 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 16, No. 2, July/August, 2011, pp. 135-138 Fine Needle Aspiration: A simple and convenient alternative for diagnosing and treating ganglions. S N. Ramraje, N. Chaturvedi, V Bhatia, A Goel Department of
Pathology, Grant Medical College, Mumbai-400008 Code Number: js11041 Background: Ganglion cysts are common lesions of the hand and
wrist. They are usually asymptomatic well circumscribed soft to firm nodules.
Their origin is still muddled in controversy. Here we report our experience
with fine needle aspiration of ganglions. Introduction Ganglion cysts are relatively common lesions resulting from mucoid, cystic degeneration of soft tissues adjacent to a joint space. There are three hypotheses regarding their origin. They may form
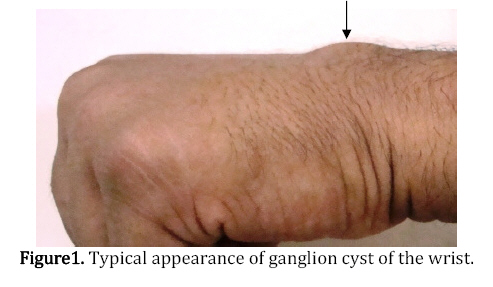
Many patients present to doctors due to the fear of malignancy or because the swelling is cosmetically undesirable1. Although they are mostly asymptomatic, in rare circumstances they may cause limitation of mobility, pain, and weakness and paresthesia. The objective of treatment is to relieve symptoms and establish a definitive diagnosis. Surgical excision is the commonly used method of treatment. But fine needle aspiration is found to be a simple, inexpensive and low risk alternative method advocated as a diagnostic modality and in most of the cases as a therapeutic modality for ganglion cysts1,2. Patients and Methods- In this report we present a study of ganglion cysts diagnosed and simultaneously treated by fine needle aspiration in our tertiary care hospital from January 2009 to July 2010. Duration of the study was 19 months. Total number of patients subjected to FNA was 20.The patients' ages ranged from 31/2 to 80 years. Males and females were equal in number. Of the 20 ganglion cysts, 14 were present on the dorsum of hand, three on the dorsum of foot and one each on the thenar aspect at the base of thumb, toe and popliteal fossa (Figure 1) All of them presented to our hospital for the first time and did not have a history of aspiration elsewhere or a previous surgical excision. Six patients came for fine needle aspiration of unrelated conditions and during their visit to the doctor for these, they mentioned the presence of another lump which was either asymptomatic or causing some pain or limitation of movement. The cysts were aspirated by the pathologist as follows-
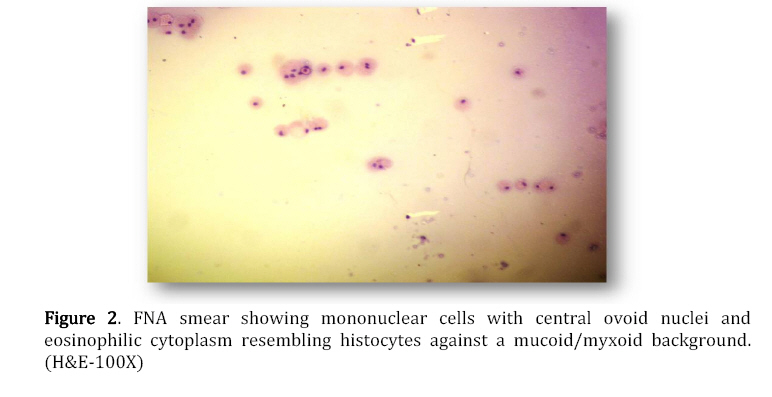
Microscopically the smears were monotonous and showed single mononuclear cells with central ovoid nuclei and eosinophilic cytoplasm resembling histocytes against a background of abundant mucoid/myxoid material (Figure 2). Follow-up Nine patients followed up to hospital for other medical problems unrelated to ganglion cysts.On examination,neither there was any visible swelling at the site of aspiration nor did the patient complain of any symptom related to ganglion cyst. Hence it was concluded that the cyst had been treated by FNA. Only one patient had to undergo surgical excision due to the large size of the cyst. No patient came with a recurrence to date. Discussion Ganglion cysts, also known as bible cysts, are swellings that often appear on or around joints and tendons in the hand or foot. They are most frequently located around the dorsum of wrist especially at the scapho-lunate joint, which accounts for 60-70% of all ganglion cysts of hand and wrist 3. Ganglion cysts can also arise from the radioscaphoid or scaphotrapezial joint volarly. The other sites, although less common, include base of the fingers on the palm, the fingertip just below the cuticle, dorsum of foot and near the knee, ankle and shoulder joint. Ganglion cysts are common soft-tissue tumors of the hand and wrist. They occur three times more commonly in women and are predominantly seen in young adults being rare in children4. They are small outpouchings of joint capsule if they are found around a joint or of tendon lining tissue if they are found near a tendon. In general, ganglion cysts consist of an outer fibrous coat and an inner lining, and contain a clear, colorless, gelatinous fluid. Microscopically, fine needle aspiration smears show single mononuclear cells resembling histocytes against a background of abundant mucoid/myxoid material. Ultrastructural studies have revealed the fibroblastic and/or histiocytic nature of the cells5 Hence we believe that in an appropriate clinical setting, the diagnosis of ganglion cyst can be made by FNA confidently. Though no confirmed etiology is known, the theory that ganglion originates from degeneration of the mucoid connective tissue, specifically collagen, has been prevalent since 1893, when Ledderhose described it as such6. Ganglion cysts can occur as an outpouching of synovium or as an irritation of articular tissue, forming a new cyst The most common etiological theory is degeneration of connective tissue with formation of cystic space6. It has also been suggested that connective tissue degeneration is caused by irritation or chronic damage causing the mesenchymal cells/ fibroblasts to produce mucin4. Ganglion cysts can be unilobulated or often multilobulated, with connective tissue septa separating the cavities. According to Thornburg4, a ganglion cyst is not a true cyst because there is no epithelial lining to the cyst wall, and, hence, the theories of synovial herniation or synovial tumor formation are disputed. The origin of ganglion cyst remains controversial. Many theories have been postulated till now. Treatments have also varied including the ancient and classical method of alarming the cyst with family Bible7, aspiration under local anaesthesia8 and injection of sclerosing fluids7 or steroids9. An out-dated method of treating a ganglion cyst was supposedly to strike the lump with a large heavy book, causing the cyst to rupture and drain into the surrounding tissues. The term "Bible bump" comes from a common urban legend which states that since even the poorest households often possessed a Bible, this was commonly used, which led to the nicknaming of ganglion cysts as "Jillian's lump", "Bible bumps" or "Gideon's disease."This type of treatment is not recommended by some doctors as it can damage the area around the cyst and may have a higher recurrence rate than aspiration or excision. Today surgical approach is the most widely used method and leads to the lowest recurrence rate. But surgical excision is an expensive approach for a relatively asymptomatic condition. The cost of anaesthesia, overnight admission and the patient losing his working days, all make the surgical method expensive. Also, complications like damage to vital nerves and tendons, and hypertrophic scars and keloids occur. Aspiration with a thick bore needle as treatment of ganglion cysts has been used in the past by De Orsay et al and Mc Evedy7,8. The method of fine needle aspiration has several advantages, eg using thin bore needle avoids use of local anaesthesia, the procedure takes less than ten minutes, and in majority of cases the cyst collapses after FNA preventing further need of excision. Physical activity is not restricted and patient is able to return to his day-to-day routine. There are no complications and the cost of the procedure is negligible. Follow up of the patients is easy and simple. The patients don't lose their working days and thus their productivity is uninterrupted. There are reports wherein a syringe holder was used for better control over the needle to completely puncture and aspirate the contents of the cysts, which is not used in our institute. In our study, the swelling reduced in size in eight patients and in 12 cases it collapsed after FNA preventing further need for excision. We did not encounter any complications by this minimally invasive, atraumatic procedure and no patient has returned with a recurrence till date .This could probably be due to the short span of study time and the small number of patients sampled. Follow up of patients with recurrences and additional aspirations would be simple and reduce failure rate if any. If recurrence does occur, patient can undergo surgical removal. References
Copyright 2011 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js11041f2.jpg] [js11041f1.jpg] |
| |||||||||

{kind=link}
{kind=link}