 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 16, No. 2, July/August, 2011, pp. 87-96 Outcome of SIGN Nail Initiative in Treatment of Long Bone Fractures in Addis Ababa, Ethiopia E. Ahmed Addis Ababa University, Medical faculty, Orthopedic surgeon, Addis Ababa, Ethiopia, E-mail: ahmedelias11@yahoo.com Code Number: js11034 Background: Currently the standard of
treatment for femoral shaft fracture and unstable tibia fracture are closed
locking intramedullary nail which require fluoroscopy and fracture table. The
objective of this review was to evaluate the outcome of Surgical Implant Generation
Network (SIGN ) initiative, locking
intramedullary nailing that do not require fluoroscopy and fracture table, in
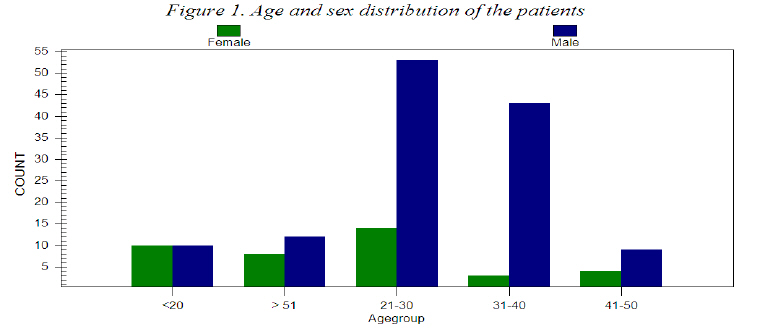
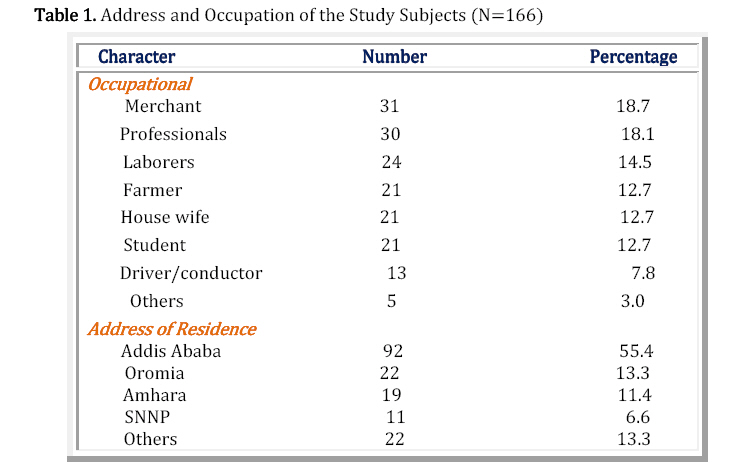
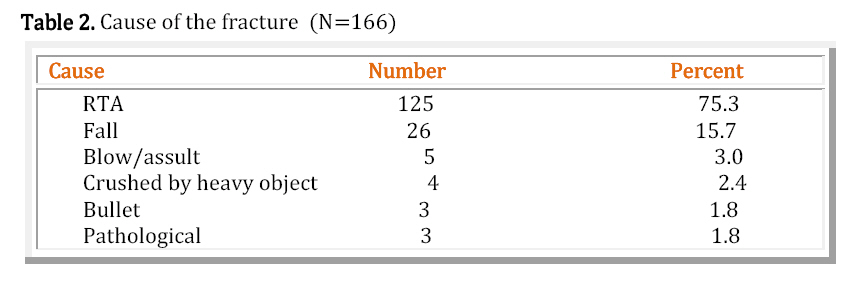
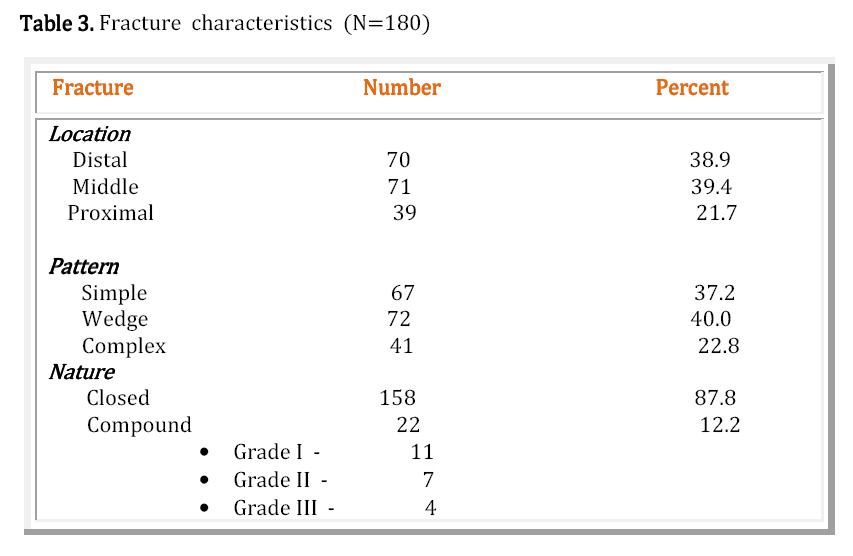
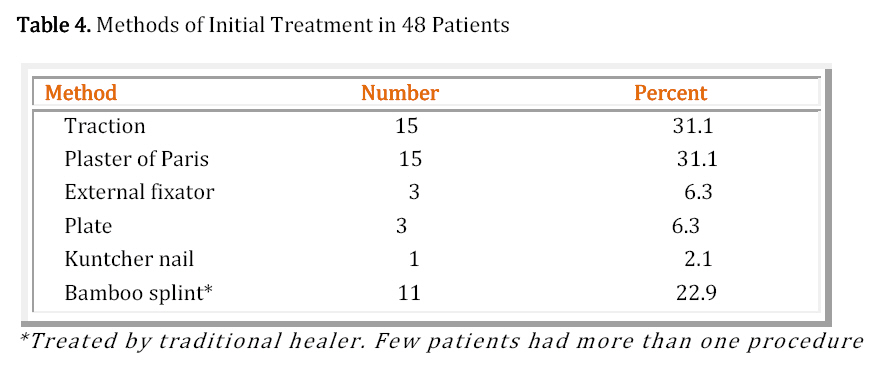
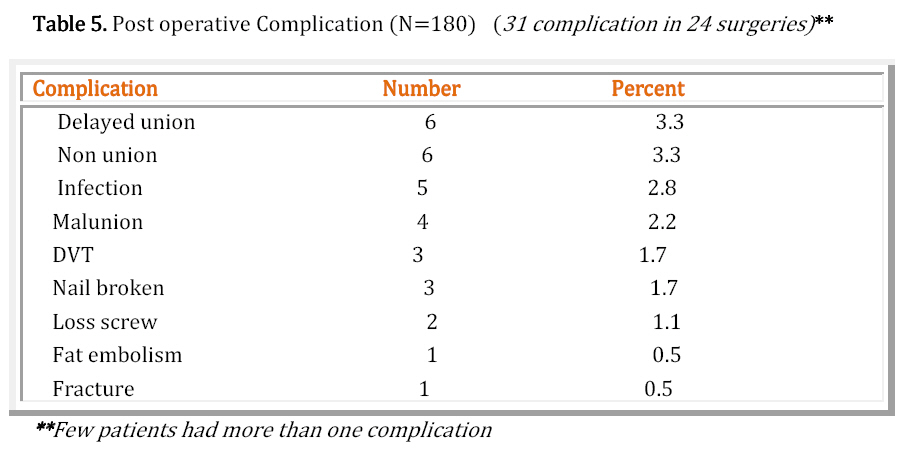
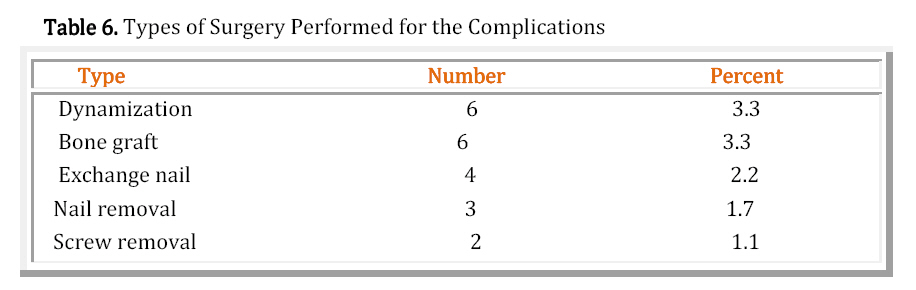
Ethiopia. Introduction Each year around 20-50 million people are injured in road traffic accidents (1). Developing countries account for ninety percent of these injuries (2-4). Long bone fractures occur in majority of these severe injuries. Traction has been traditional method of treatment of femoral fracture but this method was proved to have high rate of malunion and knee stiffness (5, 6). Even though the advent of plate fixation resolves the above problems, it had higher complications like infection, nonunion and plate failure. Advances in internal fixation of fractures include better implant design and manufacturing such as closed kuntscher nailing. These changes have resulted in improved results and fewer complications like shortening and rotation (7, 8). The development of intramedullary nail with holes for screw fixation solves the remaining problems (9, 10). Currently closed locking femoral nail is the standard of treatment for femoral shaft fracture but it is technically demanding, and requires fluoroscopy and fracture table (11-15). It is also preferred method for most displaced and unstable tibial fracture (16-19). Road traffic accident is the leading cause of injury in Ethiopia, resulted in large number of severe injuries involving tibial and femoral fractures20-23. Zonal and most regional hospitals of Ethiopia, who treats most of the injured patients, have no adequate facility to treat this orthopedic patient. Most of these patients are usually referred to central referral hospital like Black lion and St. Paul. Like other developing countries; even in central referral hospitals, usually uses conservative (non-operative) management for fractures which in turn resulted in lack of operating time and a shortage of the necessary often relatively sophisticated implants and instruments24,25. Since January 2008, it has become possible to achieve interlocking nail insertion in Ethiopia, because of SIGN (Surgical Implant Generation Network), Richland, WA, USA, who has provided us with training and equipment, inter locking intramedullary nails with interlocking screws (Sign nails) which do not require image intensifier and fracture table26. The objective of this study was to determine or evaluate the out come of SIGN interlocking intramedullary nail introduction or initiative in Ethiopia. Paying particular attention to the types of fracture which can be managed by this method, and possible complication. Patients and Methods This is a Prospective descriptive analytical study of all patients older than 12 years, who presented to any of the three hospitals (Black lion, Saint Paul and Yordanos) with femoral and/or unstable tibial fracture and treated using Sign nail from January 2008 to January 2010. All patients had given informed consent to be included. The surgical technique was as manufacturer’s manual with minor modification. In all cases open reduction and hand ream was used and the fractures were statically locked with at least one screw proximally and distally. All cases received antibiotic (Ceftriaxon) as a prophylactic for closed fracture and as treatment for open ones. The degrees of comminution on pre operative X-ray were confirmed intra-operatively because some times the degree of comminution are more than pre operative anticipation27. Standard radiograph were taken pre and post operatively. Patients were encouraged to start partial weight bearing using crutches as tolerated, starting 1st post operative day and discharged when patient condition allowed. Patients followed up every 4- 8 weeks until fracture united and rehabilitation completed or the nail was removed. Data was collected by assessing the patients before and after surgery and on follow up using a structured questionnaire which includes: sociodemographic variables; cause of injury, pattern of fracture, presence of complications, previous treatment, range of knee motion, evidence of fracture union, duration of callus formation and need of second surgery. All surgeries, patient evaluation and follow ups were done by the author. Fracture union was defined as clinically by having no pain or tenderness at the site of fracture and radiological evidence of bridging callus. Delayed union was considered if there was no callus at 16 weeks. Nonunion is defined as a fractured bone that has not completely healed within 9 months of injury and that has not shown progression toward healing over 3 consecutive months on serial radiographs28. Open fracture is classified according to Gustilo-Anderson, which is most widely used classification scheme, divided in to three as Type I: inside-out injury, minimal soft tissue injury, clean wound. II: inside-out injury, moderate soft tissue injury. III: outside-in injury, extensive muscle devitalization or major vessel injury29. Fracture pattern was classified according to Arbeitsgemeinschaft für Osteosynthesefragen (AO) which is the international association for the study of internal fixation30. The data analyzed using Epi- info 2002 software. Data were compared and statistically analyzed to identify associated factors. A p-value of less than 0.05 was taken as statistically significant. ResultsOut of 170 patients operated, 166 included in the study (four lost follow up) which gives a response rate of 97.6%. One hundred eighty surgeries were done in 166 patients (one nailing in 153 patients (92.2%), two in 12(7.2%) and three in 1 (0.6%)). One hundred and twenty seven (76.5%) were male and 39 (23.5%) female giving M: F ratio of 3:1. The mean age was 34years (Figure 1). Table 1 describes address and occupation of the patients. Blood test for Human immunodeficiency virus (HIV) was done in 116 cases and 6 (5.2%) turned out to be positive. The leading cause of the injuries was road traffic crash 125 (75.3%). Forty (24.1%) patients had more than one fractures, of which 13 (32.5%) were treated with two or more nailing particularly for 6 bilateral femur, 2 bilateral tibia, 2 ipsilateral and 2 contra lateral femur and tibia, 1 case with bilateral femur and one tibia (Table 2). Characteristics of the fractures includes; 97(53.9%) on the left side and 83 (46.1%) on the right, involving 123 (68.3%) femur and 57 (31.7%) tibia, mainly affects either mid shaft or distal in 74.8% (92/123) of femur and 86% (49/57) of tibia with unstable (wedge or complex) fracture pattern in 113 (62.8%) and 22 (12.2%) were open fracture (Table 3). At presentation 132 (73.3%) fractures were fresh and 48 (26.7%) old with malunion 28 (58.3%) or nonunion 20 (41.7%) as a result of initial treatment failure (Table 4). Seven of 123 freshly presented patients (5.3%) had early complications of fractures, 3 fat embolism, one compartment syndrome, 2 blisters, and gangrene of the fore foot in one. Concerning the technique 71 (57.7%) femoral nails were inserted in retrograde fashion and 52 (42.3%) antigrade. Bone graft was used in 37 (77.1%) of 48 old fractures. Circumferential wire was added to fix big displaced fragment in 27 (15.0%) comminuted fracture. All post-operative X-rays were satisfactory (reduced adequately and no missed hole of locking screw). Ninety percent (90%) of patients started partial weight bearing with crutches in the first two weeks and only 16 patients started late because of poly trauma and severe comminution of the fracture. Mean hospital stay was 13.8 ± 4 days, ranging from 7-30, this included the stay before surgery 4.9 ± 3.8 days (0-17) and after surgery 8.9±2.7 (4-14) days. Mean duration of follow up was 21.9 months (Range 12-36) with an average of 5 visits (range 2-10). Bone union was achieved in 7.4 weeks on average with a range of 5 to 20 weeks. Fifty-three (29.4%) nails were removed because the fracture had healed and consolidated with the mean duration of removal were 17.3 months, ranging from 7 – 30 months. Great majority of the knees had a minimum of 130 degree of flexion. Only 10 knees had less than 90 degree of flexion Twenty four patientss had post-operative complication, 5 (2.8%) had infection, 6 (3.3%) delayed union, 6 (3.3%) non-union with three (1.7%) broken nail after 20 months of its insertion, 4 (2.2%) deformity, and 3 (1.7%) deep venous thrombosis (DVT) (Table 5). There was no shortening or rotational deformity. All three DVT cases and one of fat embolism were treated medically and resolved with out sequel. Bone grafts from iliac crest was done for all the six non-union, with exchange nail for three broken nail, one re-nailing and two with already existed nail. Six delayed union cases were treated successfully with dynamization and lost screws were removed in two patients. Fracture above the nail was treated by exchanging with longer nail. Infection rate among open fractures were 13.6% (3/22) and 1.3% (2/158) for closed one. Risk of developing infection among open fractures were higher than closed (P =0.008). Two of them were present with late abscess collection (7-8 weeks after surgery), both were HIV positive. Three responded to antibiotics but in two the discharge persisted, so the nail had to be removed, debrided and fracture stabilized with external fixator and bone graft added after 8 weeks when the discharge stopped, finally one united and the other develop non union (Table 6). Unstable fracture patterns (wedge and complex) were high likely to develop post operative complication and took longer time to heal the fracture, statistically significant, p-value was 0.02 and 0.007 respectively. Duration of fracture and nailing technique were not significantly correlated with union time and complication (P>0.05). The added circumferential wire had no roll in rate of fracture healing, statistically not significant (P>0.05). Discussion Road traffic accident is a leading cause of injury accounted for 75%, predominantly affect young male (mean age 34, M:F = 3:1), which coincides with previous studies in Ethiopia and other developing countries20-24, 31-34. As a result of this and lack of facility in peripheral hospital, large number of patients with femoral and tibio-fibular fractures are presenting to central referral hospital of Addis Ababa23, even in this hospitals the availability of appropriate treatment modality was the main concern, only recently some start doing Sign interlocking nail with out fluoroscopy like other developing countries26,35,36. Due to static inter-locking nail, great majority (90%) of our patients start supported walking early which is safe37. It is interesting to compare current hospital stay of 14 days with very long hospitalization (48 and 45 days) of trauma patient in previous study of black lion24,38, mainly due to non-operative management of fractures. Shifting fracture management from non-operative to operative increases bed turn over which in turn increase availability and resolve our severe shortage of bed for trauma patients23,24. It is possible to shorten the current hospital stay by increasing operating time, which decrease the current pre operative stay of 5 days, and by provide wound care at out patient level for post operative patients. Posttraumatic infection rate of tibial and femoral fractures varies depending on the severity of the injury; our rate for open fracture was 13.6% and 1.3% for closed fractures. In developed world the average rate for open fracture is approximately 10%. (39, 40), In contrast, the infection rate following intramedullary nailing of closed fractures is approximately 1-3% 41-43. Our infection rate is almost similar with the surgeries done under ideal situation, except a little bit higher infection rate among open fractures, probably due to delayed wound care, debridement and wound closure which was done during fracture fixation after 48 of the injury. Most of our post operative complications such as DVT, nail breakage, deformity and infection, could have been prevented by giving anti coagulant prophylaxis for high risk patients, early detection and management of non union, delay weight beating for unstable sub-trochanteric and distal tibial fractures, and proper wound care for open fractures respectively. High follow up rate (98%) was due to our patients’ behavior that they do not like having implant inside the body, so they keep on coming and requesting for implant removal. Fifty-three (29%) nails were removed in healed fracture on patients request after an average of 17 months (range 7-30). Bone union was achieved in 7.4 weeks both clinically and radiologically with the union rate of 93.3%. The union rate of medulary nails treatment in developed world is the same (range between 90-100%) with our result but healing is faster44-46. Only 5% of the patient had knee stiffness (flexion less than 90 degree); almost all were patients operated for old fracture who presented with similar finding but there is no statistical difference in development of other complications and duration of healing as compared with fresh fractures. Adding circumferential wire had no significant effect in rate of union but had better patient satisfaction because of alignment of the fragment on X-ray. As it was shown in other studies, there was no significance correlation between nailing techniques and union time, as well as between complication and nailing technique47,48. The complication is few and mild, which is almost similar with closed nailing surgeries under ideal situation. It has also the advantage of eliminating the harmful effect of radiation from fluoroscopy and reduce the price to the patients as compared with other nails49. The study in Cambodia showed that even cost wise SIGN nail is more cost effective than traction for femoral shaft fracture50. Therefore I can concluded that, SIGN nail shows excellent results, with minimal complication rates which significantly improves our fracture care by reducing the complication; shorten hospital stay, early patient mobility, and patient return to function early. Recommendations It is recommend that:
Acknowledgement The cooperation of the Orthopaedic department is greatly appreciated. Special thanks go to Lewis Zerkle and Toreston Jacobson for providing us the SIGN nail and instrument. References
Copyright 2011 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js11034t3.jpg] [js11034t1.jpg] [js11034t2.jpg] [js11034f1.jpg] [js11034t4.jpg] [js11034t6.jpg] [js11034t5.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}