 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 16, No. 2, July/August, 2011, pp.123-129 Cerebral hydatidosis, a rare clinical entity in Ethiopian teaching hospitals: case series and literature review. G. Assefa1, H. Biluts2, M. Abebe2, M.H. Birahanu2 1Department of Radiology, 2Department of
Neurosurgery, Faculty of Medicine, Addis Ababa
University, Ethiopia Code Number: js11039 Background:
Cerebral hydatidosis (CH) is a rare disease and unlike other body organs
cerebral involvement is very uncommon and if it occurred it is often seen in
pediatric patients. The aim of the study is to show the clinical and imaging
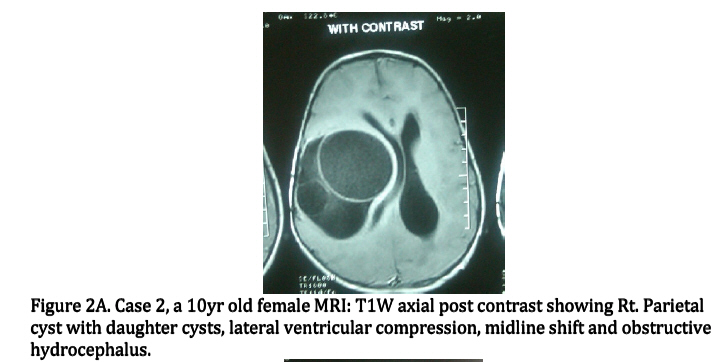
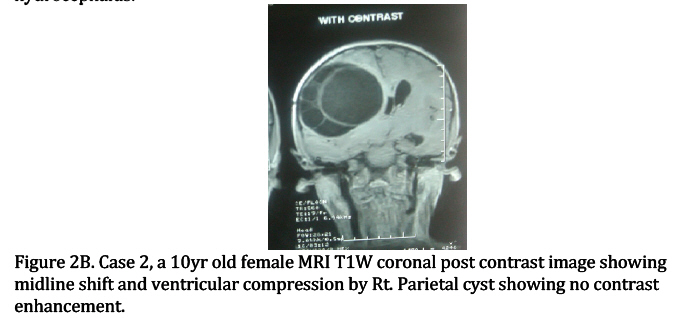
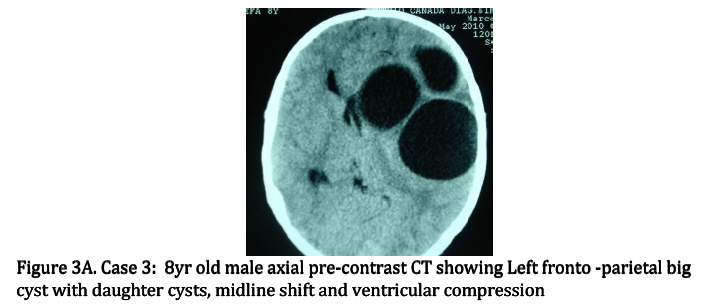
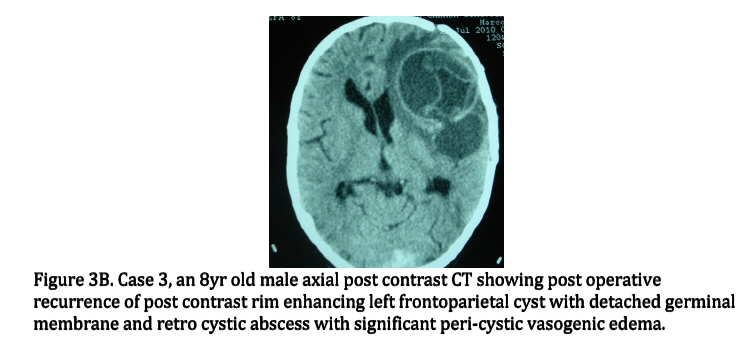
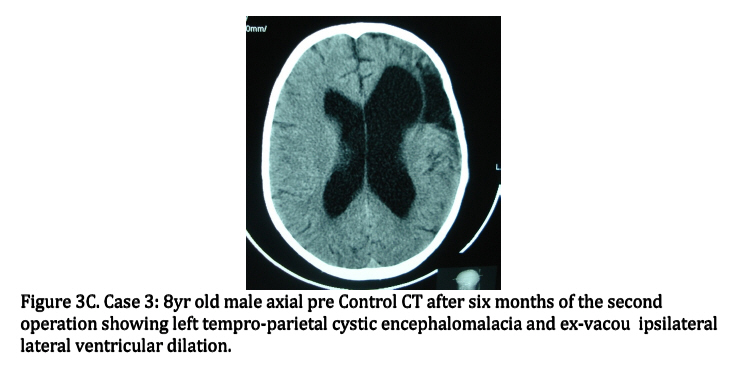
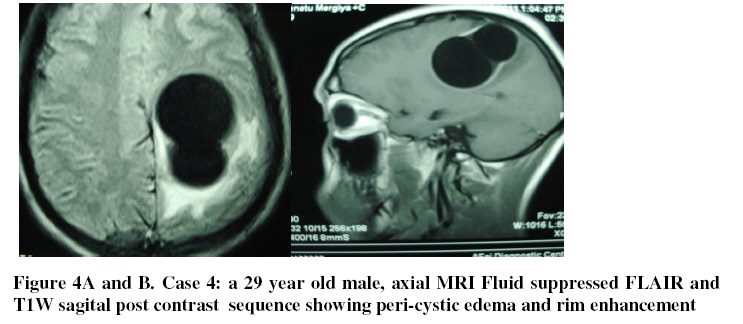
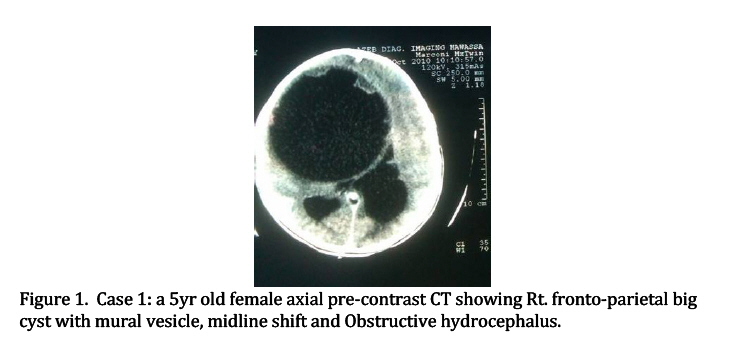
features and neurosurgical outcome of CH in East African setup. Introduction Hydatid disease is worldwide zoonosis by the larval stage of the echinococcosis tapeworm. There are two types of echinococcus infections namely Echinococcus granulosis, the more common type and Echinococcus multilocularis (alveolaris) which is the less common type but more invasive mimicking malignancy. HD continues to be a significant health problem in underdeveloped world where animal husbandry is common but no veterinary control exists. HD is not uncommon and is endemic in Ethiopian setting pausing significant health problem with significant clinical and surgical morbidity and mortality1-5. HD spares no body organs and affects from head to toe and accounts for 3-4% of intracranial lesions, and 2-3% of patients with HD have intracranial Hydatid6,7. The majority of HD involving the lungs (8.5-43%) and the liver (50-77%)6-10. CH is acquired in two different forms, a primary CH caused by embryos passing hepatic and pulmonary barriers. The primary intracranial cysts are the most common and are commonly solitary. Secondary cysts are usually multiple, which may follow embolization of ruptured traumatic or surgical cysts in other organs7,11. The treatment of cerebral Hydatid cysts is principally surgical. The primary goal of the operation is total cyst extirpation without rupture. We report four case series of surgically proven and exclusively primary CH in Ethiopian setting, which is the first of its kind with review of the literature. Patients and Methods Four cases of CH were operated in Tikur Anbessa and Zewditu teaching hospitals between 2009 and 2011. Their age, sex, clinical presentation, domicile, surgical treatment the intra operative findings, the intra and postoperative complications and six months postoperative clinical follow-ups were recorded. Contact history with pets such as dogs if available was also recorded. All the MRI and CT brain performed with and without intravenous contrast media were reviewed. The size, location and contrast enhancement feature and compression effects of the cyst were recorded. Other imaging such ultrasound of visceral organs and chest x-ray and hematological results were also noted. Results Four cases of cerebral hydatidosis (CH) were operated between 200-2001. Three of the patients were pediatric cases and included one male and two female children aged 8, 5 and 10 years respectively. The fourth case was a 29 years old male. All the three pediatric cases lived in rural South East of the country (Arsi, and Bale). The adult was raised in the same area but at the time of review was living in urban town, Dire Dawa. All had history of contact with pet animal (dogs). All of them presented with progressive hemiparesis, nausea and vomiting, and one of the pediatric patient presented with progressive visual impairment and seizure disorder. Two of the pediatric patients had both MRI and CT of the brain and the others had only brain CT. All the MRI and the CT were performed pre and post contrast. On imaging all showed single big cerebral hemispheric cyst, with three cases showing daughter cysts (Figures 2a & b, 3a, b, & c, 4) and one showing simple cyst with mural vesicle (Figure 1). The cysts measured 6x5cm at minimum and 11x11 cm maximum, all causing ipsilateral lateral ventricular compression or effacement and obstructive hydrocephalus and were located in the frontoparietal, parietal and temproparietal and middle cerebral artery circulations. In two patients (Figures 3a, b, & c, 4) there is peri-cystic contrast enhancement on both MRI and CT with pericystic vasogenic edema. And the other two showed a hypodense layered cyst wall or hypointense rim on both T1 and T2 weighted pre and post contrast images. One had eosinophilia of 10% otherwise all had normal CXR and abdominal ultrasound and CBC.The mode of treatment for all cerebral hydatidosis were craniotomy (three Frontal craniotomies and one temporal craniotomy) with the goal being complete removal without rupture. The hydatid cysts were removed unruptured in three of the cases. All had uneventful post operative course except one of the pediatric patient who developed post operative recurrence of the cerebral hydatidosis at the same location and brain abscess and leptomenigitis (Figure. 3B). He was re-operated and the cyst was removed and the abscess was drained. Control CT scan after 8 months showed extensive temproparietal gliosis with ex-vacou ventericulomegaly (Figure 3C) otherwise no residual CH. Clinically has persistent residual poor vision and seizure and he is on pediatric neurology clinic follow-up. Discussion Cerebral cystic echinococcosis commonly seen in children and young adults in 50-70% of the cases12-14 and this is compatible with our findings, and are located in the supra tentorial hemispheric region and are distributed within the territory of the middle cerebral artery and mainly in the parietal lobe and this is consistent with other reports12-15. CH are usually single and multiple cysts are rare and multiple cysts are often associated with other organs involvement15,17. Recurrent cysts due to rupture of the primary cyst during surgery is not uncommon and was seen in one of our patients who had an infected cyst which ruptured intra-operatively. Patients with CH may have HC in other organs, in recent studies hepatic, pulmonary and other locations were found in 10% of the cases18 but none of our patients had extra cranial hydatid as abdominal ultrasound and CXR were normal. Both CT and MRI demonstrate a spherical and well defined, smooth, thin walled homogenous cystic lesion with fluid density similar to the CSF with or without septation or daughter cyst and/or calcification. On CT the cyst wall is isodense or hyperdense to the brain tissue. On MRI the cyst wall shows a rim of low signal intensity on both T1 and T2 images. Enhancement of the cyst wall and pericystic edema may be seen in both CT and MRI if there is super infection, rupture or leakage of the cyst7,15 and this was seen in two of our patients. Postoperative recurrence of CH is not uncommon13,15,19 and one of which had a recurrence and postoperative complication of brain abscess. However surrounding edema and rim enhancement is usually absent in untreated or non-complicated cases and this was seen in two of our patients. Displacement of the midline and compression of the ventricles are common because of the big size of the cyst at clinical presentations and this was seen in all of our patients. The differential diagnosis of CH includes cystic lesions such as porencephalic cyst, arachnoid cyst and cystic tumors of the brain and pyogenic abscess. In contrast to Hydatid cysts porencephalic and arachnoid cysts are not spherical in shape and not surrounded entirely by brain substance. Arachnoid cysts are extra axial masses that may deform adjacent brain. Porencephalic cysts result from insults to normal brain tissue and are lined by gliotic white matter that could easily be demonstrated with MR. Cystic tumors could be differentiated by the enhancement of the mural nodule. Pyogenic abscesses show rim enhancement with surrounding extensive vasogenic edema. Cysticercosis is one of the differential diagnoses and epidemiology of the disease is helpful in the differential diagnosis and this is unlikely as it is not endemic in African setup. The clinical presentation of CH is nausea vomiting and hemi paresis with or without seizures and such presentation is almost seen in all of our patients. Complete removal of Hydatid cyst surgically through wide cranial opening (craniotomy) was the main modality of management of cerebral hydatidosis in our case series consistent with the primary goal of the operation, i.e. total extirpation of the cyst without rupture20-23. Conclusion In a country where hepatic and thoracic hydatidosis are common clinical attention should be paid for CH, and patients with thoracic and abdominal hydatidosis should be screened for CH with CT and MRI before patients are symptomatic when the size of the cyst is big enough to compress vital structures and get complicated with associated clinical and neurosurgical morbidity and mortality. And cerebral hydatidosis should be included in the differential diagnosis of intracranial and cystic space occupying mass lesions, especially in the pediatric patients, if CT and/or MRI reveal such findings. Surgery is the main treatment. The goal of surgery is to remove the cysts in Toto without rupture References
Copyright 2011 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js11039f3b.jpg] [js11039f1.jpg] [js11039f2b.jpg] [js11039f2a.jpg] [js11039f3c.jpg] [js11039f4.jpg] [js11039f3a.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}