 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 16, No. 2, July/August, 2011, pp. 130-134 Balanitis Xerotica Obliterans: An experience with Buccal Mucosa Onlay Flap Graft. M.D. Mchembe1, A. Kategile1, C.M.A. Yongolo1, K.A. Mteta2 1Department
of Surgery, Muhimbili University of Health and Allied Sciences. Code Number: js11040 Background: Balanitis Xerotic
obliterans (BXO) or Penile
Lichen Sclerosus is a dermatological condition
affecting the genitalia and associated with chronic, progressive, sclerosing
inflammatory dermatosis of unclear etiology.
It was first described by Stuhmer in 1928, as being a rare condition but
causes severe tissue destruction and often causes meatal stenosis and urethral
stricture. Our objective is to present the experience of treatment of urethral
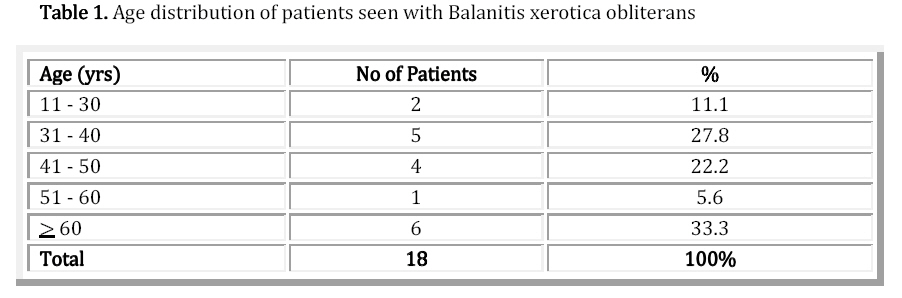
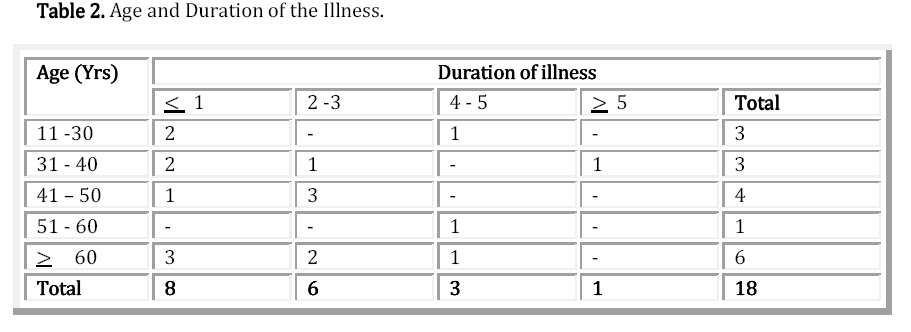
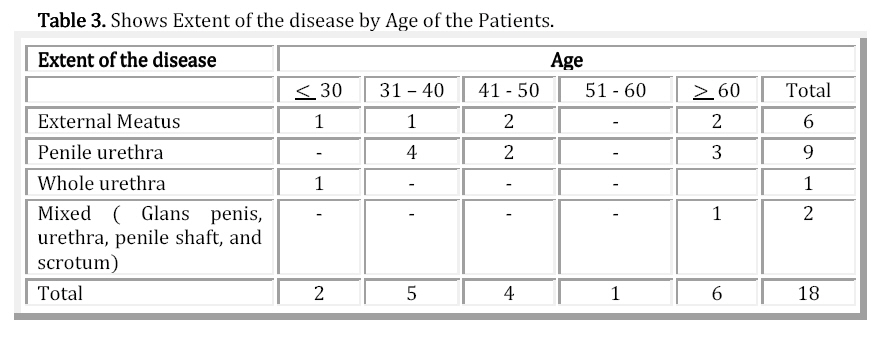
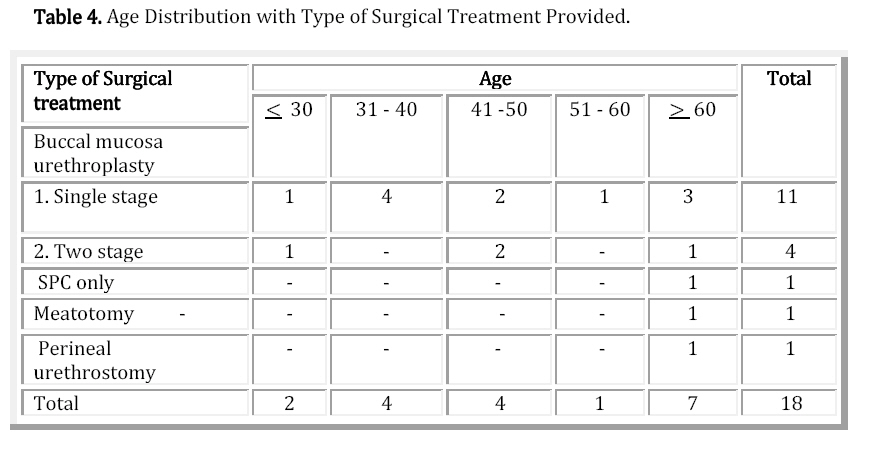
stricture caused by Balanitis Xerotic Obliterans in our hospitals. Introduction There are many causes of urethral stricture, these include inflammatory causes, tumours, traumatic causes both MTA and pelvic injuries or fall astride and iatrogenic secondary to prostatectomy (TURP) and catheterization. Occasionally the urethra can be affected by other conditions like Lichen sclerosus (BXO) and this can result into formation of urethral narrowing and strictures. BXO is a skin disease which causes severe fibrosis of the skin and has been described in both females and male genitalia 1,3,4. The skin becomes discolored having an ivory coloration. The involvement of the genitalia is of varying extents. The etiology of the disease is not clear however there are immunological causes that have been postulated but the result is severe fibrosis of the affected area1,2,3. Depending at which stage the patient presents to you for treatment, the presentation can differ from prepuce or penile glans discoloration to difficult in passing urine because of narrowing of the urethra and eventually retention of urine and its consequences of upper tract dilatation and uro-sepsis resulting to urine finding an alternative passage and presenting with multiple urethral- cutaneous fistula and sinuses2,3,4.The treatment of this condition causing stricture of the urethra is excision of the fibrotic area and urethra reconstruction which varies from different centers. We wish to present to you our experience on 18 patients who presented to us with BXO already having urethral stricture. Patients and Methods We have been maintained a record of all patients with urethral stricture presenting to our urology unit at Muhimbili and KCMC in Tanzania which are both university teaching hospitals. On the average we see three (3) new patients in a week which makes a total of 150 patients per year. Since 2003 we have seen 18 patients with urethral stricture due to BXO making it 2.2 patients per year. The patients were all not circumcised during their childhood and two of them had circumcision because of skin discoloration of BXO several months before they presented to us. The patients were aged between 17 years and 84 years old. All eighteen patients presented with poor stream of urine which have led five of them having retention of urine. Three patients came to us with Suprapubic Cystostomy in place while two patients had fistulae and sinuses that we had to place the SPC. Results The table below represents the number of patients attended with BXO, their age, presentation and the type of surgery provided for their condition. A total of 18 patients were treated for stricture caused by BXO for 5 years. Most of the patients whom we saw were late and neglected cases probably highlighting the poor health services system that we see in our country. Two patients were already circumcised due to the same condition and the other five had to be circumcised in the course of treatment of their stricture. Diversion of urine was done to five patients who had SPC and others, had no diversion made. The whole fibrotic strictured area was removed and buccal mucosa was placed in five on the same sitting with closure and repair of the urethra while in one patient excision was done followed by two months of dressing before clearing the infection and a two stage buccal mucosa on lay was performed. In one patient during follow up the meatus and the stream became narrow and had to have dilatation and now is on CIC. The 84 years old man was lost to follow-up 8months following perineal urethrotomy operation. The median follow up was 26.2 months excluding two patients who were lost from follow up and the results are good. Discussion BXO involvement of the urethra poses a challenge when considering urethral reconstruction that will have minimal recurrence. Surgical treatment is required to patients with severe form of BXO causing significant LUTS and particularly poor urine flow. Some patients actually develop retention of urine and several degrees of compensations like chronic retention and Hydronephrosis and hydroureter and the renal insufficiency that ensues. Stasis of urine is a problem that causes urinary tract infections and infection which may lead to development of sinuses and fistulas. Urethral dilatation as observed by others3,4,5 causes more trauma and fibrosis and is discouraged. Excision of the affected urethra is the key to successful treatment of this condition. Several substitution options for reconstruction of urethral stricture are used where the affected length is long, skin being one of them. But in case of BXO, the skin is involved with the disease or may become involved during follow up and hence, not recommended. Therefore substitution from other tissues is highly needed to treat established urethral disease and several innovative works using different tissues have been published4,5,6,7,8. In this series of patients who had established disease of the urethral at our institution only buccal mucosa graft has been used for obvious reasons mainly experience of the surgeons and results obtained from this technique. We learnt this technique in the year 2003 and since then we have been able to use it to different types of reconstructions where a long segment of urethra is lost. Buccal mucosa is a versatile substitional material as it is easy to harvest and has a good take with its adaptability to wet environment easily gets well in the urethra exposed by urine. Bladder mucosa is not a choice here where schistosomal endemicity is high and may require other investigations like Cystoscopy to rule out bladder changes of Bilharzia before its consideration. We excised the whole fibrotic tissues and replaced it with buccal mucosa in 14 patients. In 10 patients as single stage on-lay and in four patients as two stage procedure was performed. One patient 84 years old patient had multiple sinuses and urethral cutaneous fistula with pus and infection of the right testis with extensive BXO involving prepuce ventral skin of the penis and urethra to the level of bulbous urethra. This one was offered excision of the affected urethra and the affected skin and had to have perineal urethrotomy. This patient was lost to follow up after eight months, he became dry and was voiding through the urethrotomy created in the perineum. Ten patients who had on-lay buccal mucosa graft single stage had good meatal cosmesis and observed flow of urine was adequate with a mean flow rate of 20mls per second on the average. One patient had re-stenosis and was dilated at urethroscopy there was no evidence of fibrosis beyond the 0.5 cm from the meatus and had a meatotomy done and has been kept on Clean self intermittent catheterization. We have not described patients with mild form in this series because most of our patients get circumcised early and also can be circumcised in the case of prepuce involvement of lichen sclerosus. Buccal mucosa replacement of urethra affected by lichen sclerosis is the preferred mode of treatment in our center. More follow up however is required to assess the long term results. Conclusion BXO is a rare cause of urethral stricture in our institution and buccal mucosa graft offers satisfactory intermediate term results. References
Copyright 2011 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js11040t4.jpg] [js11040t1.jpg] [js11040t3.jpg] [js11040f1.jpg] [js11040t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}