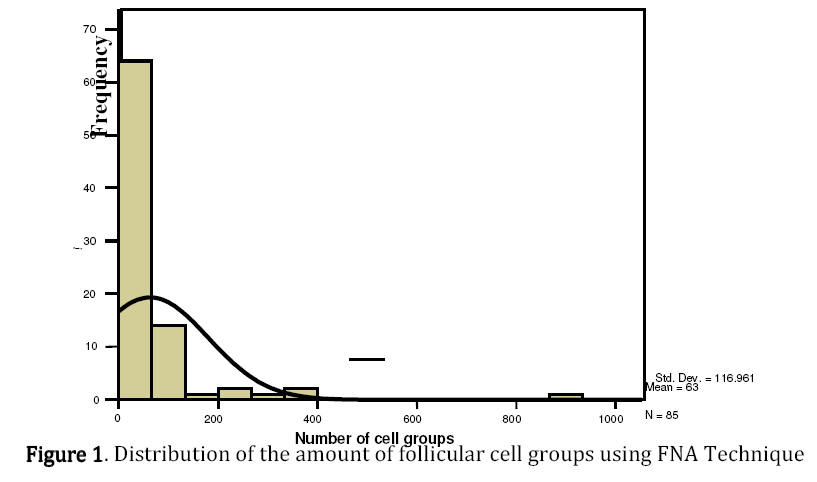
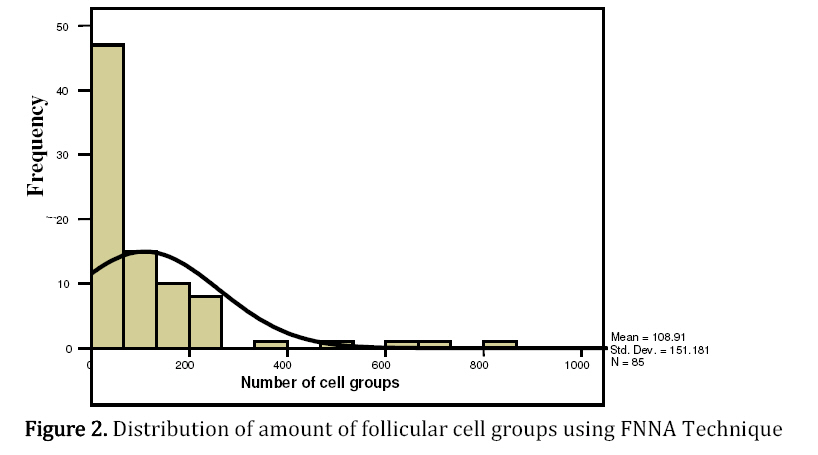
of nodularity and nodule size. Follicular cell counts for eighty-five
nodules were available for statistical analysis. In this study, FNNA technique
provided a greater mean cell count than did FNA. (108.9 vs. 63, p=0.01).
(Figures 1 and 2).
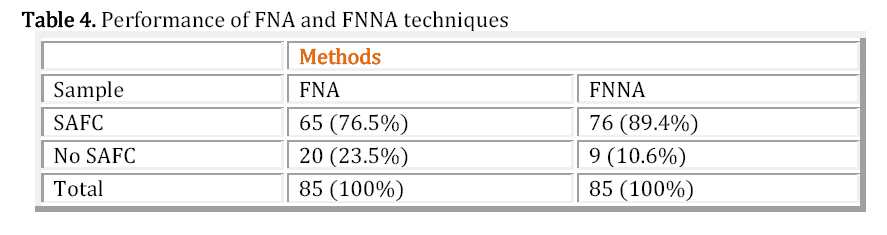
The proportion of nodules with smears having SAFC using FNNA was 76/85 (0.894)
compared with 65/85 (0.765) using FNA (Table
4). The
difference between the proportions was therefore 0.129, 95% C.I, 0.053 – 0.206.
This means that the rate of providing the SAFC was between 5.3% and 20.6%
higher if FNNA was used than if FNA was used. FNNA was significantly superior (p< 0.01) to FNA in providing the SAFC. In two nodules (2.3%), FNA yielded the SAFC while FNNA did not. Both of the nodules measured 1-4 cm in their widest diameter. One nodule was a solitary thyroid nodule while the other was in a multinodular goitre. Previous studies by Ciatto et al, and Mariyan et al among others similarly showed superiority of FNNA, p< 0.01.17, 19, 20, 26, 27, 32. However, Suen found FNA to provide more cells than FNNA in some cases and vice versa in others25. On the other hand, Ghosh et al found that FNA was superior to FNNA. The difference is statistically significant18. The FNNA technique draws up cells by
capillary action with minimal dilution with blood. The FNA technique, on the
other hand, is not infrequently complicated by aspiration of significant
quantities of blood, which compromises cellular concentration, preservation,
and interpretation. This is the likely reason for the provision of more cells
by FNNA. 2,6,23,24 Fine needle biopsy of the thyroid is widely
used in the cytodiagnosis of thyroid nodules since it is quick, safe,
inexpensive and reliable. Inadequate cell harvest is a major limitation, while
previous studies comparing FNA and FNNA techniques with regard to this
limitation show conflicting results3,8,17,20,25. Over a four months period, eighty-eight
patients with thyroid nodules were recruited from the medical and surgical
endocrine clinics. In this study, FNNA technique provided a
greater mean cell count than did FNA. (108.9 vs. 63, p=0.01). The proportion of nodules with smears having
SAFC using FNNA was 76/85 (0.894) compared with 65/85 (0.765) using FNA. The
difference between the proportions was therefore 0.129, 95% C.I, 0.053 – 0.206.
This means that the rate of providing the SAFC was between 5.3% and 20.6%
higher if FNNA was used than if FNA was used. FNNA was significantly superior
(p< 0.01) to FNA in providing the SAFC. In two nodules (2.3%), FNA yielded
the SAFC while FNNA did not. Both of the nodules measured 1-4 cm in their
widest diameter. One nodule was a solitary thyroid nodule while the other was
in a multinodular goitre. Previous studies by Ciatto et al, and Mariyan et al
among others similarly showed superiority of FNNA, p< 0.01.17, 19, 20,
26, 27, 32 However, Suen found FNA to provide more cells than FNNA in
some cases and vice versa in others25. On the other hand, Ghosh et
al found that FNA was superior to FNNA. The difference is statistically
significant18. The thyroid gland is very vascular. The FNNA
technique employs capillary action, which draws up the cells into the biopsy
needle while the FNA employs high suction pressures. The FNNA technique draws
up cells by capillary action with minimal dilution with blood. The FNA
technique, on the other hand, is not infrequently complicated by aspiration of
significant quantities of blood, which compromises cellular concentration,
preservation, and interpretation. This is the likely reason for the provision
of more cells by FNNA 2,6,23,24. Common technical errors leading to
inadequate specimen include aspirating a mass without a syringe holder,
aspirating a mass without moving the needle back and forth through the specimen
and aspirating of air after the biopsy is completed and the needle is
withdrawn, allowing the specimen to be lost in the syringe28. In
this series, in 20/85 (23.5%) of nodules the specimen was inadequate. This may have partly been contributed
to by not using a syringe holder and the loss of part of the specimen in the
syringe. During biopsy, it was more cumbersome aspirating the smaller nodules
while maintaining suction in the syringe when using the FNA technique. The FNNA
technique afforded better control of both the needle and nodules during biopsy
than did the FNA technique. This has been observed by other researchers as well29.
It was difficult to control the syringe movement while maintaining suction with
one hand when using the FNA technique. Where the syringe holder is not
available for FNA, the biopsy material can easily be sucked up into the
syringe. This is makes it difficult to express onto slides. The reasons could
have contributed to worse performance of FNA. In the present study, biopsies
were performed by a single operator. This avoids bias introduced by differing
skills and experience by different performers15, 27. The possibility
of trauma caused by the first procedure affecting the outcome of the second was
minimized by placing the punctures as far apart as possible. In this study, nodule size in diameter was
categorized into < 1cm, 1-4cm, and > 4cm. There were no nodules in the
< 1cm category. Thyroid nodules with widest diameter
Makoba4 in his study found that
regarding nodular thyroid disease, clinical diagnosis was made in 48.8% of the
patients while with ultrasonography it was 82.2%. Other studies found that about 50% of solitary nodules on palpation,
were multiple nodules on ultrasound evaluation30. This implies that
the multinodular goiters in this study was an under estimation and that some
nodules were probably missed. Similarly, clinical determination of nodule size
using Vernia calipers is likely to have over-estimated nodule size. The widest
diameter clinically might not be real because of inaccessibility. There were no
nodules of diameter <1 cm. These could have been missed because of there
position, being inaccessible. The use of ultrasound to determine nodule sizes
would certainly give more accurate measurements as other researchers have found4. For each of the techniques the difference in
providing the SAFC from the different nodule sizes was not statistically
significant. These findings suggest that no particular technique performed
better with regard to nodule size. Brownridge et al15 had similar
findings. It is likely that patients with smaller
nodules in this case < 1cm widest diameter had sub-clinical nodules and
therefore, were not recruited. The current study did not undertake to screen
thyroid glands for sub-clinical nodules, neither were any biopsies done using
ultrasound. The main indication for ultrasound-guided FNA/FNNA is following
unsatisfactory biopsy by palpation32. Bivariate analysis demonstrated a tendency towards a larger cell
provision in nodules 1-4 cm category, however possibly because of the small
sample size, the statistical significance of this could not be demonstrated by
the current study. Larger nodules tend to have centres undergoing degeneration
and less numerous follicular cells as compared to small ones.3 This
probably is one of the reasons for a larger cell provision in the smaller 1-4cm
nodules. Even though the order of FNA or FNNA was
randomly assigned and these were performed as far apart as possible, it is
conceivable that some bias would be introduced especially to the technique that
was performed second. However random assignment minimizes this limitation. In assessment of thyroid disease without
Ultrasound scan, thyroid nodules could be missed. Thyroid nodules are better
assessed with FNNA, which is less technically challenging and does not require
a syringe holder. The association between the diameter of the thyroid nodule
biopsied and the provision of adequate standard amount of follicular cells for
cytodiagnosis of thyroid nodules using either FNA or FNNA at Mulago was not
statistically significant.
Copyright 2011 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js11029f1.jpg] [js11029t1.jpg] [js11029f2.jpg] [js11029t4.jpg] [js11029t2.jpg] [js11029t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}