 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 16, No. 2, July/August, 2011, pp. 146-150 Rectal bleeding amongst Medical Students: Prevalence and Consultation Behaviour. Adedayo O.T, Babatunde A.S., Adekoya O A, Nwokoro C C Department of Surgery,
Olabisi Onabanjo University Teaching Hospital Sagamu, Nigeria Code Number: js11043 Background: Rectal bleeding can be a symptom
of colorectal cancer. Consultation behaviour of health care professionals may
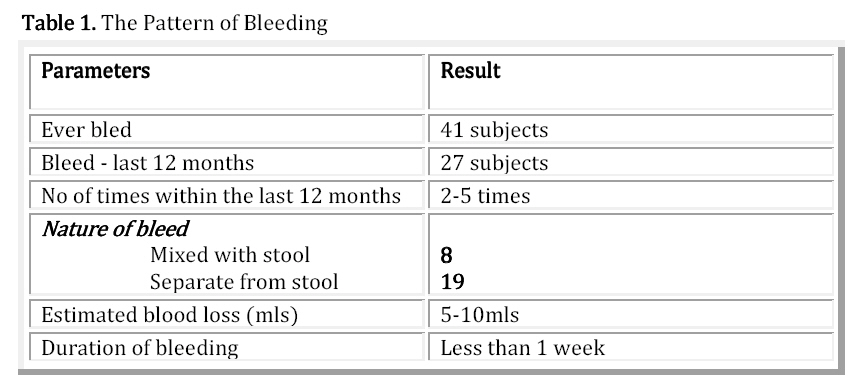
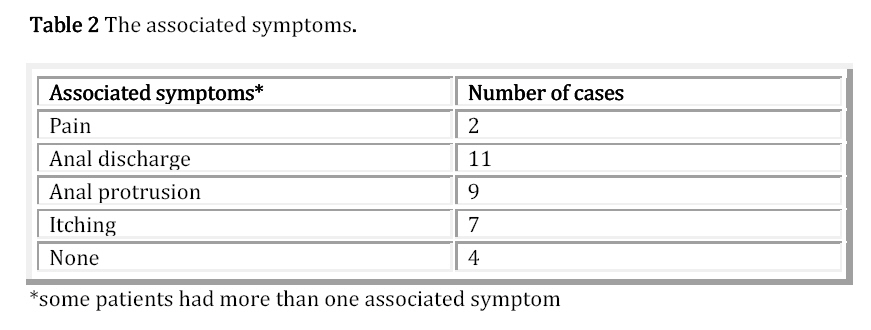
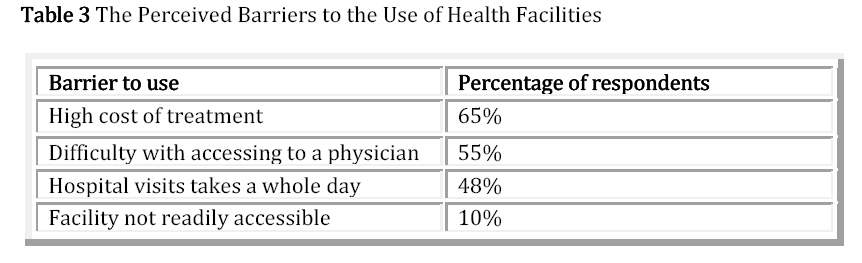
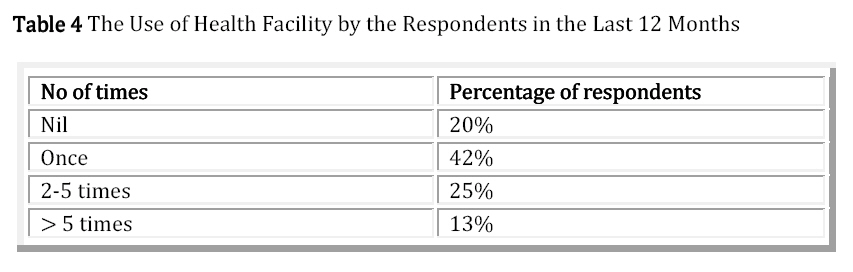
influence the attention they give to patients who consult them. Introduction Rectal bleeding poses a problem for clinicians, because although it is common, it can be a symptom of colorectal cancer. Toit et al reported that 1 in 10 patients aged 45years and over with new onset rectal bleeding had colorectal neoplasia1. The prevalence of colorectal cancer in Nigeria is unknown, but hospital based reports suggest an increase in the number of cases being treated2,3 In the UK 30,000 new cases of colorectal cancer are diagnosed annually and 11% of cancer deaths are due to colorectal cancer4. Survival from colorectal cancer is dependent on the stage at diagnosis. Timely investigation and early detection offer the best chance of survival. Health care professionals have a role to play in early diagnosis. Their perception of the seriousness or otherwise of the symptom of rectal bleeding influences the attention they give to patients who consult them with this symptom. National guidelines for referral, investigation and management of rectal bleeding, exist in the developed world4.. Such guidelines are yet to be developed for Nigeria. Consultation behaviour in relation to rectal bleeding has rarely being studied in health care professionals. Most studies had been in patients, a consultation rate of 34% was reported in a study conducted in Newcastle5; while a rate of 5% was reported in Sagamu6. This was a study of the prevalence of rectal bleeding and consultation behaviour amongst medical students who will become doctors in the near future. Subjects and Methods One hundred and ninety-two final year medical students of Olabisi Onabanjo University had questionnaire administered in class, to determine the prevalence of rectal bleeding and their consultation behaviour. The results were then analyzed. The study was approved by the Ethical Review Committee of the Hospital. Results All the 192 questionnaires were returned. Five out of them were discarded for incomplete data. One out of these five had rectal bleeding in the past 12months. One hundred and eighty-seven records were analyzed. The mean age of the subjects was 26yrs. (age range = 23-30yrs). The male to female ratio was 1:1.8 One hundred and seventy-eight was single while 9 were married. Forty-one (21.9%) had bled in their lifetime, while 27(14.4%) had bled in the last 12 months. Three were pregnant; none of these had rectal bleeding in the past 12 months. Table 1 shows the pattern of bleeding; blood was separate from stool in 19 subjects, less than 5-10mls and lasted less than one week. Table 2 shows the associated symptoms, anal discharge and rectal protrusion were the common associated symptoms. Only 5(18.5%) out of 27 consulted a physician. The reasons for consultation were pain in 2 subjects, perception of the bleeding as being serious in 5 subjects. Twenty-two did not consult a physician. Reasons for non-consultation in 18 subjects were that they felt they knew the cause of the bleeding, 21 felt that the bleeding would stop anyway, 15 bought drugs for use, and 12 subjects would not like a rectal examination. In response to questions on causes of rectal bleeding, hemorrhoids, cancer and tear in the anal region were selected. When asked what they thought was responsible for their own rectal bleeding, the list included tear in the anus, hemorrhoids and constipation. All the subjects however said that they would advise a friend or relative to consult a doctor for rectal bleeding. Table 3 shows the perceived barriers to the use of health facilities, high cost of treatment and delays in the hospital were rated high. Table 4 shows the use of health facility by the respondents in the last 12 months Out of the 5 subjects that consulted a physician, only two had physical examination and digital rectal examination performed by the physician. Discussion This study shows that the one year prevalence rate of rectal bleeding amongst the group of medical students studied is 14%. This rate is comparable to the one year prevalence rate of 18% and 15% reported in the adult populations in Newcastle5 and Sagamu6. We found that although rectal bleeding was common, only a minority sought medical advice. In this study only one out of six (18.5%) sought medical advice. This figure is lower than the 30% to 41% consultation rate reported from the developed world.5 but higher than the 5% reported from Nigeria6. Several factors may be responsible for this. The factors include a high level of awareness and easy access to health facilities in the developed countries, on the one hand, and self-medication and difficult access in less developed countries on the other hand. Other reasons for non-consultation may be related to the community belief that the bleeding is from “jedi jedi”, a local terminology for piles, which does not require the attention of a physician. This belief is rooted in folklore and has no scientific basis. Cancer of the rectum is not uncommon in this age group as 2-10% of all colorectal cancers occur in patients aged less than 40years.8, 9, 10. Obstacles to the use of health facilities listed in Table 3 also contribute and require the attention of the government. Medical students will eventually graduate as doctors. Their perception of the seriousness a symptom such as rectal bleeding will influence the attention they give to patients with such symptom. In this study, the main reason for not seeing a physician is that they felt the cause was known and resulted to self medication. No differences were found between consulters and non-consulters in the frequency and severity of the symptoms, knowledge of causes of rectal bleeding and action taken before consultation. Rectal bleeding can be a symptom of rectal cancer. The high prevalence and low consultation rate for rectal bleeding do however indicate the need to balance initiatives in health education against the resources available to deal with the problem. Risk factors known to be associated with colorectal cancer include age over 40yrs, a family history of colorectal cancer and the characteristics of the bleeding. However there are several reports of cases occurring in the younger age group (18-30yrs)7. Over 90% of cases of colorectal cancer occur sporadically and without any recognized predisposing factor. Survival of patients with colorectal cancer is related to the stage of the disease at diagnosis. Timely investigation and early detection offer the best chance of survival. Advanced stage of disease at diagnosis may result from delays due to late consultation and inadequate assessment by the attending physician. In this study only 40% of the consulters had a rectal examination. It is recommended that all patients with rectal bleeding should have a minimum of digital rectal examination. Recurrent episodes indicate the need for further investigation. Conclusion Rectal bleeding is relatively common amongst the group of medical students studied. Only one in six, who perceived the symptom a serious, consulted a physician. Guidelines for referral, investigation and management of rectal bleeding are required in countries, such as Nigeria, where such do not currently exist. References
Copyright 2011 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js11043t1.jpg] [js11043t4.jpg] [js11043t2.jpg] [js11043t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}