 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 16, No. 2, July/August, 2011, pp. 62-71 Peritoneal Drains in Perforated Appendicitis without Peritonitis: A Prospective Randomized Controlled Study. P. G .Jani1, P.N. Nyaga2, 1Dept.
of Surgery, College of Health Sciences, University of Nairobi. Code Number: js11031 Background:
Appendicitis is recognized worldwide as the commonest surgical emergency. Its
management becomes more challenging when the patient presents with perforated
appendicitis In the western world To determine the value of peritoneal drains
in patients operated with an appendicular pathology more advanced then simple
acute appendicitis (referred as advanced appendicular pathology). Patients with
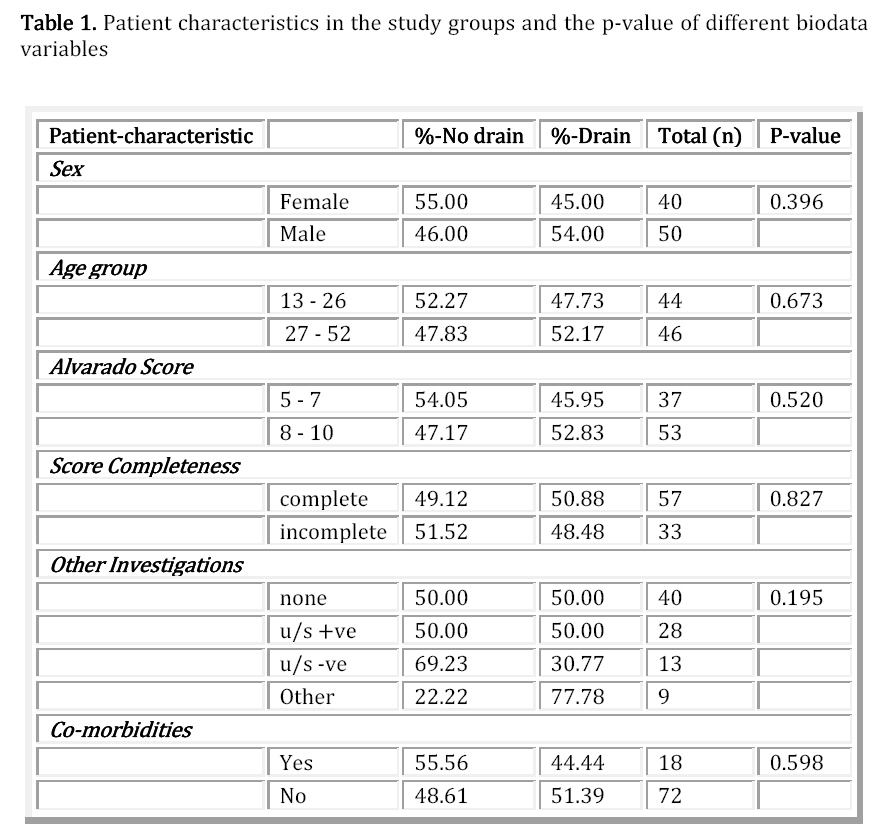
generalized peritonitis secondary to an appendicular pathology were excluded. The management of acute appendicitis at Kenyatta National hospital, Nairobi Kenya, has routinely been to use peritoneal drains whenever an advance appendicular pathology is encountered at operation. This is in addition to peritoneal lavage with normal saline1,2. Harlan et al3 on a study focused on abdominal drainage following appendectomy and cholecystectomy showed no difference in outcome when drains were used on simple appendectomy, but significantly higher infectious complications in gangrenous or perforated appendicitis. In this study, penrose drains were used and all stages of appendicitis were included with drains exteriorlized through the main incision wound. A systemic review and meta- analysis by Petrowsky et al4 showed that many gastro intestinal operations can be performed safely without use of prophylactic drainage. They did not find evidence for use of prophylactic drains in any stage of appendicitis. However, some of the studies included in the review did not report on their exclusion criteria, others excluded patients with severe intraperitoneal sepsis and appendiceal abscesses. Recognizing these limitations the reviewers called for well designed randomized controlled studies to clarify the value of prophylactic drainage in perforated appendicitis. There is no consensus on the use of peritoneal drains, while evacuating an established collection is a clear indication for therapeutic drains; prophylactic drains are placed in anticipation of complications, they are expected to signal leakages or hemorrhage early. These drains are also anticipated to prevent further collections in the cavity. Opinions on the practice are divided, some believe peritoneal drains are useless and do not work while others insert drains routinely, sometimes as safety valves5. The purpose of this study was to evaluate the efficiency and the value of prophylactic peritoneal drainage in patients with advance appendicular pathology at Kenyatta National hospital. Patients and Methods This was a randomized prospective trial undertaken at Kenyatta National hospital, which is the leading referral centre in Kenya and a teaching hospital for the University of Nairobi. All patients managed in the general surgical wards for advanced appendicular pathology and aged over 13 years old were included in the study. Patients with a simple acute appendicitis or patients who had a laparoscopic appendisectomy were excluded from the study. Patients were recruited from casualty or admitting general surgical wards. The procedure was explained and a note was made of patient’s demographic profile, presenting symptoms and duration of symptoms prior to presentation to hospital. The patients with known comorbidities were also noted. Previous treatment received especially antibiotics were recorded. Also noted were any investigations done before arrival and during clinical work up. The patient was examined and further investigations ordered the most important being total WBC count and differential counts. A modified Alvarado score table was then completed or filled as per information available and relevant antibiotics were prescribed. In theatre, patients were classified into four groups depending on gross pathological findings:-
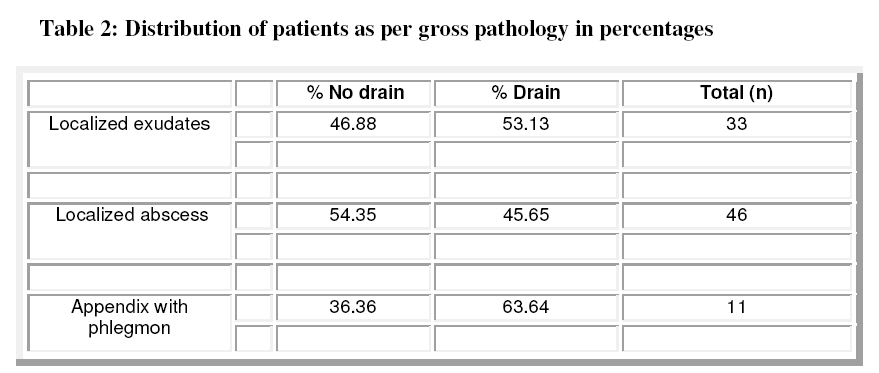
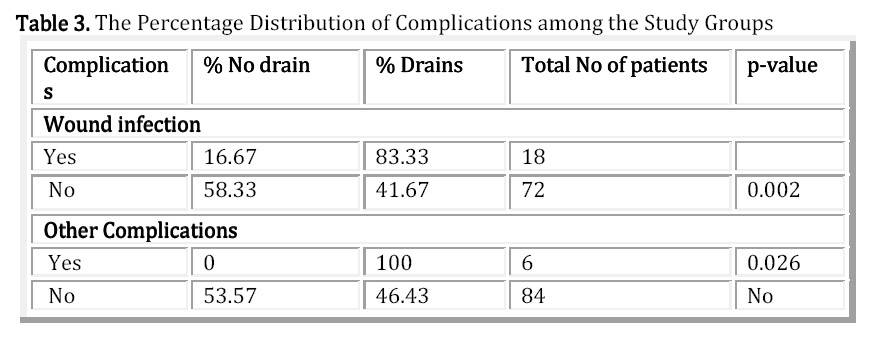
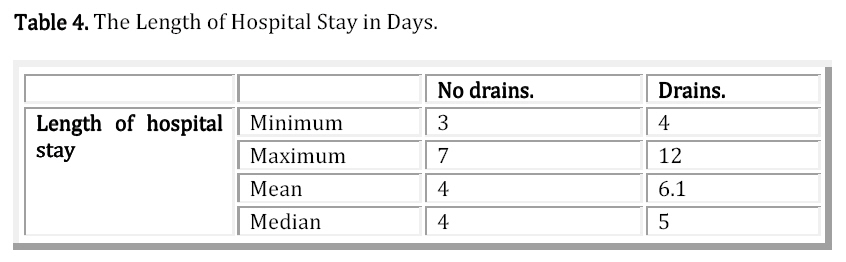
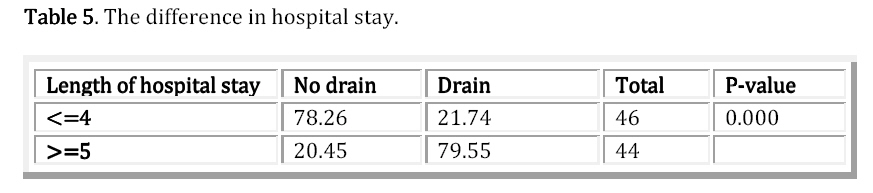
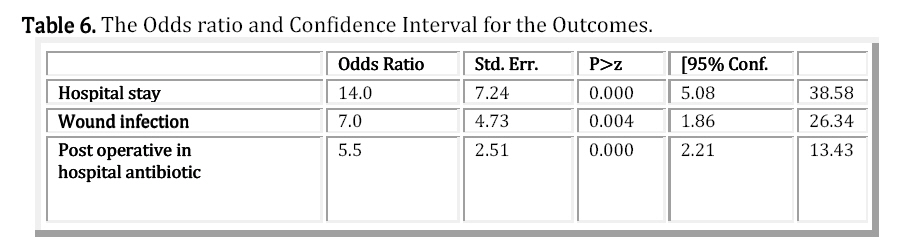
All the patients with perforated advanced appendicular pathology had appendisectomy performed with evacuation of all gross pus, exudates and a thorough warm saline lavage until the effluent was clear of contamination and the operation bed was clean. Just before closure a tube drain was fixed from the appendectomy site through a separate incision anchored with a stitch and connected to a sterile urine bag that acted as drain reservoir. A PVC suction catheter was used as the drain as these were the only types of drains available. The drain exit incision was dressed separately from main incision wound. The main incision wound was closed with interrupted stitches to the fascia and skin in both groups and dressed. Wound dressing were soaked in povidone 10% solution and held in place by strapping. All patients had antibiotics prescribed postoperatively. Various combinations were used depending on availability in the hospital at the time. The regimens were meant to cover both gram negative and positive pathogens plus added cover for anaerobes. The drugs used included cefuroxime, and metronidazole combination or penicillin, gentamicin and metronidazole combination or amoxicillin-clavulinate and metronidazole combination. Which ever was available was used. Both groups received similar antibiotics in dosage and class. All antibiotics were administered intravenously for the period the patient was in the hospital. All patients were discharged when fever settled or white blood cell count normalized and were feeding orally. Antibiotics were stopped earlier if patient recovered quickly or were changed on basis of culture and sensitivity. At times they were extended when septic complications occurred. All the appendisectomy specimen were sent for histology. Postoperatively, patients were admitted and treated in the general surgical wards. The investigators followed and recorded patient progress in a questionnaire until discharge. During the daily visits the consistency and amount in the drain reservoir was estimated and recorded, (all volumes were estimated to the nearest 50 ml mark). The wounds were inspected and their status noted. The total duration of drain activity was noted and recorded in days. Those who had further investigations e.g abdominal ultrasonographic scans were noted and also other complications such as fistula formation. Infected wounds had the growth from pus swab noted. The types and duration of antibiotic also recorded. Data collected was tallied into tables and analyzed using STATA version 9.2. Statistical analysis comparing drain group and no drain group was calculated using the Fisher’s exact test for categorical variables and Student’s t-test for continuous variables. Statistical significance was accepted when p < 0.05. Logistic regression was used to assess the probability of occurrence of various outcomes between the two groups. Continuous variables were further dichotomized for analysis. Results Table 1 shows the patients characteristics in both study groups. It shows that the p-values were insignificant, indicating that the distribution resulted in comparable groups. The intra-operative gross findings were as indicated in Table 2. Of the thirty three patients with edematus perforated appendix with turbid exudates and adhesions there were 53% who had a drain inserted while 47% were managed without drain. The patients with perforated appendicitis with localized abscess were forty six. Of the thirty three patients with edematus perforated appendix with turbid exudates and adhesions there were 53% who had a drain inserted while 47% were managed without drain. The patients with perforated appendicitis with localized abscess were forty six. Of these 46% had a drain and 54% had no drain inserted. In the last category there were 11 patients with a phlegnon and these were randomized to 36% who had a drain inserted and 64% who were managed without a drain. This distribution shows insignificant difference in terms of gross pathology in the two study groups. On post-operative day I, greater than 80% of the patients with drains, drained less than 50ml. 1 patient had a drain output of 200mls. By the 3rd day it was found that 100% of the drains could be removed as the output drained was less than 50ml in all of them. The septic complications were significantly higher in the drain group as shown by the p- value calculations above. Antibiotic use. All 90 patients in the study received parenteral antibiotics covering anaerobic as well as aerobic gram positive and gram negative organism. Parenteral antibiotics were stoped once pyrexia resolved and the patients were feeding well. Forty six patients used intravenous antibiotics for up to 3 days postoperatively; 24 patients for 4 days, 20 patients for 5 days or more. 85% of those who were on antibiotics for longer than 5 days in the hospital had drains while 15% did not have drains. In addition all patients were discharged home on oral antibiotics for a period of 5 days. Overall, patients in the drain group had longer use of in-hospital antibiotics. Length of hospital stay Table 4 shows the duration of hospital stay. Patients with drains inserted stayed for an average of 6 days in the hospital as compared to patients without drains. The length of hospital stay was categorized and p value was calculated as shown in Table 5. The patients in the drain group stayed significantly longer in the hospital as shown by the significant p-value. Twenty three (25.5%) of the patients developed postoperative complications. The most common complication was wound sepsis recorded in 18 (22%) of the cases. More than 80% of the wound infections occurred in patients who had drains, only 17% of the patients without drains developed wound infection. Other complications included faecal fistula (2 patients), intraperitoneal abscess (3 patients) and paralytic ileus (1 patient) all of them occurring in patients with drains. Significance of the outcome measures. The odds ratio for prolonged hospital stay in patients with drains was 14.0, with wound sepsis and antibiotics odds ratios as shown in Table 6. This study indicated that fixing a drain in a patient with advanced appendicular pathology almost certainly ensures that they will have a prolonged hospital stay, predispose the patient to wound sepsis and hence, prolonged antibiotics use as shown by the high odds ratio and the confidence intervals calculated at 95% Confidence interval. Discussion Appendectomy is recognized worldwide as the commonest surgical emergency. In the western world; the rate of appendicitis is estimated at 10/10000, with a lifetime risk of 7%. The disease presents at a more advanced states in Africa as opposed to the western world6. The incidence of appendicitis in Kenya has been reported to be higher than the rest of the world at 428/100002. Awori found that appendectomy contributed 63% of all abdominal emergencies at Kenyatta national hospital7. The management becomes more challenging when the patient presents with perforated appendicitis. In this study we evaluated 226 patients 97 of whom had perforated acute appendicitis and its complications. This gives a complicated acute appendicitis rate of approximately 43%. This is comparable to other studies in that showed rate between 39-43% 2,7. The situation in the district hospitals could be different. A study from a rural Kenyan hospital showed a 50% presentation with perforated appendicitis8. The management of acute appendicitis is aimed at attaining a low negative appendectomy rate without increasing the complication rates. In this study the negative appendectomy rate was 12%, a significant drop since the previous study showed a rate of 23% in 20022. Internationally a negative appendectomy rate of 7-25 has been reported. There have been changes in management in our set up which include the use of the modified Alvarado score, increased availability and use of ultrasound for diagnosis and involvement of surgical registrars in evaluation of patients in casualty. The increased diagnoses of complicated acute appendicitis could be related to delay of presentation to hospital. There was a mortality rate of 0.9% in this study. A review of papers from the African continent showed the mortality rate to range from 0.9 to 4%6. Perforated acute appendicitis that presents with generalized peritonitis is associated with higher mortality. One of our patients succumbed to severe sepsis despite surgical intervention; the other was thought to be a case of post operative pulmonary complications after a relatively successful appendectomy for non perforated appendicitis, highlighting the risks associated with surgery at the extremes of the disease pathology. The study subjects in the perforated appendicitis group were 44% female to 56% male with a male to female ratio of 1.3:1. They were in the age brackets 13 -52years with children below 13 years having been excluded. Age and gender distribution was comparable to many other studies showing appendicitis as predominantly a condition in the young2,6,7,9. Some authors have argued that the characteristics of those who rapidly progress to complicated are different from others who have simple appendicitis a position that cannot be verified in this study. The delay to intervention has been shown to increase the rate of perforation. A study from India calculated that perforation in the majority of their patients occurred after 36 hours. The delay to presentation in that study was 2.5 days in those who were found to have perforated appendicitis10.Our study concentrates on complicated acute appendicitis and hence, it is not surprising the mean duration of pre-hospital stay was 4.3 days. One patient arrived after 21 days with a localized appendiceal abscess. After randomization; patients were distributed into two groups which were comparable in all aspects as shown by the statistical analysis. Age, gender, pre hospital duration of symptoms, co-morbidities and pre operative use of antibiotics showed no significant difference between the groups. This is important since significant differences in the results could be attributed to the use of drains. The modified Alvarado score was also comparable between the groups whether it was incomplete or completed. The patients were put through the similar management except in the aspect of the peritoneal drain use. The use of antibiotics has been shown to reduce the incidence of post operative infectious complications in appendicitis8,11,12,13. In complicated acute appendicitis full therapeutic regimen should be given till the resolution of fever and normalization of white blood count. The debate rages on the regimen, the dosing and the duration of these antibiotics. In our study, it was not possible to standardize the regimens due to fluctuations in availability. However, adequate drugs were available for broad spectrum and anaerobic infection coverage. The drugs used were in various combinations, cefuroxime and metronidazole, amoxy-clavullin and metronidazole and penicillin, gentamicin with addition of metronidazole. Intravenous antibiotics were used till the patient was discharged. This phase of antibiotics varied between three and five days. Fever resolved early, patients had bowel function returning faster and they ambulated quicker when no drain was used, despite similar disease state and management. Both groups had similar antibiotics treatment prescribed and administered. It is obvious that septic complications were higher in the drain group despite adequate antibiotic cover. A drain tube encourages formation of a biofilm of pathogenic organisms on its surface that cannot be eliminated until the drain is removed3. Two or more extra days of intravenous antibiotics were administered in the drain group before resolution of fever or wound discharge after drain tube removal. This contributed to more antiobiotic use and prolonged hospital stay in the drain group despite similar management in all other aspects. All patients were discharged after resolution of fever. Furthermore, a five day regimen of oral antibiotic was prescribed on discharge. There is need for a structured study and policy on use of antibiotics in acute appendicitis in our center. The peritoneal drains were used in patients with perforated appendix with adhesions and inflammatory exudation, localized abscess, appendicular phlegmon in similar fashion they had been used previously in our set up1,2. Unlike in those previous studies, there was a control group and strict follow up of patients in the present study. In the use of drains in the peritoneal cavity it has been the practice to remove the drain when the collected effluent is between 50 and 100mls. On the first day only 12.8% of the drains had collected more than 100mililitres, hence, 87.2% of the drains were not functional or there was nothing to drain. Only one of ten drains in this group was useful to the patient. All the drains did not serve any function on the second and third day. During the operation, a thorough peritoneal lavage was performed until the effluent was clear, there was no gross fluid left in the operation field and the little that could have remained was reabsorbed by the body since normal saline was used. In addition, broad spectrum antibiotics were administered. In the group that had no drains this seems to have been adequate treatment. The presence of the drain tube in the operation field in this case therefore seems either to encourage persistence of infection or reduce efficiency of antibiotics. Drains appear to be an over-treatment in the group of patients with perforated appendicitis and no generalized peritonitis. The infectious complications were encountered in both groups, this mirrors the findings by Harlan et al3 and others12,14 who had previously done randomized studies in this subject but in other centers. The average age in the study by Harlan et al3 was 26 years which was comparable to the mean of 27 yrs found in tis study. In advanced appendicitis the surgical incision infection rate was higher but not statistically different from the non drained group. In contrast our study shows a higher and significant difference in wound sepsis of patients with drains. The drain group contributed 83% of patients with wound infection in our study as opposed to 17%in the no drain group. Harlan et al found a very high incidence of intra abdominal abscess formation in the drain group where 45%of the patients with drains had intra abdominal abscesses as opposed to 15% in those without drains. Though, the incidence is very different the trend is similar; since in our study, the intra abdominal abscess formation and fistula were observed only in the drain group. A drain tube could act as an irritant to friable gut and lead to fistula formation. The formation of intra abdominal abscess suggests that the drain failed to function as expected. The finding of higher infectious complications in the drain group contrasts other studies that found no difference between the groups12,14,15. It could have been due to the exclusion criteria in those studies, since patients with appendix abscess and phlegmon were excluded. After review of the studies on drainage in gastro intestinal surgery, Petrowsky et al4 noted that intra abdominal infections were not reduced; wound infections and fistulae were increased in the drain subjects and recommended no drains in perforated or any stage of appendicitis. Our study adds to this body of evidence, however caution is required in appreciation of this data; since all other studies seem to exclude patients with generalized peritonitis secondary to perforated appendix. Patients with drains are more prone to developing post operative sepsis as shown in our study. A drain tube, being a foreign body tends to harbor infecting organisms on the bio-film that forms on its surface. Drains also require frequent handling during dressing, emptying of the reservoir, and mobilization of the patient. The presence of a drain provokes inflammatory reaction that encourages infection especially in presence of gut contaminants in complicated appendicitis. All these activities promote infectious complications post operatively. There was significant difference in length of hospital stay. Patients in the drain group had an average of 6.1 days in hospital, and they continued the use of antibiotics. It was a common observation that on removal of the drain, there was a self limiting serous exudation from the drain site and pain in most of the patients. Sometimes a sterile dressing was placed on the site for an extra day or so. If the treating team discharged the patient in this state, most patients would not leave and the nursing team would continue with the antibiotics. This practice; though not contested, contributed to the length of hospital stay in patients with drains without other septic complications. There is a concealed cost implication that was not analyzed in this study, but becomes apparent on consideration of the added days and antibiotics in the patients with drains. Patients who stay longer in the hospital have longer delay to return to work or school. Our study reveals high odds ratio for increased hospital stay and use of in-hospital antibiotics suggesting that use of drains in these patients adds to the patient’s disease burden and delays their return to normal activities. Conclusions
Reference
The following images related to this document are available:Photo images[js11031t5.jpg] [js11031t4.jpg] [js11031t2.jpg] [js11031t1.jpg] [js11031f1.jpg] [js11031t3.jpg] [js11031t6.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}