 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 16, No. 2, July/August, 2011, pp. 97-101 Boda Boda Injuries in Gulu Regional Hospital, Northern Uganda. D.L. Kitara Gulu University, Faculty of Medicine, Department of Surgery, P.O Box 166, Gulu, Uganda. Email: klagoro@yahoo.co.uk Code Number: js11035 Background: Trauma is the commonest indication for surgical admission
in Gulu Hospital in Northern Uganda. The situation was made worst by the conflict
between the government of Uganda and the LRA. As and when the guns fell silent,
the Boda-boda motocycles brought another form of trauma epidemic. These
injuries contributed significantly to the number of road traffic crashes seen
in Gulu, significantly affecting the health budget and health workers' time.
This study was aimed at determining the frequency and pattern of injuries
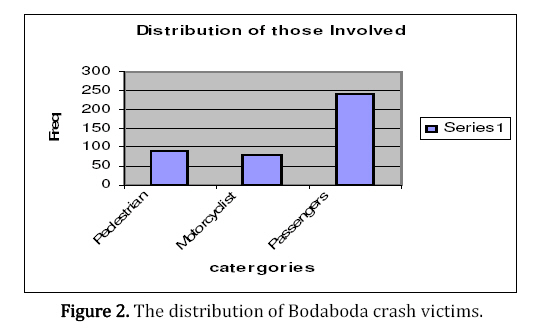
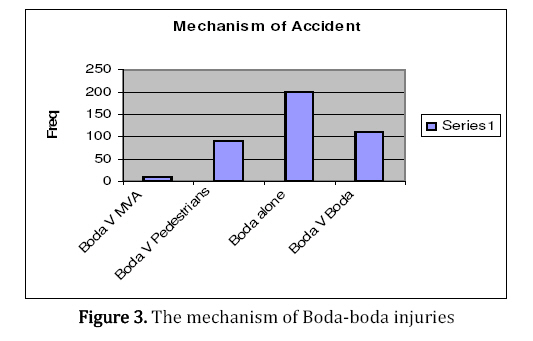
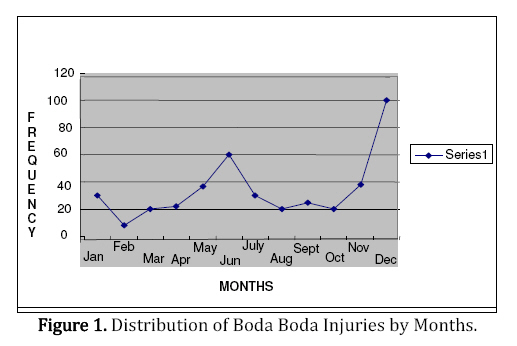
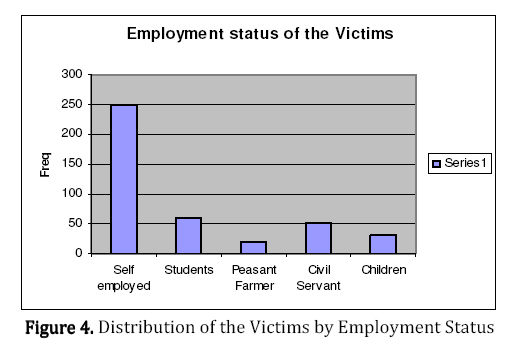
associated with Boda-boda crashes in Gulu. Introduction Road traffic injuries is one of the leading causes of death and disability world wide, and therefore an essential part of primary health care1,2. While for a long time road traffic crashes have been the leading causes of permanent disability and mortality among those aged between 10 to 50 years in the developed countries, the same picture is unfolding in the developing countries as they undergo the epidemiology of transition3,4,5,6,7 .The “Boda-boda” is a cheap means of transport on a small motorcycle with an engine capacity of 50-80cc. It's the cheapest means of transport, easy to navigate in the usually devastating traffic jams in the developing countries4,5,6,10,13. They are a quick means of transport especially for short distances in the cities and towns7,8,9,13. Most riders are not trained in road traffic and safety precautions and are usually young males who are schhool drop outs and are trying to make a living. Boda bodas are efficient in mitigating bad road delays or rash hours in most cities and towns. They are available throughout the day and night and can be riden even in small village paths which are not accessible by other quick means of transport13,14 They are a source of livelihood for the operators and the owners as highlighted by a study conducted by Naddumba in Uganda. They are now a serious health problem in northern Uganda and have contributed significantly to the increase of the disease burden. The numbers of boda-boda have increased over the years. Regulation of the riders by way of licensing and the punishment of the traffic offences are mostly poorly implemented. Boda-boda are mostly licensed to carry one passenger but it is not uncommon to find three, four or even five passengers on the same motor bike plus a cargo tide behind the motorcycle making it overloaded and difficult to navigate in our bad roads13,14 Methods This was a retrospective study conducted in the Gulu Regional Hospital surgical ward over a period of two years. A total of 410 patients with Boda-boda injuries were admitted to the surgical ward over the period. Their medical records were retrieved, compiled and analyzed. The data collected focused on the mechanism of injury, sex, the victim, and the period when the injury occurred. The research and ethical review board's approval was obtained from Gulu Hospital. Results A total of 410 patients with various forms of Boda-boda injuries were seen in the surgical ward of Gulu Regional Referral Hospital during the study period. The peak was in December followed by June of each year which represented the highest and second highest incidences of Boda-boda injuries. The lowest number occurred in February. During the study period, there were 454 (24.1%) cases of assault (Gender related violence), followed by 410 (21.8%) “Bodaboda” crash injuries, 137 (7.3%) gunshot Wounds (GSWs) and 110 (6.3%) burns. Among other causes of trauma were falls from trees and animal bites. More males (57.5%) were involved in Boda boda crashes than females (42.5%) with a male to female ratio of 1.4:1.0 Of the 410 Boda boda victims, 250 (61.0%) were passengers, 85 (20.7%) were pedestrians and only 75 (18.3%) were the motorcyclists themselves (Figure 2). The majority of cases were Boda-boda crashed alone, followed by boda colliding with another Bodaboda, then boda smashing into pedestrian and last boda-boda crashing with a motorvehicle (MVA) (Figure 3). Most (61%) of the injured were self-employed with 250 cases followed by (14.6%) of them students with 60 cases, (12.2%) of them civil servants with 50 cases, (7.3%) of them children with 30 cases and last (4.9%) were civil servants with 20 cases. Discussion Boda-boda injuries admitted in Gulu Regional Hospital were the second commonest cause of physical injury after Gender based violence. Males were more involved than the females and most of those involved were self-employed persons. The Boda-boda motorcyclists tend to over-speed and over-load the motorcycles for quick financial returns12,13,14,15. It is probably because of that reckless, indiscipline and lack of respect for other road users by the motorcyclists who were mainly youths and drop-outs from school as a possible major cause of those accidents and injuries13,14,15. The self-employed and the students were the most injured because of the rushes for businesses and travels to schools respectively. December had the highest number of cases recorded. This was probably because most of the people from Gulu district who live in other districts and diaspora come back to Gulu to celebrate the festive season. This was usually accompanied with massive celebrations and merry making, frequent movements from the villages to the town and massive drinking of alcohol. It should be noted that during this month, the students were also back at home on holidays. Regular movements from the town to the villages for the revelers and misuse of motorcycles have also been reported. It was in this process that many got involved in Boda-boda accidents because of the movement under the influence of alcohol and frequent use of the motorcycle by unlicensed persons14,15. The increases in the number of road traffic crashes are not new, similar incidences were recorded in Tanzania4,6,8,9,10. There were a large number of pedestrians who constituted the largest number of the injured and the dead 11,12. Although disturbing, this incident has been reported in many developing countries11,12. Public awareness on road use is fairly low and pedestrians are less likely to use the walking pavements even when they are available8,11. The month of February had the least number of Boda-boda injuries. This was probably because, most people who had come home to celebrate the festive season would have returned to their respective destinations and the pupils and the students would have returned to their respectively boarding schools. Also about the same time most of the people had little money because of overspending during the merry making festivities as well as payment of school fees. Farmers became busy because of preparing their fields for the next planting session. This finding could be explained further by the fact that, there was usually a reduced number of “Boda-boda” riders and activities of the motorcyclists in the area. The students who usually form the bulk of the Boda-boda riders would have returned to school and therefore the sudden reduction in the numbers of the injuries. The males formed the majority of the cases of injuries recorded in the 2 years. This was mainly because nearly all Boda-boda riders were males. Females on the other hand registered a lower number of cases 42.5% and most of them were either passengers or pedestrians. The commonest mechanism of injury was a Boda-boda rider crashing after failing to control his motorbike, followed by Boda-boda and another, then Boda-boda with a pedestrian and finally and the least common is between a Boda-boda and a motor vehicle. This generally reflected the quality of Boda-boda riders who were generally ill-trained and lacked the basic skills of handling the machine and most of them did not undergo any formal training program for riding12,13,14,15. Most of the Boda-boda riders in Gulu as reported by the Central police station of Gulu did not even have a riding permit (Road License to ride a motorbike) as provided for in the Road and Safety Act of Uganda and no specific efforts were being put forward to address this particular problem. Conclusion and Recommendation Bodaboda crashes are a major cause of physical injuries in Gulu Hospital. Passangers are the commonest victims of the crashes. It is a major public health problem that requires the attention of policy makers in the post conflict region of Gulu. Proper training and licencing of boda boder riders and imposition of strict discipline among boda boda riders, surveillance and enforcement of the Road traffic and safety Act will go a long way in reducing boda boda injuries. References
Copyright 2011 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js11035f4.jpg] [js11035f1.jpg] [js11035f2.jpg] [js11035f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}