 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 16, No. 2, July/August, 2011, pp. 72-79 Typhoid Intestinal Perforations in a Tropical Tertiary Health Facility: A Prospective Study. A.O. Tade1, S.O. Olateju2, O.A. Osinupebi3, B.A. Salami1 1Department of
Surgery, 2Department of Anaesthesia and Intensive Care, 3Department
of Microbiology, Olabisi Onabanjo University Teaching Hospital, Sagamu, Ogun
State, Nigeria. Code Number: js11032 Background: Despite decades of improvement
in patient care globally, typhoid
intestinal perforation remains a frequently fatal illness in the developing
world. This study aimed at determining the factors that influenced the outcome
of surgical management typhoid intestinal perforation in Sagamu, South-West
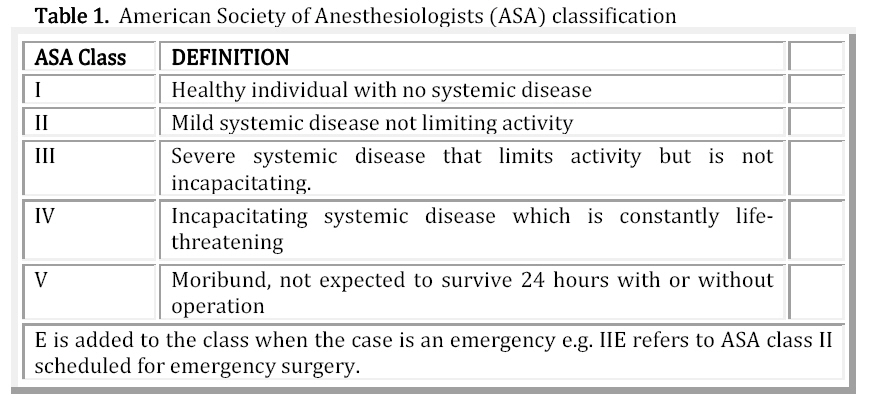
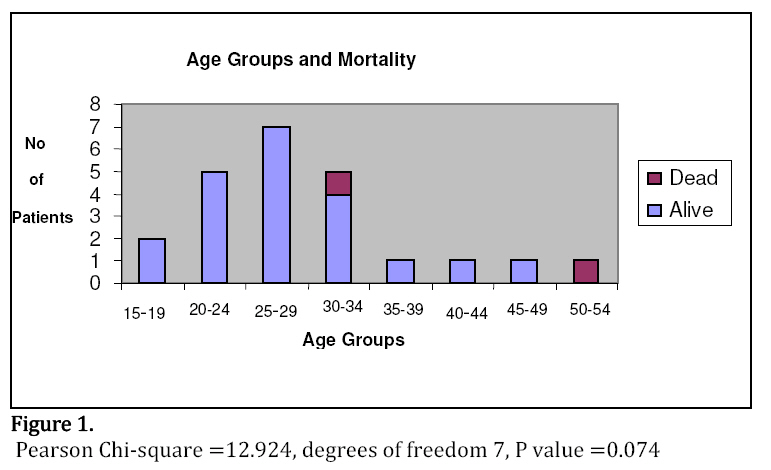
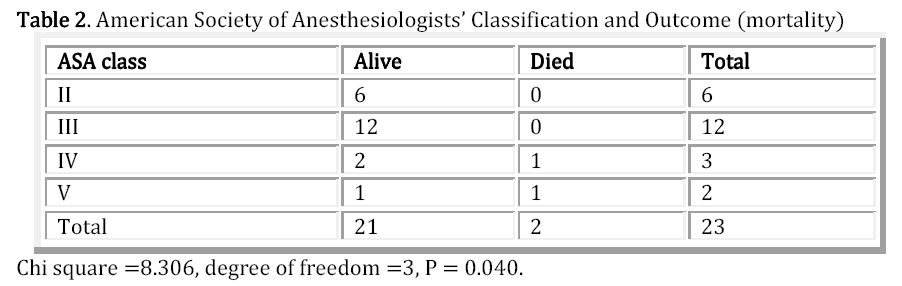
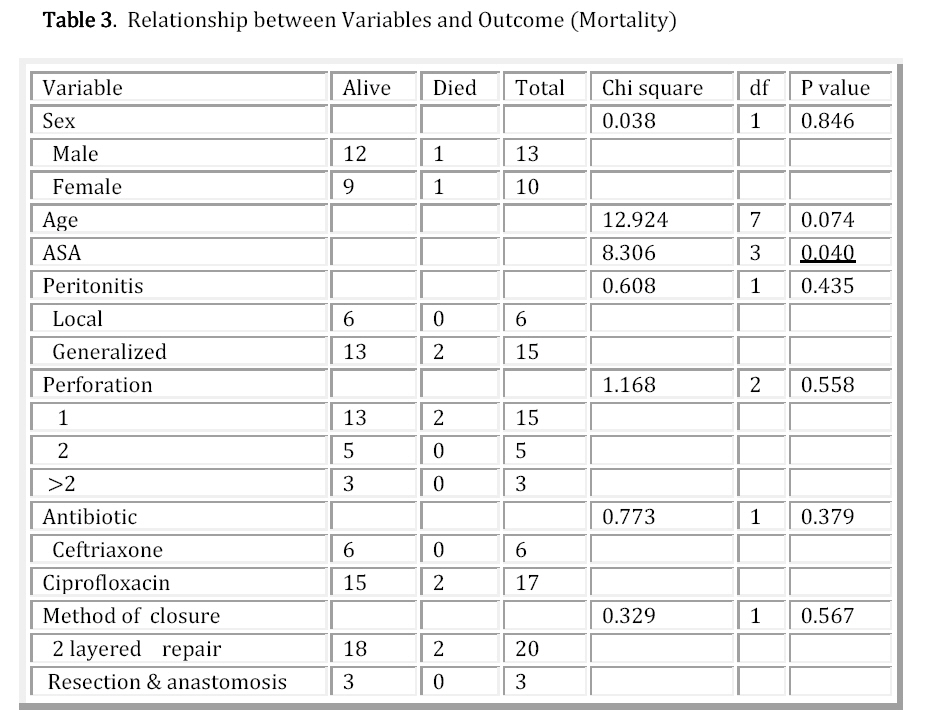
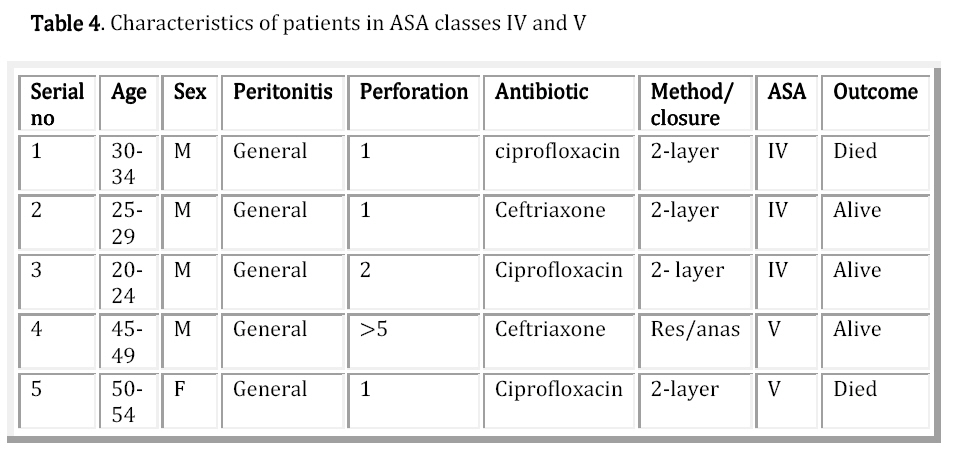
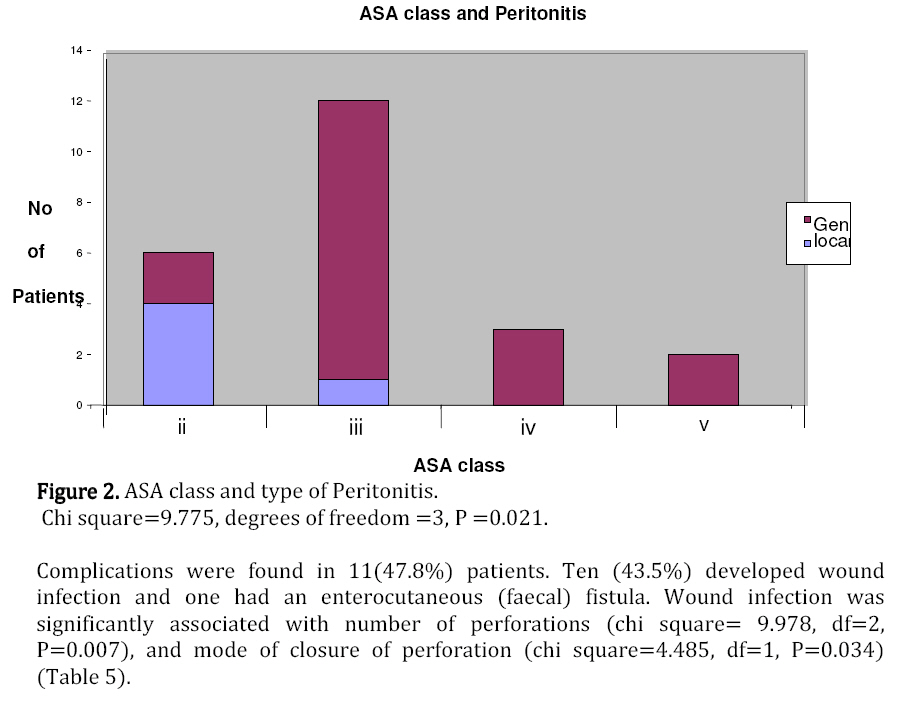
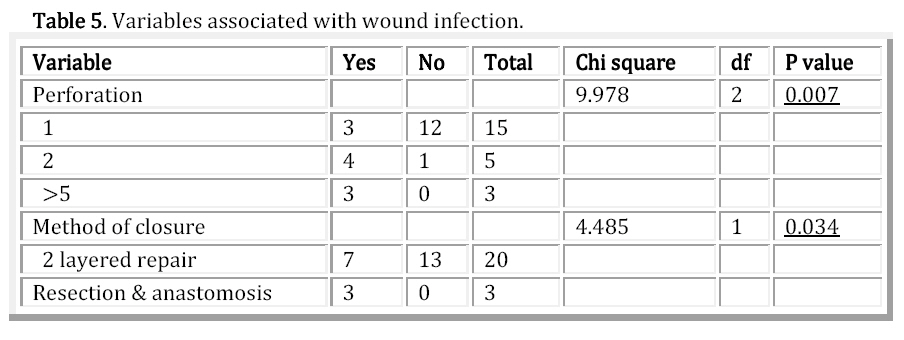
Nigeria. Introduction Typhoid fever continues to be a major health problem throughout most of the developing world. A severe complication and a frequent cause for death from typhoid is perforation of ileal ulcerations, which leads to generalized peritonitis, septicemia, fluid and electrolyte derangements, and ultimately a threat to the patient’s life. The incidence of perforation varies considerably, with the West African sub region having one of the highest perforation rates, (15-33%), in the world1,2 Typhoid intestinal perforation is a common cause of surgical acute abdomen in our environment and has traditionally been treated with surgical plication and chloramphenicol. Several studies have shown that improved survival follows adequate resuscitation with intravenous fluids, 2-layered repair of single perforation, resection and anastomosis for multiple perforations and a combination of effective antibiotics3,4,5. While mortality in the developed world has dropped to between 0%and 2%6,7, mortality in the developing world remains high at between 9% and 22%3,4,8,9. This prospective study was aimed at determining the prognostic factors in typhoid intestinal perforation in Sagamu, Southwestern Nigeria, and to compare our findings with results from other parts of the world. It is hoped that the identification of these factors will help in policy decision making, prioritizing management and improving the quality of care in typhoid intestinal perforation. Patients and Methods A total of 23 consecutive patients aged 18 years and over with typhoid intestinal perforations had laparotomy at the general surgical department of Olabisi Onabanjo University Teaching Hospital Sagamu between January 2006 and December 2008. Sagamu is suburban and is located about 40 kilometers east of Lagos, Nigeria’s commercial capital. The hospital policy provided care, including surgery, without the mandatory admission deposit during the first 48hours of an emergency admission. Diagnosis was mainly clinical, supplemented by intraoperative findings of oval perforation on the antimesenteric border of the ileum and an acutely inflamed and edematous terminal ileum. Peritonitis was recorded as general when the whole abdomen was involved; it was recorded as local when peritonitis was limited to the lower abdomen. Preoperative Care Preoperatively, all the patients had intravenous fluids to correct fluid and electrolyte deficits; nasogastric suction; urethral catheterization and broad-spectrum antibiotic coverage. The antibiotic protocol for the study was ciprofloxacin and metronidazole for all patients. However, patients who were on ciprofloxacin prior to presentation to our hospital received ceftriaxone in place of ciprofloxacin. Anemic patients had blood transfusion. Relevant preoperative investigations included packed cell volume, serum electrolytes, urea and creatinine; chest and abdominal radiographs to detect air under the diaphragm. They had pre-operative anaesthetic assessment using the American Society of Anesthetists classification (Table 1). A major drawback of the ASA system is assessment of a patient’s “correct” ASA classification by different anaesthetists. To minimize this variability in our study, the assignation of ASA class was performed by one consultant anaesthetist adhering strictly to criteria in Table 1. Surgical treatment The patients had exploratory laparotomy under general anesthesia with endotracheal intubation via long lower-midline incisions as soon as resuscitation was considered adequate. Patients in American society of Anesthesiologists (ASA) class VE were operated upon under local anaesthesia, intravenous ketamine and diazepam. Operative findings were noted. In patients with single perforation, the edge of the intestinal perforation was excised, and double-layer closure was done with chromic catgut or coated vicryl 2/0. Patients with multiple perforations had bowel resection and anastomosis. Copious peritoneal lavage was done with warm isotonic saline, 2 drains were placed, one in the pelvis, the other in the right paracolic gutter, and mass closure of the abdomen was done using nylon-1. The skin was closed with interrupted stitches of nylon-2/0. Postoperative care The postoperative outcome was monitored; patients in ASA classes IV and V were admitted into intensive care unit after surgery. Data on each patient were entered into a pro forma prepared for the study. The study variables were age and sex, type of peritonitis, number of perforations, antibiotics used, ASA classification, and method of closure. The main outcome measure was mortality. Other outcome measures were postoperative complications. The ages were in groups of 5years. Statistical analysis All data were analyzed using the SPSS statistics software for windows version 17. Pearson’s chi square test was used to determine the influence of the study variables on the outcome factors. The variables were also analyzed for their influence on complications. The differences were taken as significant only if the P value is<0.05. The study was approved by the Ethics Review Committee of the hospital. Results There were 13 males and 10 females; the male: female ratio was 1.3:1. Their ages ranged from 19 to 51 years with 17 (73.9%) being aged between 20 and 34years.The age distribution in relation to mortality is shown in Figure 1. All the patients were on antibiotics prior to presentation at our hospital. Thirteen patients were on chloramphenicol, 6 patients were on ciprofloxacin and 4 patients were on ampicillin. Following admission at our hospital, the 6(26.1%) patients that were on ciprofloxacillin had the antibiotic changed to ceftriaxone (Rocephin). The remaining 17(73.9%) patients had ciprofloxacin. Generalized peritonitis was present in eighteen (78.3%) patients, 5 (21.7%) patients had peritonitis limited to the lower abdomen (localized). Nine patients had laparotomy within 12hours of admission; the remaining fourteen patients had laparotomy within 24hours. Single perforation was found in fifteen (65.2%) patients, 2 perforations in 5 patients (21.7%). In the remaining 3 patients, 6, 6, and 7 perforations respectively were found. In 15 cases with single and 5 cases with double perforations, closure was in 2 layers with chromic catgut or vicryl suture. Resection and anastomosis was carried out in the 3 patients with multiple perforations. Six (26.1%) patients were ASA class II, 12(52.2%) were ASA class III, 3 (13%) were ASA class IV and 2(8.7%) patients were ASA class V. Two (8.7%) patients, one each from ASA class IV and V, died 1st and 2nd postoperative day. Mortality was significantly associated with ASA class (P= 0.04) Table 2. Other variables associated with prognosis are shown in Table 3. The characteristics of the patients in ASA classes IV and V, including the 2 patients that died are shown in Table 4. The 2 patients that died had single perforations and received ciprofloxacin. The ASA classification was significantly influenced by severity of peritonitis (chi square 9.775, df =3, P=0.021) (Figure 2). Complications were found in 11(47.8%) patients. Ten (43.5%) developed wound infection and one had an enterocutaneous (faecal) fistula. Wound infection was significantly associated with number of perforations (chi square= 9.978, df=2, P=0.007), and mode of closure of perforation (chi square=4.485, df=1, P=0.034) (Table 5). Discussion This study has shown that mortality in typhoid perforation is significantly associated with ASA classification and that ASA class is significantly influenced by severity of peritonitis. The preponderance of males in this study is in agreement with male predominance in other series. Typhoid perforation is a disease common in the young productive age group, 83% of our patients were aged less than 35years. This age and sex distribution is comparable to reports by other authors.8,9,10,11. In the developing world mortality rates from typhoid perforation range from 9-22% 3,4,8,9. The mortality rate of 8.7% in this study is comparable to the rates reported from tropical countries such as 8% from Ghana3, 6.8% from Nepal, 12 and 10.5% from India13. This rate is however lower than 22% from Ibadan, Nigeria8 and 15.1% from Kano4 where chloramphenicol is still the drug of first choice. However, mortality rates of 1.5-2% have been reported from some parts of the developed world, where socioeconomic infrastructures are well developed 6,7. Certain steps taken for all patients in this study might be responsible for the favorable outcome. All patients had surgery within 24 hours of admission as a result of hospital policy which provided care, including surgery during the first 48 hours of an emergency admission, without the mandatory deposit. Survival had been shown to be better in patients operated upon within 24 hours4. Secondly effective antibiotics (ciprofloxacin or ceftriaxone in addition to metronidazole) were used. The choice of antibiotic was based on local experience as an earlier report from this centre14 identified in some patients salmonella organisms that were resistant to chloramphenicol. Ciprofloxacin is the drug of first choice in the treatment of typhoid intestinal perforation in our centre. All our patients were on antibiotics prior to admission and these antibiotics included chloramphenicol, ampicillin and ciprofloxacin. Those patients on ciprofloxacin prior to perforation had the antibiotic changed to ceftriaxone because of the risk that the salmonella organisms in this group might be resistant to ciprofloxacin. In this study while no mortality was recorded in 6 patients who had ceftriaxone, 2 out of 17 patients that had ciprofloxacin died. This difference was however not statistically significant (p=0.38) and suggests that the practice be retained. Mortality was reduced from 31% to 8% in Ghana 3, with more effective antibiotic coverage and 2-layered closure of single perforation. In this study 20 cases had 2-layered repair whilst 3 patients had bowel resection and anastomosis. There was no significant association between method of closure and mortality. (p=0.57). Data from Cologne, Germany15 covering a total of 6301 general and vascular surgery operations identified significant correlation between specific intra- and postoperative variables and ASA classification. Intraoperative blood loss, duration of intensive care stay and and in-hospital mortality showed a 20 -180 fold difference between ASA I and IV, and an average of 3.7 fold difference between ASA III and IV. In this study there was significant association between ASA classification and mortality (chi square=8.31, df=3, p=0.040). The two deaths were from ASA classes IV and V (one per class). ASA classes IV and V refer to patients with systemic disease that is life-threatening. While intestinal perforation is a local disease, the ensuing peritonitis, septicemia, fluid and electrolyte derangements constitute systemic disease that threatens life. Severe peritonitis results in severe systemic disturbance and threat to life. In this study ASA classification and severity of peritonitis were also strongly associated (p=0.021). Peritonitis gets worse as the perforation- surgery interval is prolonged. The two components that make up the perforation- surgery interval are pre-hospital and admission surgery intervals. In this study all patients had surgery, after adequate resuscitation, and within 24hours. Further reduction in perforation – surgery interval requires reduction in perforation- admission interval. Improvement in health infrastructure, such as national health insurance, (which eliminates direct payment for cost of health care by individuals) is a measure that may achieve this. Mortality in moribund patients can also be improved by adequate resuscitation, which may be difficult in such patients, appropriate choice of anaesthesia, prompt and appropriate surgical intervention and post operative intensive care. In this study one out of the two moribund patients (ASA V) survived probably due to the attention paid to some of these factors. This study showed no significant association between mortality on the one hand and age, sex, number of perforations, choice of antibiotics, and method of closure on the other. Wound infection was the main complication, found in 10(43.5%) patients. This rate is comparable to 37% and 20% reported from Kano4 andTurkey5 respectively. Wound infection was strongly associated with number of perforations (chi square =9.98, df =2, p=0.007) and method of closure (chi square=4.49, df=1, p=0.034). One patient had a fecal fistula which healed with conservative treatment. No case of burst abdomen or intra abdominal abscess was recorded in this series. Aziz Sümer et al5 in their report from Turkey also found no case of burst abdomen or intra abdominal abscess. Conclusion This study has shown that ASA class is a significant predictor of mortality in patients treated for typhoid ileal perforation in our center and that severity of peritonitis is strongly associated with ASA class. Improvement in socioeconomic infrastructure and national health insurance by providing better access to health care facilities may shorten perforation surgery interval and consequently the severity of peritonitis. Improvement in severity of peritonitis may translate into improved ASA class and improved survival. Patients in ASA IV and V should have appropriate anaesthesia as well as post operative intensive care since all the deaths were from this group References
Copyright 2011 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js11032t3.jpg] [js11032t5.jpg] [js11032t4.jpg] [js11032t2.jpg] [js11032f1.jpg] [js11032f2.jpg] [js11032t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}