 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 16, No. 2, July/August, 2011, pp. 55-61 Drain versus No Drain after Thyroidectomy: A prospective Randomized Clinical Study P.L. Chalya1, J.M. Gilyoma1, M.Mchembe2 1Department
of Surgery, Weill- Bugando University College of Health Sciences, Mwanza,
Tanzania Code Number: js11030 Background: Drains have been traditionally used routinely after
thyroidectomy despite limited evidence to suggest any benefit. We conducted a
prospective randomized clinical study to evaluate the necessity of drainage
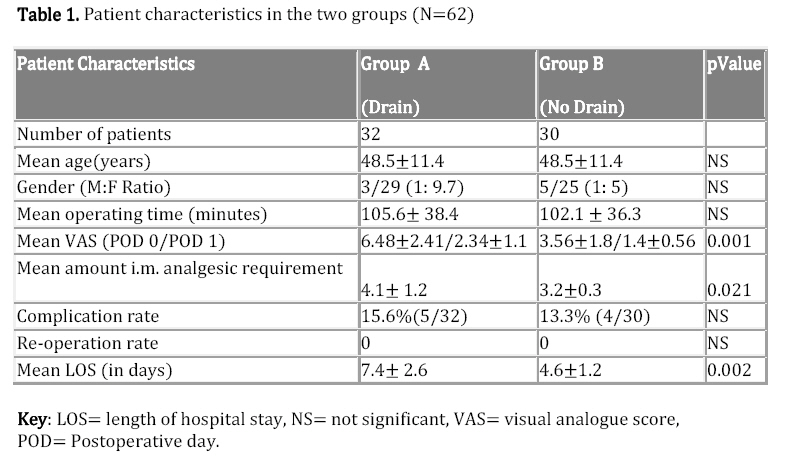
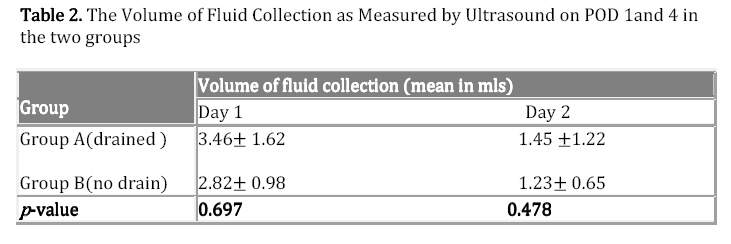
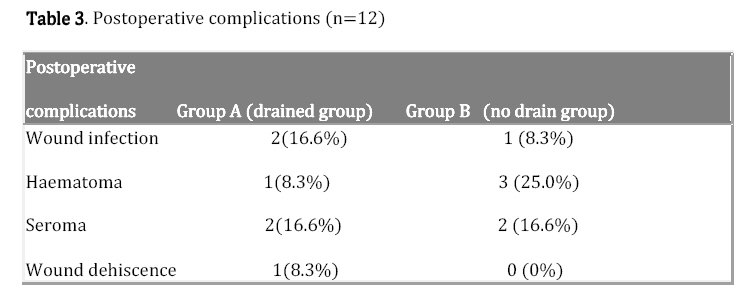
after thyroid surgery. Introduction Thyroidectomy is one of the most commonly performed operative procedures in general surgery and may be associated with complications if not performed by experienced surgeons 1. Postoperative hemorrhage is a well known complication of thyroidectomy that requires special attention since this may be life-threatening due to acute airway obstruction 2. Traditionally, many surgeons routinely use drains after thyroidectomy so as to drain off a possible postoperative haemorrhage, which may compress the air passages and produce respiratory failure3,4. This fear prompts to surgeon to use routine drains after any type of thyroid surgery1-4. The need for use of drains in thyroid surgery has been debated for the past two decades 5. Numerous recent randomized trials have failed to show any benefit of drainage in thyroid surgery and concluded that routine drainage is unnecessary after thyroid surgery6-9. Most of these studies have documented that the use of drains contribute to the discomfort of the patients, increase the rate of surgical wound infections, prolong the length of the hospital stay and thereby increase the cost, and deteriorate the cosmetic result7,8,9. Despite lack of evidence in many randomized clinical trials in support of the routine use of drains after thyroid surgery, many surgeons in many centres including ours still advocate the routine use of drains post-thyroid surgery. This prospective randomized clinical trial was aimed at evaluating the need for using drains after thyroid surgery in our setting. Patients and Methods This was a prospective randomized clinical study which was conducted in the surgical wards of Bugando Medical Centre (BMC) between March 2009 and February 2010. BMC is 1000-bed, tertiary care and teaching hospital for the Weill-Bugando University College of Health sciences (WBUCHS). All patients who underwent thyroidectomy during the period under study were eligible for the study. Preoperatively, hematological tests and coagulation profile, along with thyroid hormone profile and FNAC were undertaken. Patients who had very huge vascularized goitre, thyroid cancer, clinical or laboratory evidence of coagulopathy and those who underwent thyroidectomy with neck dissection were excluded from the study. All patients who met the inclusion criteria were, after informed written consent, consecutively enrolled in the study. Approval to conduct the study was sought from the WBUCHS/BMC joint institutional ethic review committee before the commencement of the study. The patients included in the study were randomized into two groups according to whether drains were inserted at the time of surgery or not. A computer program (random number generator, Microsoft excel 5.0) was used to generate random number list, whereby patients were assigned to either of the two groups i.e. Group A consisted of patients with drains and group B consisted of patients without drains. The randomization was provided by a computer consultant. The surgeon was informed of the drains insertion just before the closure of the wound. Study variables recorded included, operating time, postoperative pain, amount of intramuscular analgesic requirement, Volume of fluid collection in thyroid bed, hospital stay, post-thyroidectomy complications, and necessity for re-operation. The operating time was defined as the time from the first incision to the last suture's placement. Postoperative pain was assessed according to a visual analogue scale (VAS) from 0 (no pain) to 10 (worst pain imaginable) on the postoperative day 0 and 1. Postoperatively, ultrasound of the neck (using B mode with linear frequency of 7.5 MHz) to assess the amount of collection of thyroid bed was done to all patients in the two groups on first and seventh postoperative day by the same ultrasonologist each time. The patients were discharged when the patients did not have any complication or no longer required intramuscular analgesics, regardless of whether the patient felt enough to discharge, after the drain was removed, if drained. The drains were removed in all the patients after 48 hours. Before the present study was contemplated, a pilot study was carried out on 15 patients (excluded from the present study) to ascertain the duration of drainage and the drains were removed after the drainage reduced to less than 30 ml in 24 hours following which the patients were discharged. The study patients were followed up for seven days at the end of which were asked to measure their overall level of satisfaction (1=poor, 2= fair, 3=good and 4=excellent). Data were collected using structured questionnaire and analyzed using SPSS computer software version 11.5. Continuous variables were analyzed using means, standard deviation and compared using independent sample t-test. Categorical variables were analyzed using frequencies and percentages and compared using the chi-square (c 2). The 95% confidence interval (95% CI) was calculated where appropriate. Statistical significance was set at p-value of less than 0.05. Results A total of 67 eligible patients admitted to Bugando medical Centre for elective thyroidectomy were approached for the study. Out of those 67 eligible patients, five patients were excluded from the study because one patient refused to consent for the study and the remaining four patients; one each had thyroid cancer, clinical evidence of coagulopathy, very huge vascularized goitre and thyroidectomy associated with neck dissection respectively. Hence, 62 patients, 58 (93.5%) females and 4 (6.5%) males (F: M= 14.5:1) aging between 21 and 67 years (mean 48.9 ± 24 years), were enrolled and consented to participate in the study. Thirty two patients were eventually randomized to Group A (drain group) and thirty patients to Group B (no drain group). No randomized patients withdraw from the study. All 62 patients were included in the subsequent analysis. The two groups were equally distributed according to age, sex, the size of the gland and the type of procedure performed. Group A (drained group) consisted of 3 males and 29 females (M: F = 1: 9.7) with a mean age of (48.5±11.4) years. Group B (non-drained group) comprised of 5 males and 25 females (M: F= 1: 5) with a mean age of (46.7±14.6) years. There was no statistically significant difference in the gender and age between the two groups (P = 0.781). The mean operating time in Group A (drained group) was 105.5±38.4 min and in Group B (non-drained group) was 102.1±36.3 min. The difference between the two groups was not statistically significant (P = 0.756). The mean VAS was significantly reduced more in Group B (non-drained group) than in Group A (drained group) patients on postoperative day 0 (P =0.001)and 1 (p-value =0.011) respectively. The mean amount of intramuscular analgesic requirement was significantly less in the non-drained group than in the drained group (P= 0.021). Table 1 shows patient characteristics in the two groups. The amount of fluid collection in thyroid bed as measured by ultrasound for both the groups on day one and day four is shown in Table 2. There was no statistically significant difference in the volume of fluid collection on day one (P = 0.697) and day four (P = 0.478) between the two groups. Twelve complications were recorded in 9 out of 62 patients giving an overall complication rate of 14.5%. The complication rates in the drain and no drain group were 15.6% (5/32) and 13.3% (4/30) respectively. The difference between the two groups was not statistically significant (P = 0.218). Table 3 shows postoperative complications between the two groups. No patient needed surgical revision or re-operation for any complication and all complications were successfully managed with palliative care. The average duration of hospital stay was 3.6±1.8 days for the entire group. The mean hospital stay was significantly shorter in the non-drained group when compared to the drained group (4.6±1.2) versus 7.4 ± 2.6 days) (P = 0.002). The satisfaction of patients was found to be superior in the non-drained group. Discussion Drains after thyroidectomy have traditionally been used in many centres worldwide despite lack of evidence to suggest any benefit6,7,8. Classic teaching in surgery has dictated that drains should be used routinely after thyroid surgery so as to prevent postoperative complications by evacuating postoperative hematoma or lymphatic fluid in the thyroid bed and to alert the surgeon to early postoperative bleeding1-4. This anecdotal based teaching and practice has been challenged by recent randomized clinical trials6-9.These randomized clinical trials have failed to provide clear evidence that using drains in patients undergoing thyroid operations significantly improves patient outcomes6,7,8,9. Most of these studies have suggested that routine use of drains after thyroid surgery is unnecessary and contribute to the discomfort of the patients, increase the rate of surgical wound infections, prolong the length of the hospital stay and thereby increase the cost, and deteriorate the cosmetic result7,8, 9. Although several prospective randomized reports regarding the functioning of drains in thyroid surgery have not justified their use, most surgeons still advocate routine drainage of the thyroidectomy bed with an effort to monitor a potentially life-threatening complication of postoperative bleeding6-10. In agreement with other clinical trials 6-9, the present prospective randomized study has failed to demonstrate any benefit of routinely using drain after uncomplicated thyroid surgery. This study have shown no statistically significant difference in the mean operating time, volume of fluid collection in thyroid bed, complication rates and the necessity for re-operation between the two groups. However, the mean VAS and the amount of intramuscular analgesic requirement were significantly more in the drained group (Group A) and the length of hospital stay was significantly prolonged in this group. Most randomized clinical trials have advocated use of drains in patients with huge goitres, thyroid cancer, clinical or laboratory evidence of coagulopathy and those who underwent thyroidectomy with neck dissection as these are more extensive operations and drains are necessary in this situation5,7,11. Similar exclusion criteria were also applied in our study. This practice is in contrast with Seung et al12 who reported that thyroidectomy without drains is safe and effective even in more extensive thyroid surgery and appears to confer several advantages over the routine drainage method and achieves significant reduction of hospital stay, which led to a reduction in costs for the patients. There is however strong arguments against the use of wound drains after thyroid surgery; they often become blocked by clotted blood13 and collections of blood or tissue fluid (seroma) can occur in spite of drains4, 6, 14. In addition airway compromise can occur due to other causes such as nerve injury, laryngeal edema15-17. Drains can increase the infection rate 10, 18 and are associated with increased pain14 and they add to discomfort, give extra scar and increase hospital stay8. Drain usage has been questioned after various types of surgeries with much larger potential dead spaces in other areas such as colorectal19, plastic surgery20, vascular 21 and orthopedics22. These procedures are now routinely not drained. Previous reports have also reported that the drain being a foreign body may induce reactive fluid formation, thus encourage formation rather than preventing fluid collection8. The present randomized clinical study failed to demonstrate any benefit of routine use of drains in uncomplicated thyroidectomy. However, the hospital stay was found to be shorter and pain scores were smaller in the non-drain group (Group B). Therefore, we concluded that routine prophylactic drainage was not essential in uncomplicated cases of thyroidectomy. Importantly, we achieved significant reduction in postoperative pain, the amount of intramuscular analgesics requirement and the duration of hospital stay in no-drain group, leading to a reduction in costs for the patients and increased satisfaction of patients. Conclusion The study has demonstrated that routine drainage of the thyroidectomy bed is unnecessary and may be abandoned after uncomplicated thyroid surgery, as it is not effective in decreasing the rate of postoperative complications resulting from post-thyroidectomy haemorrhage. Furthermore, drainage causes a prolonged hospital stay and increased postoperative pain and the amount of intramuscular analgesic requirement. So, by ensuring meticulous hemostasis drains can be avoided in uncomplicated thyroid surgery. Acknowledgements The authors would like to thank the staff and nurses of the surgical department at Bugando Medical Centre for their excellent care they provided to our patients. Special thanks go to Dr Mkumbo, Head of Radiology Department for his assistance in ultrasonographic work up. References
Copyright 2011 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js11030t2.jpg] [js11030t1.jpg] [js11030t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}