 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 16, No. 2, July/August, 2011, pp. 102-111 Surgical Volumes at the District Hospital: A Retrospective Review of National Data in Rwanda R.T. Petroze1,2, A. Nzayisenga2,3, J.F. Calland1, G. Ntakiyiruta3 1University of Virginia Healthsystem,
Charlottesville, VA Code Number: js11036 Background: Surgical conditions are a
significant contributor to global morbidity and mortality, and much of the
burden of surgical disease arises in resource-limited settings. There are profound disparities in surgical
care worldwide, with only 3.5% of surgical procedures estimated to be performed
in the poorest 1/3 of countries. Yet,
very little is known regarding the true volume of surgical procedures performed
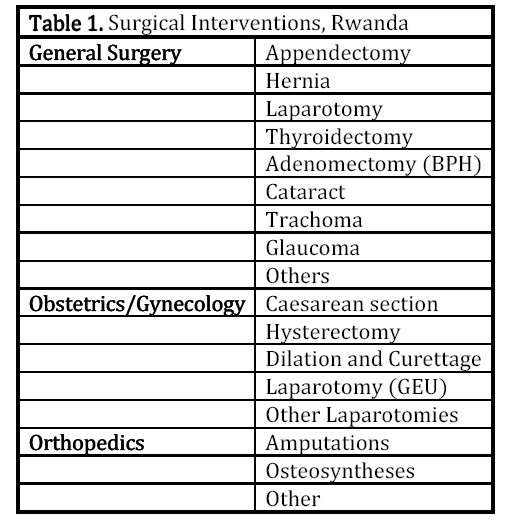
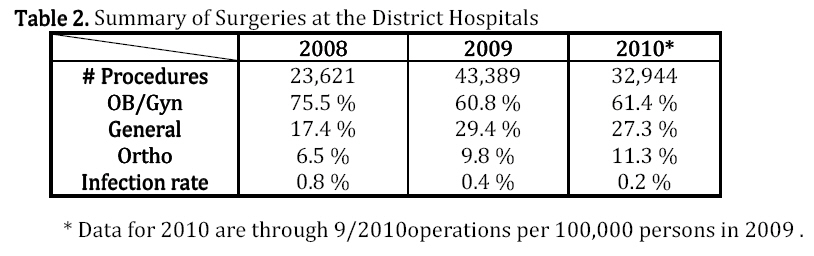
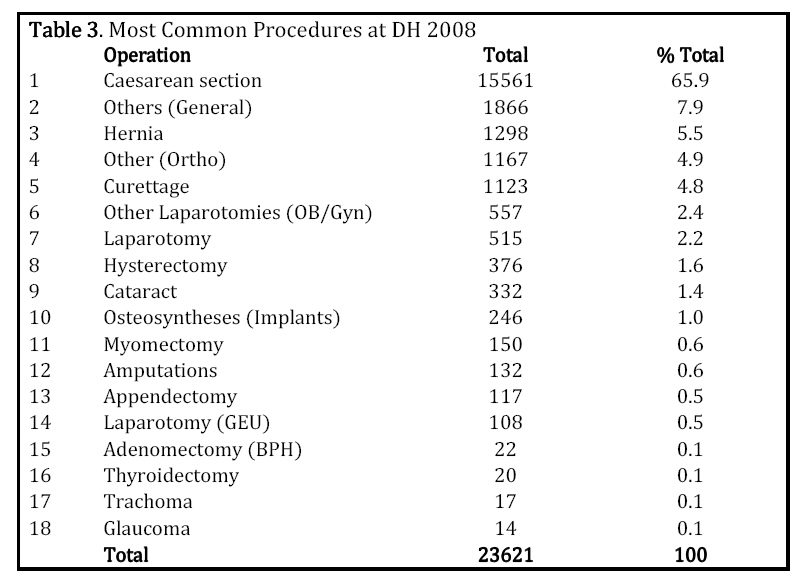
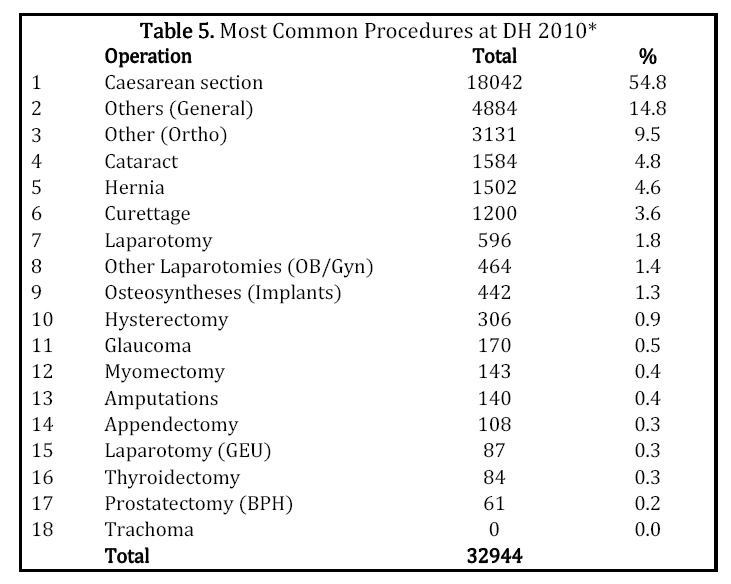
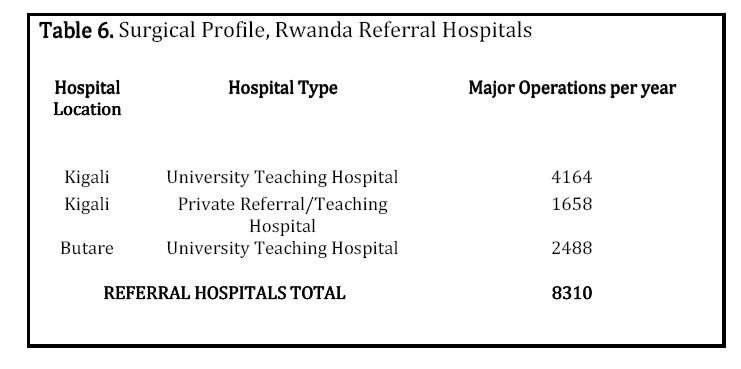
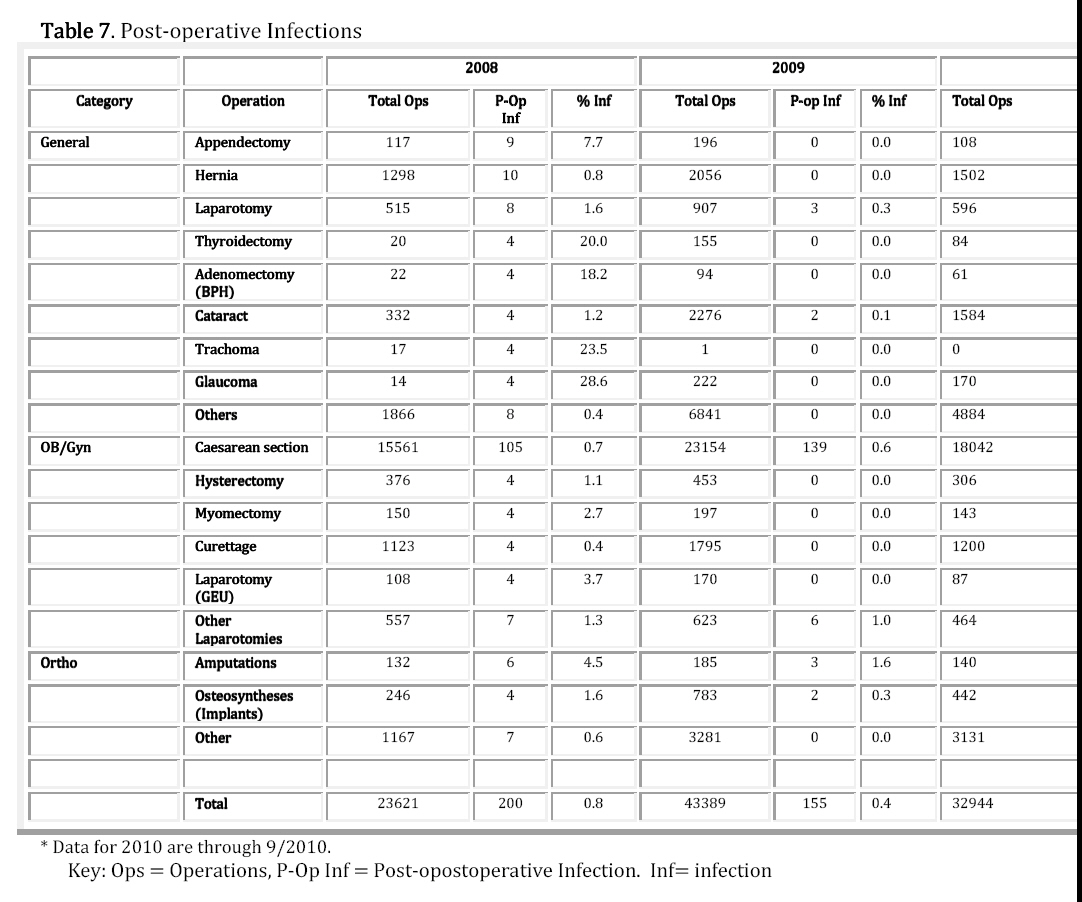
in resource-limited settings. Introduction Surgical conditions are conservatively estimated to contribute to 11% of the world's disability-adjusted life-years (DALYs), a quantitative measure of disease-related morbidity and mortality. Defining the true global burden of surgical disease is, however, a challenge based on limited data in many parts of the world1,2. Using available surgical data from World Health Organization (WHO) member states, Weiser and colleagues created a predictive, statistical model, estimating that 234 million surgical procedures are performed worldwide each year3. Disparities in global surgical care are profound, with only 3.5% of those surgical procedures being performed in the poorest 1/3 of countries, and 90% of injury deaths occurring in low-income countries3,4. Much of the missing surgical data comes from such resource-limited settings. This is not surprising as access to surgical care is severely limited by provider scarcity. Africa, for example, has only 1% of the surgeons America has, a number that is clearly insufficient to meet the surgical needs of the continent5,6. Until recently, the international public health and international surgical communities have not regarded access to surgical care, particularly emergency and essential surgical care, as a clinical, funding, training and research priority. Recognizing this need, efforts to increase surgical capacity have begun, often through collaborations with local government, regional societies, and international partners. Yet, knowing what types of procedures are performed is important for safety, training, resource allocation, and quality assessment. To date, very little has been published regarding the true volume of surgical procedures performed in resource-limited settings. Rwanda is a land-locked country in East Africa with a population of over 10 million people and a population density of 368 inhabitants per square kilometer. The Rwandan health system was devastated by the violence of the 1990s, and despite tremendous progress in the health sector, there is still a scarcity of physicians, with approximately one doctor per 33,000 population7,8. Access to surgical care is increasingly being recognized as a health priority in Rwanda, but the needs have yet to be systematically evaluated. Methods We conducted a retrospective, descriptive study of aggregate district hospital statistics in Rwanda from January 2008 to September 2010. Data was extracted by theatre staff at each hospital from the handwritten surgical registers and placed into a monthly hospital reporting form. Monthly data was then entered electronically by a trained hospital data manager to the national level via the HMIS database, GESIS SQL server database. The categories of information collected had been previously set by the Ministry of Health; specific procedures are quantified in general surgery, obstetrics/gynecology, and orthopedics, as detailed in Table 1, as well as reported post-operative infections. Only operations performed in the main operating theatre are delineated as major operations, and thus, we have not analyzed outpatient or minor procedures. There are 42 district hospitals and 3 designated referral hospitals in Rwanda. The aggregate District Hospital data is from 40 district hospitals. The psychiatric hospital and the new police/maternity hospital were excluded due to lack of surgical data. Data was missing or incomplete for 8/40 hospitals in 2008 and therefore excluded. Referral hospital data is not centrally recorded in the MOH database and was therefore extracted from the hospital statistics department for comparison. 2009 data is reported for the university hospital in Butare and 2010 data for the university teaching hospital and private referral hospital in Kigali. Results A significant number of procedures are occurring at the District Hospital level in Rwanda, the majority of which are caesarean sections in obstetrics and gynecology. Table 2 provides a breakdown of the number of recorded procedures performed each year and the percentage in each pre-defined category. A total of 23,621 procedures were performed in 2008 at the District Hospital level in Rwanda. Table 3 lists the breakdown of procedures at the District Hospital in 2008. 66% percent of all operations performed were caesarean sections. 43,389 procedures were performed in 2009. Table 4 details the most frequently recorded procedures in 2009. Table 5 details the results for 2010. Using the most current population projection from the Rwandan National Institute of Statistics (10,117,029 population)9, Rwandan district hospitals performed 429 major operations per 100,000 persons in 2009 . Table 6 provides a breakdown of the volume of major surgical interventions performed at the 3 referral hospitals, providing a further 82 major operations per 100,000 persons. Table 6 provides a breakdown of the volume of major surgical interventions performed at the 3 referral hospitals, providing a further 82 major operations per 100,000 persons. Reported post-operative infection rates were 0.8%, 0.4% and 0.2% for all operations for 2008, 2009 and 2010, respectively. Table 7 shows reported post-operative infections for each procedure per year. Discussion Addressing the global burden of surgical disease poses many challenges. One of the first challenges is defining this burden in terms of scope of disease and available treatment. Another debate arises in addressing the dearth of surgical workforce in low-and middle-income countries, with many resources being focused in the capitals or at the university-level.10 Here, we looked retrospectively at aggregate statistics provided by the district hospitals in Rwanda to the Ministry of Health. In comparison to surgical volumes at the referral and teaching hospitals in Rwanda, our study confirms that a significant number of procedures are occurring at the district hospital level, the majority of which are in obstetrics and gynecology. The majority of studies on the global volume of surgical disease in the literature have used statistical modeling to define the burden of surgical disease1,3. Surgical data in low-income countries is scarce, but there are a few studies that also look at retrospective surgical data. Galukande and colleagues conducted a retrospective review of surgical volumes in eight representative district hospitals in Uganda, Tanzania, and Mozambique. Similar to the results of our review, the breadth of surgical procedures performed was narrow, and obstetric procedures were by far the most common procedures performed. Hernias and wound care procedures were the most common general surgery procedures11. In our review, hernias comprised 5.5%, 4.7% and 4.6% of overall procedures (Tables 3, 4, 5). Wound care procedures were not specifically recorded, but a significant number of procedures are simply listed as “other”. It is important to note that our study does not include wound care procedures that occurred outside of a designated operating theatre (in a treatment room, for example). The dramatic increase in total procedures from 2008-2009, as detailed in Table 2, is likely due to under-reporting (8 hospitals were excluded in 2008 due to absent or incomplete data) and the significant increase in cataract surgeries recorded after 2009, which also corresponds to the creation of an eye referral center at one of the district hospitals. Interesting, the HMIS system classifies ophthalmology procedures as general surgery, as in Table 2. The percentage of ophthalmology procedures—cataracts, trachomas, and glaucomas—performed rose from 8.8% of general surgery procedures in 2008 to 20% of general surgery procedures in 2009 and 2010. A more appropriate breakdown of surgical procedures is provided in Tables 3, 4, 5. Cesarean sections are by far the most common overall procedure performed in Rwanda at the district hospital level, comprising nearly 90% of OB/Gyn procedures and 50-65% of all procedures (Tables 3, 4, 5). The most recent overall c-section rate for in-hospital (district hospital or referral hospital) deliveries in Rwanda is 22%12. There are several points to be noted from these statistics. In the United States, caesarean sections are one of the most common operations performed but comprise only 2.5% of all surgical procedures. This is comparable to high-income nations worldwide at 2.6%, as reported to the Organization for Economic Cooperation and Development13. This may be because of greater overall surgical volume and more varied caseload. The predominance of caesarean deliveries in Rwanda may also be influenced by initiatives related to Millennium Development Goals 4 and 5 to decrease maternal and child mortality14-17. In reviewing the literature, one author further suggests that the percentage of total procedures that are caesarean sections can be a useful indicator of surgical services in resource-limited settings. He suggests that caesarean sections are often the most common procedure in resource-limited settings but as capacity increases, breadth of surgical procedures diversifies and the percentage caesareans decreases18. Based upon our review, orthopedics procedures are not well quantified at the district hospital level in Rwanda, but are noted to be on the rise. Injuries are known to account for the greatest burden of surgical disease worldwide, with road traffic accidents expected to become the 5th leading cause of death by 2030.19, 20 A retrospective study to evaluate demographics of injury at the central university referral hospital in Kigali, Rwanda in 2005 found injury rates to be high, predominantly blunt trauma due to road traffic accidents with a predominance for young males.21 Clearly, the volume of recorded orthopedic procedures at the district hospital level does not reflect the burden of orthopedic injury and needs in Rwanda. As the reporting form is set by the Ministry of Health and not by surgical caregivers, several procedures known to be a surgical burden at the rural level are not specifically recorded. These include things like circumcision, obstetric fistula repair, and emergency procedures like thoracostomy tube or burr hole. There are several limitations to this study and the available data. Firstly, post-operative infections, the only measure of complications and outcome available for surgical procedures, appear to be poorly recorded, as shown in Table 6. For example, in 2008, thyroidectomies had a 20% infection (4/20 operations), but there are no recorded infections for 2009 or 2010, despite increased volume of procedure (155 and 84, respectively). A similar pattern is seen with adenomectomies, trachomas, and glaucomas. Caesarean section infection rates, which are the most numerous, are 0.7%, 0.6% and 0.3% for 2008, 2009, and 2010, respectively. In addition to the need for reliable quality assurance, the overall low reported infection rates may likely be due to ineffectual reporting of complications and poor follow-up. Furthermore, while a patient may present to a district hospital for surgery, once discharged, their care returns to the local health center level, and so post-operative infections may not present to the district hospital. Complications presenting at the health center level are not currently tracked in a way that links the complication to the district hospital procedure. This study provides a good overview of the volume and breadth of surgical procedures performed at the district hospital level in Rwanda. Only the district hospital data is centrally available in the HMIS system. Here we have included overall surgical volumes from the referral hospitals for comparison, indicating a significant surgical burden at the district hospital level. Importantly, future studies should evaluate specific procedural volumes and outcomes at the central referral level, via visiting mission surgical groups and at private clinics. In order to maintain patient safety and an adequate vision of personnel and capacity resources, a future step could be the creation of a central, organized database of all surgical activities. Our study of the available data has hopefully established a baseline on which to build improved and accurate reporting of surgical procedures and complications as surgical capacity improves in Rwanda. Further information can be gathered from a prospective analysis of surgical disease in resource-limited settings using both urban—which can reflect the impact, for example, of multisystem trauma due to road traffic accidents—and rural registries where surgery is performed by general practitioners. The focus must be on outcomes and safety as capacity improves, and dynamic systems of quality assurance and quality improvement as well as accurate patient follow-up are vital at centers where surgery is performed. Furthermore, accurate knowledge of the breadth of surgical disease can help to guide material and personnel resource allocation and training in resource-limited settings. Conclusion Comparable to the global literature, the majority of procedures performed at the District Hospital level in Rwanda are caesarian sections, but proportionately more general and orthopedic procedures have been performed over the past 2 years. A substantial opportunity remains to increase surgical capacity within Rwanda, and a prospective analysis of surgical epidemiology and surgical outcomes is needed. As surgical capacity improves, accurate reporting of surgical procedures and outcomes with a robust surgical quality assurance system is imperative to planning the training of surgical caregivers, allocation of resources and ensuring patient safety. References
Copyright 2011 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js11036t5.jpg] [js11036t3.jpg] [js11036t1.jpg] [js11036t6.jpg] [js11036t7.jpg] [js11036t4.jpg] [js11036t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}