 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 16, No. 3, Nov/Dec, 2011, pp. 6-34 A Review of Surgical Capacity and Surgical Education Programmes in The COSECSA Region I. Kakande, N. Mkandawire, MIW Thompson A collaboration between the Royal College of Surgeons in Ireland (RCSI) and the College of Surgeons of East Central and Southern Africa (COSECSA) Code Number: js11047 1. Introduction The College of Surgeons of East, Central and Southern Africa (COSECSA) is an independent body that fosters postgraduate education in surgery and provides surgical training throughout the region of East, Central and Southern Africa. COSECSA decided to conduct a survey of surgical capacity and surgical education in the COSECSA countries: Ethiopia, Kenya, Malawi, Mozambique, Rwanda, Uganda, Tanzania, Zambia and Zimbabwe. The aim of this research wasto map out the current status of surgical capacity and training in the region with a view to developing key guidelines and recommendations concerning surgical education for COSECSA surgical trainees at Fellowship (FCS) and Membership (MCS) levels as well as exploring ways of complementing and enhancing synergies between COSECSA surgical training and existing university based surgical training programmes. In addition, the survey also intended to map out the surgical capacity and training of non- physician clinicians (NPCs) conducting essential surgery in these countries. The survey identifies the region’s existing surgical programmes and non physician programmes and the type of training provided. The survey also investigates each country’s training programmes, the entry qualifications required and the associated cost of training. The survey was conducted by Prof N. Mkandawire from Malawi and Prof I. Kakande from Uganda between June and July 2010. The former covered Mozambique, Zambia, Zimbabwe and his home country Malawi while the latter covered Ethiopia, Rwanda, Tanzania, Kenya and his home country Uganda. The key stake holders met during these visits were: Ministry of Health officials, training institutions officials, Medical Council officials and COSECSA country representatives. Where data was not available representatives were asked to provide estimated figures. The completion of the report and literature review was conducted by Dr MIW Thompson between August and September 2011. This research was funded by Irish Aid support for the collaboration programme between COSECSA and the Royal College of Surgeons in Ireland (RCSI). 2. Literature Review of Surgical Capacity in Africa It has been recognized that providing surgical care is important in reducing mortality and morbidity in developing countries. Surgical conditions from burns, injuries, cancers and obstetric complications amount to 11% of the world’s disability-adjusted life years and are important contributors to the overall burden of disease. In the African continent, 10 million disability adjusted life years (DALYs) are caused by accidents and 4 million DALYs by obstetric complications.1,2 Of the 47 countries in sub-Saharan Africa, 38 do not meet the WHO recommended minimum of 20 doctors and 100 nurses per 100,000 population or the surgical specialties mix required to deal with the burden of surgical diseases.3 This report suggests that there is currently only one surgeon for every 196,000 people. In rural areas this declines to only one surgeon for every 2.5 million people living in rural areas in Africa.2 In developing countries, there is little data or publications related to the capacity of surgical services delivery in hospitals. It is even more difficult to measure how much surgical research is being done in Africa. A recent study in 2011 found that of 2,236 publications on training, only 561 discussed surgery and 40% of these articles were published from within Africa. Published articles on training in Africa tended to cover internationalorganisations rather than national universities therefore under representing the number of training initiatives. Many countries in the publications cited less than two references in their papers and those with two or more were predominantly from West Africa, particularly Nigeria.4 The World Health Organisation (WHO) estimates that managing surgical diseases is an important determinant of the public health crisis in developing countries. The lack of information on surgical services and capacity in developing countries propelled the WHO5 to work closer with ministries of health, WHO local offices and academia to reduce mortality and morbidity related to surgical conditions as well as strengthening existing training programs.6,7 It is important to address the deficit in surgical care as it has been also shown to be as economically cost effective as providing vaccination programs.8,9 3. Demography of COCESCA Countries The data provided by country representatives was triangulated with WHO figures. In order to provide data of similar time periods the WHO data on country statistics were used. The graphs below show the figures from the WHO global health observatory and represent a snapshot view of country profiles for 2009 – the latest figures publically available10,11. The most populated country is Ethiopia with almost 83 million people. The least populated of the region is Rwanda with a population of 10 million. The total population for the COCECSA region is 272.6 million. Although being the least populated country, Rwanda invested 9% of its GDP on health care a figure similar to European countries in 2009. This was double the investment of Kenya and Ethiopia each investing 4.3% of GDP. Zimbabwe figures were not estimated by WHO as little data was available since 2001. Recent figures from country representatives showed an increase in health care spending as a percentage of GDP; Ethiopia 10.4%, Kenya 7.9%, Malawi 8.0%, Mozambique 15.0%, Rwanda 9-15%. Kenya had the highest income per capita (US $1,560), almost double the income for Malawi. Figure 4 below shows the life expectancies in COSECSA countries. Kenya had the highest life expectancy for men and women (58 years and 62 years respectively) and Malawi had the lowest life expectancy (44 years for men and 51 years for women). In comparison, the average life expectancy for the African region was 52 years for men and 56 years for women; and the global life expectancy was 66 years for men and 71 years for women. Mozambique had the highest infant mortality rate (92/1,000 live births) and Tanzania had the lowest Infant mortality rate (50/1,000 live births). The average African infant mortality rate was 75/1,000 live births and the global average was 40/1,000 live births Tanzania had the highest maternal mortality rate (790/100,000) and Uganda had the lowest maternal mortality rate (430/100,000). The average African maternal mortality rate 620/100,000 and the global average was 266/100,000. For developed countries the average maternal mortality rate was 14/100,000. 4. Current Status of Surgical Training in the Region 4.1 Overview of Non COSECSA Training Programmes All surgical training programmes in COSECSA countries are government funded and trainees usually receive a full salary and other related benefits. Surgical trainees are required to have completed undergraduate medical training, their intership posts and government service usually in a rural district hospital before being eligible for government funding. Of the COSECSA countries, the shortest surgical training time was for Urology in Kenya (two years), however trainees are required to have an MMed surgical qualification before embarking on the urology programme. The longest training programmes were found in Kenya and Mozambique lasting 5 years for nearly all programmes. Different countries had implemented surgical training programmes at different times. Table 1 shows the surgical training programmes in each country and a more in depth review of individual countries are provided in the appendix section (page 38). 4.2 Overview of COSECSA Training Programme COSECSA has two training programmes, the membership and the fellowship. The membership programme is designed to train the candidate in the basic principles of surgery and give the candidate a broad knowledge of surgery in general. It leads to the qualification of Member of the College of Surgeons of East Central and Southern Africa, MCS (ECSA). Membership of the College does not confer specialist status but signifies that the member is ready to pursue higher surgical training in a particular specialty. This involves a minimum of 2 years training. The fellowship programme leads to the exit qualification of Fellow of the College of Surgeons of East Central and Southern Africa, FCS (ECSA) that qualifies the successful candidate as a specialist surgeon. Six different specialities are offered: General Surgery, Orthopaedics, Neurosurgery, Urology, Paediatrics and Plastic Surgery. The training lasts a minimum of 5 years including the membership. Forty nine (49) surgeons have graduated from the COSECSA programme, 79 have finished the membership programme and there are currently 125 candidates in training. COSECSA also has two accredited training institutions in West Africa. These hospitals are associated with the Pan African Academy of Surgeons (PAACS) and have been accredited as COSECSA training locations. No trainees have yet completed the fellowship or membership. There are 9 candidates in training in Cameroon and 7 in Gabon. 4.3 Ethiopia Overview of Surgical Training Ethiopia has well established postgraduate surgical training programmes in general surgery, orthopaedics and plastics which have been running since 1980, 1996 and 2004 respectively. Between 2004 and 2009 programmes in urology, neurosurgery, cardiothoracic surgery and ENT (ear, nose and throat) surgery were introduced. For these programmes, trainees must have a general surgery qualification as a minimum entry requirement. All postgraduate surgery programmes are based at the University teaching hospital in Addis Ababa. All surgical trainees have been nationals and protected funding from the government allows between 38 and 52 surgeons to be trained annually. There appears to be no regular government funded external training programmes in surgical areas even if not offered locally. To be eligible for government funding, candidates must have worked for at least two years post graduation in government service for each year of funded training. The unit cost of training a surgeon was not readily available but is estimated to be the same for local and foreign students. So far, more than 372 surgeons have been trained. COSECSA Training Three surgeons have graduated from the COSECSA programme, 8 have finished the membership programme and there are currently 2 candidates in training. There are 5 accredited training facilities. 4.4 Kenya Overview of Surgical Training Kenya has long standing post graduate surgical programmes in general surgery, ophthalmology, anaesthesia, ENT and Neurosurgery which started in 1971, 1978, 1979, 1987 and 2005 respectively. For orthopaedics, all trainees must have general surgery training as a minimum entry requirement before they can be enrolled onto the programme. The orthopaedic programme started in 2008 and is a 5 year training programme. Government scholarships are available for surgical training but are very limited as allocation is spread over many departments. On average, approximately 40 students are enrolled annually and the cost of training is approximately US $2,326 annually per student. Newer programmes in plastics, urology, cardio-thoracics and paediatric surgery will start in 2012 which are all 5 year programmes except urology which consists of two years post MMEd training. Currently, MMed training is offered at Nairobi University and Moi University in Eldoret. Moi University is due to produce its first cohort of MMed graduates in March 2012. The number of trained surgeons from Nairobi University of since 1971 for the MMed surgery programme is approximately 242. Nairobi University is also a WHO training centre for ophthalmology so a large number of students are from other regions in Africa. Nairobi University has trained 147 ophthalmologists so far however it is not clear how many are Kenyan nationals. The Kenyan health report of 2005-2007 estimated that there were 57 ophthalmologists in Kenya nationally.i COSECSA Training Fourteen (14) surgeons have graduated from the COSECSA fellowship programme, 20 have finished the membership programme and there are currently 32 candidates in training. There are 17 accredited training facilities. 4.5 Malawi Overview of Surgical Training Malawi has MMed surgical postgraduate programmes in general surgery, ophthalmology and orthopaedics which started in 2005. The government has some targets for training Malawian surgeons both locally and abroad and there are protected funds for postgraduate surgical training. The local MMed tuition fee is US $3,000 annually per student. To be eligible for government funding, candidates must have completed two years public service work post internship. Government funded trainees continue to enjoy full salaries and other normal benefits. Approximately 6 surgical students are funded annually and so far 3 have completed surgical training (2 in ophthalmology and 1 in general surgery). Although surgeons trained with government funding are required to work for the government after training this is not enforced. Foreign nationals can be admitted into the MMed programmes at the same costs as local trainees. The sole medical school was started in 1991 with an output of 10 to 15 doctors per year in the first 15 years. Output has since increased to approximately 50 doctors per year since 2008 following the increase in student intake from 20 to 60 in 2003. It is hoped that the increasing number of graduates will correspondingly increase entry into the postgraduate programmes and surgical careers. COSECSA Training Four surgeons have graduated from the COSECSA fellowship programme, 5 have finished the membership programme and there are currently 12 candidates in training. There are 3 accredited training facilities. 4.6 Mozambique Overview of Surgical Training Mozambique has established surgical postgraduate programmes in plastic surgery, neurosurgery, cardiothoracic surgery and paediatric surgery which are offered as ‘hybrid’ programmes with the first two years of basic surgical training done in Mozambique and the higher surgical training done overseas; traditionally in Spain or Brazil. The locally based programmes which run for three years are in general surgery, orthopaedics, urology, ENT, maxillofacial surgery and ophthalmology. All postgraduate surgical programmes are based in Maputo at the Central Hospital and a specialist certificate is awarded by the Medical Council upon completion of training. Previously this was awarded by the Ministry of Health. All surgical trainees are funded by the government and there are no private or self-funded trainees. To be eligible for government funding the candidate must have worked in public service for two or three years. Trainees are predominantly Mozambican nationals although some candidates from Sao Tome and Principe and Cape Verde are trained in Mozambique funded by their governments. There is no formal requirement to work for the government after government funded surgical training. Approximately 18 to 27 trainees are enrolled into surgical training programmes annually with fees of approximately US $10,540 annually per student. The literature estimates that the State Medical School (UEM) has trained 22 physicians yearly from 1975 to 2003, with an increase in medical student reaching 120 MD/year trained after 2007. For specialized Mozambican MDs (including surgeons) it is estimated that in 2003, 21 new MDs completed their post-graduate study, and 70 more have been trained between 2004 and 2007.ii This seems plausible asUEM was started in 1963 with an intake of approximately 30 students annually. Between 1975 and late 1980’s output declined because of the civil war. In early 2000 intake increased to 100-150. Mozambique is unique in that UEM does not offer post graduate qualification. The training is done at the central hospital but exams are set by the medical council (previously set by Ministry of Health) who also issue the specialist certificate. COSECSA Training The COSECSA training programme has not yet begun in Mozambique. There are 2 accredited training facilities. 4.7 Rwanda Overview of Surgical Training Postgraduate surgical training in Rwanda started in 2006 for general surgery. To be eligible for government funding, candidates must have worked for two years post internship in public service. So far all trainees have been Rwandese nationals and are required to work for the government after training. The government has protected funding for 8 surgical trainees per year and one candidate has been trained so far. There is no plan for external training for surgical specialties already offered locally. The annual training fee for a Rwandese national is US $6,500 compared to US $14,000 annually per for a foreign national. At present, Rwanda has a total of 32 Rwandese surgeons and 15 expatriate surgeons. A recently published study estimated that there were 9 Rwandan anaesthesiologists and 17 Rwandan surgeons which is lower than the above figure but this probably represents figures from a couple of years previously. The surgeons and anaesthesiologists are practicing almost exclusively at referral hospitals.iii COSECSA training No surgeons have yet graduated from the COSECSA fellowship programme, 3 have finished the membership programme and there are currently 3 candidates in training. There are 3 accredited training facilities. 4.8 Tanzania Overview of Surgical Training Surgical training programmes offered in Tanzania are in general surgery, orthopaedics (both four years), Urology and neurosurgery (both three years) are offered as post general surgery programmes. It is not clear when the programmes started as this information was not provided. There doesn’t seem to be protected government funding or training targets for surgery. Government funded candidates must have worked for minimum of two years in public service and are bonded to work for government for three years after training. Approximately 15 students are trained a year costing US $7,400 annually per student and foreign candidates train at the same cost as local trainees. Figures for the total number of surgeons trained were not readily available. COSECSA Training No surgeons have yet graduated from the COSECSA fellowship programme or finished the membership programme. There are currently 6 candidates in training and 6 accredited training facilities. 4.9 Uganda Overview of Surgical Training: The idea of training specialist surgeons locally rather than sending them abroad for Fellowship was conceived by the late Professor Sir Ian McAdam and Head of Department of Surgery at Makerere Medical School. He and his colleagues coined the term MMed. MMed training programmes in general surgery, ophthalmology, ENT and maxillofacial surgery were started in 1967, 1972, 1975 and 2010 respectively. Due to the rapid increase in the numbers of traumatic injuries and orthopaedics, the late Professor Belcher initiated the MMed Orthopaedics and trauma in 1993 when he recruited two general surgery residents to MMed Orthopaedics. In 2002, another medical school Mbarara University of Science and Technology (MUST) started MMed General Surgery. In 2010, The Uganda Martyrs University at Nkozi opened The Mother Kevin Postgraduate Medical School at Nsambya in Kampala and started MMed General Surgery. Currently, the MMed training programmes in Uganda last three years (post MBCHB) except for orthopaedics which is four years. Although currently the duration is three years for General Surgery, discussion are in progress to extend the MMed programmes to four years. The cost of surgical training ranges between US $3,000 and US $8,000 annually per student. Students undertaking maxillofacial surgery need a BDS qualification as a minimum entry requirement. COSECSA Training: 13 surgeons have graduated from the COSECSA fellowship programme, 10 have finished the membership programme and there are currently 26 candidates in training. There are 11 accredited training facilities. 4.10 Zambia Overview of Surgical Training: Zambia has well established MMed programmes in general surgery and orthopaedics started in 1986 and 1996 respectively. It recently introduced the urology programme in 2006. All MMed programmes are four year courses and are based in Lusaka at the University Teaching Hospital. The tuition cost is US $3,000 and US $11,500 per annum for local and foreign trainees respectively The government has protected funding for training surgeons and candidates must have worked for a minimum of two years in public service before they can be funded. Approximately 10 candidates are funded annually and there are no formal requirements to work for the government after training. Approximately 40 general surgeons and 7 orthopaedic surgeons have been trained since the programmes started. There have been 5 foreign nationals trained in General Surgery or orthopaedics. The private sector, especially mining companies with private hospitals also fund surgical trainees to work for them. COSECSA Training Seven surgeons have graduated from the COSECSA Fellowship programme while 24 candidates have completed the membership programme.Currently, there are 20 candidates in training. There are 6 accredited training facilities. 4.11 Zimbabwe Overview of Surgical Training: Zimbabwe has a well established MMed programme in general surgery which started in 1986. The urology programme was started in approximately 2000. Although a neurosurgery programme exists, recruitment into this programme has been erratic with several students abandoning the programme. Currently only one neurosurgery candidate is in training and no candidate has graduated from the programme. The government sponsors the majority of surgical trainees and eligible trainees must have completed two years internship and two years community service in a public hospital. There appear to be no training targets or protected government funding for surgical training and programmes are supported in an adhoc manner by the ministry of health. Approximately 7 trainees are funded annually. Although there is a formal requirement for government funded trainees to work for the government, this is not enforced. Local student cost is US $1,800 annually to train compared to US $5,000 annually for a foreign student. COSECSA Training: Nine (9) surgeons have graduated from the COSECSA fellowship programme, 9 have finished the membership programme and there are currently 8 candidates in training. There are 5 accredited training facilities. 5. Non Physician Clinicians in the Delivery of Surgery 5.1 Overview Non Physician Clinicians (NPCs) are trained in several COSECSA countries and provide surgical services. Their scope of training and surgical responsibility varies from country to country. In addition, their titles also vary which can sometimes cause confusion and is an opportunity for COSECSA as a regional surgical training institution to lead in developing standardised policy guidelines in the training and responsibilities of non-physician surgeons. Where NPCs reach a senior grade an alternative career progression into medicine can be made but they would need to meet the entry requirements for joining a medical school like other medical students. There are no NPCs doing surgical procedures in Zimbabwe and Rwanda. 5.2 Ethiopia Ethiopia has a cadre of 800 NPCs however it is not clear the structure of their programme or which cadre performs surgical procedures. It was also not possible to assess their deployment or career structure. There is evidence of nurse anaesthetists, emergency surgery health officers and obstretic health officers working in Southern Ethiopia. There are also nurse cataract surgeons working in the Gondar region from the Tropical Health and Education Trust (THET) organisation that supports health links partnering with UK hospitals and universities.15 There is little in the literature discussing NPCs in Ethiopia however a recently published retrospective assessed obstetric care in 11 hospitals and 2 health centres in the Tigray. Between 1st January, 2006 and 31st December 2008, NPCs performed 63% of the 11,059 obstetric procedures which had similar outcomes postoperatively to physicians.16 5.3 Kenya There are 25 approved training institutions for clinical officers training in Kenya. The programme was started between 1927 and 1929 and upon completion clinical officers are awarded a Diploma in Clinical Medicine. They are registered by the Clinical Officers Council and are accepted by the Medical Practitioners and Dentists Board as a part of the medical personnel in the Country. It is unlikely the total number of trained clinical officers since 1927 is known. The current average annual output is 579 (Kenyan strategic plan 2008-2012) and records from the Chief Government Clinical Officer at the Ministry of Medical Services shows that there are 9,200 are registered clinical officers.17 It is estimated that half the clinical officers trained are lost from government service. Nurses are also trained in anaesthesia and can undertake a diploma in Clinical Medicine. They then cease to be registered with the Nursing Council and fall under the Clinical Officers Council. Nearly all the anaesthesia outside the urban settings is administered by clinical officers. They are also in great demand in urban hospitals due to the shortage of anaesthesiologists. A huge proportion of ophthalmological surgery outside Nairobi is also performed by clinical officers. Caesarean sections however are not performed by clinical officers in Kenya. The career path for clinical officers is structured and they are able to move to senior grades provided funding is secured for their training. There is no system of credit transfer currently available to them. They are required to undertake continuous professional development (CPD) but this is ungraded. Alternatively, they can obtain a Master of Science (MSc) degree in Clinical Medicine and Community Health. This programme is offered in four Universities and the four year degree course was first offered in 1999. Alternatively, they can enter medical school and train to be doctors. Clinical officers are deployed at all levels and can work independently at dispensary and health centre level. They are however supervised by medical officers if working in district, provincial or national hospitals. Surgical clinical officers working in the private sector areas fall under the Clinical Officers Act allowing them to perform certain roles; managing cuts, abrasions, cellulitis, abscesses, uncomplicated arthritis/arthralgia, circumcisions, dental extractions and providing emergency burns treatment. The Act is yet to take into consideration the new cadre of postgraduate clinical officers who have higher levels of training. 5.4 Malawi Malawi has a cadre of clinical officers and their training programme first started in 1975. Upon completing a three year training period they are awarded a Diploma in Clinical Medicine by the Malawi College of Health Sciences, a government run institution or the Malamulo College of Health Sciences, a faith based training institution. Both of these institutions are also colleges for training other paramedical officers such as radiographers, pharmacy technicians and laboratory technicians. General clinical officers have to do an internship period of one year at a district or central hospital supervised senior clinical officers or medical officers. They are formally recognised by the Medical Council of Malawi and the Ministry of Health. These officers are deployed up to the level of central hospitals in Malawi. They can work independently and are supervised by medical officers. Like all other health care workers they have to do mandatory CPD courses to qualify for annual registration with the Malawi Medical Council. Their career paths in the civil service mean that they can be promoted to more senior clinical officer grades based on experience but unfortunately there are no higher qualifications in this cadre. To progress along the clinical ladder, they have to train as doctors by joining the first year of medical school and their level of experience and diploma does not allow any them any reduction in the length of their medical training. They are permitted to provide private practice after ten years of clinical work however any private practice registered by a clinical officer must have a registered supervising medical officer (doctor). To date, approximately 900 general clinical officers have been trained. The scope of their work includes: removing lumps and bumps; hernia repair; hydrocoele surgery, laparatomy for acute abdominal emergencies; obstetric and gynaecological conditions such as caesarean sections, surgery for ectopic pregnancy, tubal ligation, uterine dilatation and curettage. Following the success of general clinical officers, post basic clinical officer programmes were introduced in orthopaedics, anaesthesia, and ophthalmology where candidates train for another 18 months after several years of clinical practice as clinical officers. Anaesthetic clinical officers are the major providers of anaesthesia in the whole country at district and central hospital levels. Ophthalmic clinical officers manage acute eye emergencies and can perform cataract surgery and evisceration of the globe. Specialised orthopaedic clinical officers have been trained since 1985 and are deployed primarily in rural district hospitals managing 80% to 90% of the orthopaedic workload in Malawi. Since the program began, 140 orthopaedic clinical officers have been trained of whom 82 are in clinical practice. This is an increase from what is in the literature (117 trained).18 The scope of work for orthopaedic clinical officers includes: debridement of open fractures and application of external fixators, managing acute pyogenic musculoskeletal infections, manipulations of major joint dislocations and closed fractures, conservative treatment of degenerative musculoskeletal conditions, club foot disorders and other developmental childhood conditions. Research from Malawi on clinical officers has shown that they perform major and general surgery safely with similar outcomes to surgeons. A retrospective study evaluated the contribution of clinical officers to major general surgery at Zomba Central Hospital between 2003 and 2007. The results found that out of 2,931 major general surgical procedures 51% were performed by clinical officers. They also performed 50% of prostatectomies, ventriculo-peritoneal-shuntings and strangulated hernia repairs.19 Another study from Southern Malawi assessed surgical registers in 17 hospitals. In 2004, clinical officers performed 61% of the 18,524 surgical and gynaecological procedures. This increased to 87% in 2007 (of 19,644 procedures). Certified clinical officers performed 8.4% of major surgical operations increasing to 17.7% in 2007.20 5.5 Tanzania Partial data was provided by Tanzania representatives. Tanzania has a cadre of non-physician clinicians called assistant medical officers. These officers are deployed up to the level of district hospitals. They can work independently and are supervised by medical officers. They are not permitted to do private practice and are required to undertake activities in CPD which are ungraded. Their career path is not well structured and it is difficult to move to any other grade from this position. A review of obstetric complications in 14 Tanzanian hospitals showed that assistant medical officers provided most of the surgery outside of major cities. In an analysis of the 1,134 complicated deliveries and 1,072 major obstetrical operations, there were no significant differences between assistant medical officers and medical officers in outcomes, risk indicators, or quality of care. 21 5.6 Zambia Zambia has a cadre of junior non physician clinicians called clinical officers and a more senior cadre called Medical Licentiate. The programmes were started in 1936 (formally called Medical Assistants) and 1978 (formally called Assistant Medical Officer). Upon completion they are awarded a Diploma and higher Diploma respectively awarded by Chainama College. The higher diploma for the medical licentiate is underwritten by The University of Zambia. Both are formally recognised by the Medical Council of Zambia. Clinical officer programmes are three-year pre-service training programmes and an entry qualification of ‘O’ Level secondary school education is required. Four programmes are offered in general medicine, psychiatry, environmental health and maternal health nursing. Clinical officers do not do any major surgical procedures but can suture wounds and excise minor lumps and growths. To date, there are 2,656 clinical officers registered with the medical council but data of the total number trained since inception of the programme is unavailable. The Medical Licentiate course is offered as a two-year post basic programme. Entry qualification is a clinical officer diploma plus a minimum of three years of clinical experience. They do a one year internship post graduation. The programme started in 1978 as an Assistant Medical Officer course which was modelled on the Tanzanian programme of Assistant Medical Officer. This was changed to Medical Licentiate in 1991. Medical Licentiates work as assistants to doctors and are posted at district hospitals. They are able to perform emergency surgical, gynaecological and obstetric procedures such as hernia repairs and caesarean sections. Graduates are bonded to work for the government for two years. Since the programme started, 140 Medical Licentiates have been trained and currently 92 are on the medical council register. Training for both programmes is done at the Chainama College which is a Ministry of Health institution. Practical attachments are done at district / provincial hospitals including Kabwe, Monza, St Francis, Ndola and Kitwe. Training and practical supervision is undertaken by specialist doctors. Other post-basic clinical officer programmes are offered in anaesthesia, ophthalmology, and dermatology. Career progression as a Medical Licentiate is limited. They can join medical training but have to join in the first year having met the necessary academic requirements for medical training. It is not clear whether they are allowed to have private practice. There is also little in the literature regarding clinical officers in Zambia. A survey carried out in 7 Zambian hospitals found that 86% of 21,245 operations performed were straightforward enough to be taught to non-surgeons. General anaesthesia was also an area often managed by clinical officers22. 5.7 Rwanda The NPCs found in Rwanda are anaesthetic assistants. They train for three years at Kigali health institute and approximately 25 students are enrolled annually. The programmes started in 1996. It is not clear how may have been trained so far or their career progression. They can work independently and are supervised by anaesthesiologists. They are however not allowed to have private practice. 5.8 Mozambique Mozambique has a cadre of non-physician clinicians called surgical technicians. The programme was started in 1984. Upon completion of the programme they are awarded a diploma / licentiate given by the ministry of health. The surgical technician is a generalist paramedic trained to be competent in procedures in general surgery, orthopaedics, obstetric / gynaecology, plastic surgery and ENT. To date a total of 100 surgical technicians have been trained. Technician programmes in anaesthesia, ophthalmology, theatre nursing and theatre technicians have also been introduced. Plans are underway to introduce a four year licentiate nurse programme to train nurses in obstetric and gynaecological procedures such as caesarean sections, ectopic pregnancy surgery and hysterectomy. Training is done at the Maputo Central Hospital which is a government institution and practical attachments are done at district / provincial hospitals. Training and practical supervision are done by specialist doctors. The scope of work for surgical technicians ranges from minor procedures such as excision of minor lumps and bumps to more complicated surgical and obstetric / gynaecological procedures such as hernia repairs and caesarean sections. Technicians are deployed at district hospitals but occasionally at central hospitals. They can work independently but have to report to medical officers. There are no mandatory CPD requirements and their career progression is limited with previous experience not being taken into account when considering career changes. Their salary can continue to increase with years of service to be equivalent to that of doctors. An economic evaluation of costs found that surgically trained assistant medical officers (tecnicos de cirurgia) in Mozambique were more cost effective than specialist physicians (medical officers, surgeons and obstetrician/gynaecologists) as a cost per major obstetric surgical procedure. The 30-year cost per obstetric surgery was US $38.9 for tecnicos de cirurgia per procedure and US $144.1 for surgeons and obstetrician/gynaecologists. Even a doubling of their salaries was still cost effective, at a cost per surgery of US $60.3 per procedure versus US $144.1 for physicians.23 Regarding their retention, a cross-sectional study assessing obstetric procedures performed by 'tecnicos de cirurgia' and in 34 district hospitals in 2002 showed that after 7 years, 90% of clinical officers were still working in district hospitals, while almost no physicians were left. They also conducted more than half of obstetric operations overall (57% of 1,217 operation) and 92% of 3,246 operations in district hospitals.24 5.9 Uganda Uganda has a cadre of non-physician clinicians in surgery, orthopaedics, anaesthesia and public health started in 1958, 1952, 1971 and 1972 respectively. Clinical officers are trained in Mulago paramedical training school and three government schools in Mbale, Fort Portal and Gulu. They are formally recognised by the Paramedical Council of Uganda and upon completion they are awarded a diploma in clinical medicine and public health. A total of 1,787 have been trained. The scope of their work includes excision of minor lumps and bumps; draining abscesses and circumcision procedures. They are deployed at health centres and can work independently and can do private practice. CPD requirements are not mandatory. With only 10 Ugandan physician-anaesthesiologists, most of the anaesthesia care provided in rural areas is by non physician anaesthetic officers.25 There are also non-Governmental institutions training clinical officers. These are Medcare health professionals’ college in Kampala, Kabale institute of health sciences, St. Elizabeth Gulu institute of health sciences and Kampala international university. 6. Surgical Capacity 6.1 Surgeons Currently Practising in COSECSA Countries. Table 2 above, gives a breakdown of the number of surgeons practising in different specialities and shows that most surgeons are general surgeons. Figure 6 represents the number of surgeons per million people in the COSECSA. Kenya hasthe highest proportion of surgeons; 11 surgeons per million people. Mozambique has the least number; 1 surgeon per million people. It is well known than that there is a lack of clinical workforce in Sub Saharan Africa (discussed in the introduction section). Another example from the literature states that there are 27 neurosurgeons in East Africa for 250 million people.27 This is a similar rate to the total numberof neurosurgeons in Table 2; 39 per 272.6 million people. Surgeons represent a small proportion of total number of clinicians; approximately 10 to 20% of the clinical workforce (Table 13). 6.2 Surgical Camps/Outreach Programmes Surgical camps / out reach programmes were provided in 6 countries; Ethiopia, Kenya, Malawi, Tanzania, Uganda and Zambia. There is need to explore ‘cross-border’ surgical camps whereby a team of specialists drawn from the region can provide surgical services not normally available in a member country. 6.3 Access to Surgical Services Ethiopia has the highest number of medical schools but it is unclear how many medical graduates are produced annually. Kenya seems to have the highest output of medical graduates but it is likely that the estimates are an under representation. Countries with the least number of medical schools were Malawi, Rwanda and Zambia with 100 graduates per year. Table 12 below gives a very crude overview of the health care worker population as the figures may represent different collection times and sources. The numbers of health care staff were calculated to represent health staff per 100,000 people. Nurses were the most common health care group; with Uganda having the most at 191 per 100,000 population and Ethiopia having the lowest at 4 per 100,000 population – almost a 60 fold difference. These figures reflect the challenges of data quality and should be interpreted with caution as some datasets were not available to give full comparisons. They would also need validating with national and WHO estimates.10 6.4 Health Service Capacity It is well known that the health worker population is below the WHO standard for many African countries. For example, Kenya almost meets the WHO standard for the doctor: patient ratio of 1:5000 (Kenya’s figure is 1: 5,300) but does not meet the WHO standard for the nurse: patient ratio of 1:800 (Kenya’s figure is 1: 1430).28 All COSECSA countries reported providing free access to emergency surgical care; 5 countries provided national insurance, 3 countries provided a public ambulance service and 6 countries provided a private ambulance service. It is difficult to estimate the vacancy rates in COSECSA countries in table 13 above. At best these estimates combine various documents from different institutions produced at different times. Even in Kenya, other datasets suggest that vacancy rates could be as high as 43% for doctors, 45% for clinical officers and 57% for nurses which are higher than the above figures.28 6.5 Impact of COSECSA Training in the Region It is not clear what the total numbers of COSECSA members or fellows. Table 14 shows 203 foundation fellows (not including Zimbabwe and Tanzania). The literature estimated there were 300 COSECSA foundation fellows.29 The present number of members and fellows is approximately 633.30 7. Discussion This survey has reaffirmed that improving the standards of surgical care, education and training will help address the huge gap in surgical skills in the COSECSA region. The survey provides baseline information and a guide for future surveys as well as highlighting the latest data intelligence on the surgical activity through COSECSA. 7.1 Major Findings All COSECSA countries provide at least three MMed surgical programmes that are government funded and taught by the universities. They last approximately four years and trainees may be required to formally work for the government post training. All COSECSA countries have increased their surgical training programmes with more subspecialties available to trainees. Most countries offer general surgery and orthopaedics as first line surgical training programmes. Foreign students are also accepted in most countries but sometimes at a training cost higher than for local students. The increase in surgical training is a positive step and needs to continue as many medical students and junior doctors choose surgery as a career option. A Kenyan study on 300 medical students showed that surgery was their top career preference.31 Similarly in Malawi, 46% of clinical medical students from College of Medicine in Blantyre chose surgery as a career option; with general surgery being the most popular (27%), followed by neurosurgery (22%) and orthopaedics (19%).32 Students however shy away from a surgical career due to excessive workload, low financial returns, inadequate number of scholarships, inadequate supervision, inadequate facilities and poor work conditions.33 As a response, Uganda has published its strategy on improving surgical training needs and to recruit future surgeons. This includes re-designing the undergraduate and internship curriculum so doctors have better surgical skills before embarking on internship posts. As well as expanding training for anaesthesia, nursing and allied health disciplines.32 Non physician clinician programmes in the COSECSA region vary from country to country. The programmes last between two and four years depending on whether it is a basic or post-basic programme. The most common surgical programmes are general surgery, orthopaedics and anaesthetics. Non physician clinicians have autonomy and are also allowed to practice independently including having a private practice in most countries. There are several examples in the literature of the important roles of clinical officers. For example, in Mozambique, Uganda and Tanzania clinical officers perform 36% of major surgery and minor surgery and 8% of the anaesthesia for major surgery.34 Studies also show that non physician clinicians have similar clinical outcomes to physicians/surgeons especially if supervisory or training frameworks are in place. 16, 19, 21, 22 Training and supervisory roles also increased their confidence to perform surgical procedures and manage basic wound and surgical infections. 20, 35 7.2 Recommendations and Conclusions It is important for COSECSA to consider the barriers and facilitators of surgical training in the region and use this report as a baseline guide for its strategic plan and mapping out its training programmes. COSECSA needs to be more visible to both prospective surgical students and policy making stakeholders by advancing the concept of a ‘college without walls’ which decentralises surgical training away from centralised university teaching hospitals to accredited regional and provincial hospitals. This results in greater numbers of surgical trainees staying in their home countries and providing surgical services. All COSECSA countries must recognise the specialist COSECSA training and raise its profile to encourage future trainees to join the programme. At the time of the survey, Malawi, Uganda, Zambia, Zimbabwe and Rwanda had the COSECSA qualification fully recognised as a specialist qualification. Re-inforcing the hypothesis that recognition encourages uptake in training programmes. At a political level all Ministries of Health must be encouraged to fund surgical training through COSECSA and give COSECSA maximum financial, moral and political support. In addition, surgical training through COSECSA must be complimentary with existing university based programmes and not be seen as a competitor. They must harness positive synergies by strengthening each others’ weaknesses. The case for task shifting / task sharing of basic surgical procedures to NPCs and non-surgeon clinicians is more or less settled. Their justifications based on cost effectiveness, competency and retention of NPCs in rural areas as well releasing specialist surgeons from routine work are well established in the literature. The importance of COSECSA as a key stakeholder in surgical practice and training for NPCs in the region cannot be underestimated. Particularly if countries have well established NPC programmes. This includes designing standardised courses for future NPCs delivering basic surgical care at the district hospital level. This is crucial in the region as general medical officers spend several years at a district hospital immediately after graduating and often feel unprepared for surgical practice. Where NPC programmes are not established or are resisted, COSECSA must use evidence based best practice to influence policy makers and map out clear career paths for NPCs to ensure they continue to provide surgical care. COSECSA also needs to influence and advocate policy makers to improve basic surgical facilities, increase the number of health care workers and acute surgical care provision such as ambulance services. At undergraduate level, COSECSA must encourage medical students to take up careers in surgery as output from medical schools is increasing in the region. This can happen by encouraging formation of ‘surgical clubs’ as has been successfully done in the medical School in Rwanda. More information sharing needs to occur between COSECSA countries (like the Uganda example above) so that areas of good practice can benefit other members including MMed trainees and COSECSA members conducting future audits or research. This includes exploring the current ‘cross-border’ surgical camps where specialist teams can provide surgical services to other member countries enhancing best practices in the region. The scarcity of good surgical data from this survey shows that COSECSA must play a leading role in meticulous data keeping which can also support future requests made to policy makers. These recommendations are meant to improve the quality of surgical care to patients and bridge the staffing gap required to manage a population of 272.6 million people in the COSECSA region. 8. Appendices Appendix 1: Data on Surgical Programmes in the COSECSA Region by Country Table 16, Table 17, Table 18, Table19, Table 20. Table 21, Table 22, Table 23, Table 24 Appendix 2: Abbreviations
References
Copyright 2011 - East and Central African Journal of Surgery East and Central African Journal of Surgery, Vol. 16, No. 3, Nov/Dec, 2011, pp. 6-34 A Review of Surgical Capacity and Surgical Education Programmes in The COSECSA Region I. Kakande, N. Mkandawire, MIW Thompson A collaboration between the Royal College of Surgeons in Ireland (RCSI) and the College of Surgeons of East Central and Southern Africa (COSECSA) Code Number: js11047 1. Introduction The College of Surgeons of East, Central and Southern Africa (COSECSA) is an independent body that fosters postgraduate education in surgery and provides surgical training throughout the region of East, Central and Southern Africa. COSECSA decided to conduct a survey of surgical capacity and surgical education in the COSECSA countries: Ethiopia, Kenya, Malawi, Mozambique, Rwanda, Uganda, Tanzania, Zambia and Zimbabwe. The aim of this research wasto map out the current status of surgical capacity and training in the region with a view to developing key guidelines and recommendations concerning surgical education for COSECSA surgical trainees at Fellowship (FCS) and Membership (MCS) levels as well as exploring ways of complementing and enhancing synergies between COSECSA surgical training and existing university based surgical training programmes. In addition, the survey also intended to map out the surgical capacity and training of non- physician clinicians (NPCs) conducting essential surgery in these countries. The survey identifies the region’s existing surgical programmes and non physician programmes and the type of training provided. The survey also investigates each country’s training programmes, the entry qualifications required and the associated cost of training. The survey was conducted by Prof N. Mkandawire from Malawi and Prof I. Kakande from Uganda between June and July 2010. The former covered Mozambique, Zambia, Zimbabwe and his home country Malawi while the latter covered Ethiopia, Rwanda, Tanzania, Kenya and his home country Uganda. The key stake holders met during these visits were: Ministry of Health officials, training institutions officials, Medical Council officials and COSECSA country representatives. Where data was not available representatives were asked to provide estimated figures. The completion of the report and literature review was conducted by Dr MIW Thompson between August and September 2011. This research was funded by Irish Aid support for the collaboration programme between COSECSA and the Royal College of Surgeons in Ireland (RCSI). 2. Literature Review of Surgical Capacity in Africa It has been recognized that providing surgical care is important in reducing mortality and morbidity in developing countries. Surgical conditions from burns, injuries, cancers and obstetric complications amount to 11% of the world’s disability-adjusted life years and are important contributors to the overall burden of disease. In the African continent, 10 million disability adjusted life years (DALYs) are caused by accidents and 4 million DALYs by obstetric complications.1,2 Of the 47 countries in sub-Saharan Africa, 38 do not meet the WHO recommended minimum of 20 doctors and 100 nurses per 100,000 population or the surgical specialties mix required to deal with the burden of surgical diseases.3 This report suggests that there is currently only one surgeon for every 196,000 people. In rural areas this declines to only one surgeon for every 2.5 million people living in rural areas in Africa.2 In developing countries, there is little data or publications related to the capacity of surgical services delivery in hospitals. It is even more difficult to measure how much surgical research is being done in Africa. A recent study in 2011 found that of 2,236 publications on training, only 561 discussed surgery and 40% of these articles were published from within Africa. Published articles on training in Africa tended to cover internationalorganisations rather than national universities therefore under representing the number of training initiatives. Many countries in the publications cited less than two references in their papers and those with two or more were predominantly from West Africa, particularly Nigeria.4 The World Health Organisation (WHO) estimates that managing surgical diseases is an important determinant of the public health crisis in developing countries. The lack of information on surgical services and capacity in developing countries propelled the WHO5 to work closer with ministries of health, WHO local offices and academia to reduce mortality and morbidity related to surgical conditions as well as strengthening existing training programs.6,7 It is important to address the deficit in surgical care as it has been also shown to be as economically cost effective as providing vaccination programs.8,9 3. Demography of COCESCA Countries The data provided by country representatives was triangulated with WHO figures. In order to provide data of similar time periods the WHO data on country statistics were used. The graphs below show the figures from the WHO global health observatory and represent a snapshot view of country profiles for 2009 – the latest figures publically available10,11. The most populated country is Ethiopia with almost 83 million people. The least populated of the region is Rwanda with a population of 10 million. The total population for the COCECSA region is 272.6 million. Although being the least populated country, Rwanda invested 9% of its GDP on health care a figure similar to European countries in 2009. This was double the investment of Kenya and Ethiopia each investing 4.3% of GDP. Zimbabwe figures were not estimated by WHO as little data was available since 2001. Recent figures from country representatives showed an increase in health care spending as a percentage of GDP; Ethiopia 10.4%, Kenya 7.9%, Malawi 8.0%, Mozambique 15.0%, Rwanda 9-15%. Kenya had the highest income per capita (US $1,560), almost double the income for Malawi. Figure 4 below shows the life expectancies in COSECSA countries. Kenya had the highest life expectancy for men and women (58 years and 62 years respectively) and Malawi had the lowest life expectancy (44 years for men and 51 years for women). In comparison, the average life expectancy for the African region was 52 years for men and 56 years for women; and the global life expectancy was 66 years for men and 71 years for women. Mozambique had the highest infant mortality rate (92/1,000 live births) and Tanzania had the lowest Infant mortality rate (50/1,000 live births). The average African infant mortality rate was 75/1,000 live births and the global average was 40/1,000 live births Tanzania had the highest maternal mortality rate (790/100,000) and Uganda had the lowest maternal mortality rate (430/100,000). The average African maternal mortality rate 620/100,000 and the global average was 266/100,000. For developed countries the average maternal mortality rate was 14/100,000. 4. Current Status of Surgical Training in the Region 4.1 Overview of Non COSECSA Training Programmes All surgical training programmes in COSECSA countries are government funded and trainees usually receive a full salary and other related benefits. Surgical trainees are required to have completed undergraduate medical training, their intership posts and government service usually in a rural district hospital before being eligible for government funding. Of the COSECSA countries, the shortest surgical training time was for Urology in Kenya (two years), however trainees are required to have an MMed surgical qualification before embarking on the urology programme. The longest training programmes were found in Kenya and Mozambique lasting 5 years for nearly all programmes. Different countries had implemented surgical training programmes at different times. Table 1 shows the surgical training programmes in each country and a more in depth review of individual countries are provided in the appendix section (page 38). 4.2 Overview of COSECSA Training Programme COSECSA has two training programmes, the membership and the fellowship. The membership programme is designed to train the candidate in the basic principles of surgery and give the candidate a broad knowledge of surgery in general. It leads to the qualification of Member of the College of Surgeons of East Central and Southern Africa, MCS (ECSA). Membership of the College does not confer specialist status but signifies that the member is ready to pursue higher surgical training in a particular specialty. This involves a minimum of 2 years training. The fellowship programme leads to the exit qualification of Fellow of the College of Surgeons of East Central and Southern Africa, FCS (ECSA) that qualifies the successful candidate as a specialist surgeon. Six different specialities are offered: General Surgery, Orthopaedics, Neurosurgery, Urology, Paediatrics and Plastic Surgery. The training lasts a minimum of 5 years including the membership. Forty nine (49) surgeons have graduated from the COSECSA programme, 79 have finished the membership programme and there are currently 125 candidates in training. COSECSA also has two accredited training institutions in West Africa. These hospitals are associated with the Pan African Academy of Surgeons (PAACS) and have been accredited as COSECSA training locations. No trainees have yet completed the fellowship or membership. There are 9 candidates in training in Cameroon and 7 in Gabon. 4.3 Ethiopia Overview of Surgical Training Ethiopia has well established postgraduate surgical training programmes in general surgery, orthopaedics and plastics which have been running since 1980, 1996 and 2004 respectively. Between 2004 and 2009 programmes in urology, neurosurgery, cardiothoracic surgery and ENT (ear, nose and throat) surgery were introduced. For these programmes, trainees must have a general surgery qualification as a minimum entry requirement. All postgraduate surgery programmes are based at the University teaching hospital in Addis Ababa. All surgical trainees have been nationals and protected funding from the government allows between 38 and 52 surgeons to be trained annually. There appears to be no regular government funded external training programmes in surgical areas even if not offered locally. To be eligible for government funding, candidates must have worked for at least two years post graduation in government service for each year of funded training. The unit cost of training a surgeon was not readily available but is estimated to be the same for local and foreign students. So far, more than 372 surgeons have been trained. COSECSA Training Three surgeons have graduated from the COSECSA programme, 8 have finished the membership programme and there are currently 2 candidates in training. There are 5 accredited training facilities. 4.4 Kenya Overview of Surgical Training Kenya has long standing post graduate surgical programmes in general surgery, ophthalmology, anaesthesia, ENT and Neurosurgery which started in 1971, 1978, 1979, 1987 and 2005 respectively. For orthopaedics, all trainees must have general surgery training as a minimum entry requirement before they can be enrolled onto the programme. The orthopaedic programme started in 2008 and is a 5 year training programme. Government scholarships are available for surgical training but are very limited as allocation is spread over many departments. On average, approximately 40 students are enrolled annually and the cost of training is approximately US $2,326 annually per student. Newer programmes in plastics, urology, cardio-thoracics and paediatric surgery will start in 2012 which are all 5 year programmes except urology which consists of two years post MMEd training. Currently, MMed training is offered at Nairobi University and Moi University in Eldoret. Moi University is due to produce its first cohort of MMed graduates in March 2012. The number of trained surgeons from Nairobi University of since 1971 for the MMed surgery programme is approximately 242. Nairobi University is also a WHO training centre for ophthalmology so a large number of students are from other regions in Africa. Nairobi University has trained 147 ophthalmologists so far however it is not clear how many are Kenyan nationals. The Kenyan health report of 2005-2007 estimated that there were 57 ophthalmologists in Kenya nationally.i COSECSA Training Fourteen (14) surgeons have graduated from the COSECSA fellowship programme, 20 have finished the membership programme and there are currently 32 candidates in training. There are 17 accredited training facilities. 4.5 Malawi Overview of Surgical Training Malawi has MMed surgical postgraduate programmes in general surgery, ophthalmology and orthopaedics which started in 2005. The government has some targets for training Malawian surgeons both locally and abroad and there are protected funds for postgraduate surgical training. The local MMed tuition fee is US $3,000 annually per student. To be eligible for government funding, candidates must have completed two years public service work post internship. Government funded trainees continue to enjoy full salaries and other normal benefits. Approximately 6 surgical students are funded annually and so far 3 have completed surgical training (2 in ophthalmology and 1 in general surgery). Although surgeons trained with government funding are required to work for the government after training this is not enforced. Foreign nationals can be admitted into the MMed programmes at the same costs as local trainees. The sole medical school was started in 1991 with an output of 10 to 15 doctors per year in the first 15 years. Output has since increased to approximately 50 doctors per year since 2008 following the increase in student intake from 20 to 60 in 2003. It is hoped that the increasing number of graduates will correspondingly increase entry into the postgraduate programmes and surgical careers. COSECSA Training Four surgeons have graduated from the COSECSA fellowship programme, 5 have finished the membership programme and there are currently 12 candidates in training. There are 3 accredited training facilities. 4.6 Mozambique Overview of Surgical Training Mozambique has established surgical postgraduate programmes in plastic surgery, neurosurgery, cardiothoracic surgery and paediatric surgery which are offered as ‘hybrid’ programmes with the first two years of basic surgical training done in Mozambique and the higher surgical training done overseas; traditionally in Spain or Brazil. The locally based programmes which run for three years are in general surgery, orthopaedics, urology, ENT, maxillofacial surgery and ophthalmology. All postgraduate surgical programmes are based in Maputo at the Central Hospital and a specialist certificate is awarded by the Medical Council upon completion of training. Previously this was awarded by the Ministry of Health. All surgical trainees are funded by the government and there are no private or self-funded trainees. To be eligible for government funding the candidate must have worked in public service for two or three years. Trainees are predominantly Mozambican nationals although some candidates from Sao Tome and Principe and Cape Verde are trained in Mozambique funded by their governments. There is no formal requirement to work for the government after government funded surgical training. Approximately 18 to 27 trainees are enrolled into surgical training programmes annually with fees of approximately US $10,540 annually per student. The literature estimates that the State Medical School (UEM) has trained 22 physicians yearly from 1975 to 2003, with an increase in medical student reaching 120 MD/year trained after 2007. For specialized Mozambican MDs (including surgeons) it is estimated that in 2003, 21 new MDs completed their post-graduate study, and 70 more have been trained between 2004 and 2007.ii This seems plausible asUEM was started in 1963 with an intake of approximately 30 students annually. Between 1975 and late 1980’s output declined because of the civil war. In early 2000 intake increased to 100-150. Mozambique is unique in that UEM does not offer post graduate qualification. The training is done at the central hospital but exams are set by the medical council (previously set by Ministry of Health) who also issue the specialist certificate. COSECSA Training The COSECSA training programme has not yet begun in Mozambique. There are 2 accredited training facilities. 4.7 Rwanda Overview of Surgical Training Postgraduate surgical training in Rwanda started in 2006 for general surgery. To be eligible for government funding, candidates must have worked for two years post internship in public service. So far all trainees have been Rwandese nationals and are required to work for the government after training. The government has protected funding for 8 surgical trainees per year and one candidate has been trained so far. There is no plan for external training for surgical specialties already offered locally. The annual training fee for a Rwandese national is US $6,500 compared to US $14,000 annually per for a foreign national. At present, Rwanda has a total of 32 Rwandese surgeons and 15 expatriate surgeons. A recently published study estimated that there were 9 Rwandan anaesthesiologists and 17 Rwandan surgeons which is lower than the above figure but this probably represents figures from a couple of years previously. The surgeons and anaesthesiologists are practicing almost exclusively at referral hospitals.iii COSECSA training No surgeons have yet graduated from the COSECSA fellowship programme, 3 have finished the membership programme and there are currently 3 candidates in training. There are 3 accredited training facilities. 4.8 Tanzania Overview of Surgical Training Surgical training programmes offered in Tanzania are in general surgery, orthopaedics (both four years), Urology and neurosurgery (both three years) are offered as post general surgery programmes. It is not clear when the programmes started as this information was not provided. There doesn’t seem to be protected government funding or training targets for surgery. Government funded candidates must have worked for minimum of two years in public service and are bonded to work for government for three years after training. Approximately 15 students are trained a year costing US $7,400 annually per student and foreign candidates train at the same cost as local trainees. Figures for the total number of surgeons trained were not readily available. COSECSA Training No surgeons have yet graduated from the COSECSA fellowship programme or finished the membership programme. There are currently 6 candidates in training and 6 accredited training facilities. 4.9 Uganda Overview of Surgical Training: The idea of training specialist surgeons locally rather than sending them abroad for Fellowship was conceived by the late Professor Sir Ian McAdam and Head of Department of Surgery at Makerere Medical School. He and his colleagues coined the term MMed. MMed training programmes in general surgery, ophthalmology, ENT and maxillofacial surgery were started in 1967, 1972, 1975 and 2010 respectively. Due to the rapid increase in the numbers of traumatic injuries and orthopaedics, the late Professor Belcher initiated the MMed Orthopaedics and trauma in 1993 when he recruited two general surgery residents to MMed Orthopaedics. In 2002, another medical school Mbarara University of Science and Technology (MUST) started MMed General Surgery. In 2010, The Uganda Martyrs University at Nkozi opened The Mother Kevin Postgraduate Medical School at Nsambya in Kampala and started MMed General Surgery. Currently, the MMed training programmes in Uganda last three years (post MBCHB) except for orthopaedics which is four years. Although currently the duration is three years for General Surgery, discussion are in progress to extend the MMed programmes to four years. The cost of surgical training ranges between US $3,000 and US $8,000 annually per student. Students undertaking maxillofacial surgery need a BDS qualification as a minimum entry requirement. COSECSA Training: 13 surgeons have graduated from the COSECSA fellowship programme, 10 have finished the membership programme and there are currently 26 candidates in training. There are 11 accredited training facilities. 4.10 Zambia Overview of Surgical Training: Zambia has well established MMed programmes in general surgery and orthopaedics started in 1986 and 1996 respectively. It recently introduced the urology programme in 2006. All MMed programmes are four year courses and are based in Lusaka at the University Teaching Hospital. The tuition cost is US $3,000 and US $11,500 per annum for local and foreign trainees respectively The government has protected funding for training surgeons and candidates must have worked for a minimum of two years in public service before they can be funded. Approximately 10 candidates are funded annually and there are no formal requirements to work for the government after training. Approximately 40 general surgeons and 7 orthopaedic surgeons have been trained since the programmes started. There have been 5 foreign nationals trained in General Surgery or orthopaedics. The private sector, especially mining companies with private hospitals also fund surgical trainees to work for them. COSECSA Training Seven surgeons have graduated from the COSECSA Fellowship programme while 24 candidates have completed the membership programme.Currently, there are 20 candidates in training. There are 6 accredited training facilities. 4.11 Zimbabwe Overview of Surgical Training: Zimbabwe has a well established MMed programme in general surgery which started in 1986. The urology programme was started in approximately 2000. Although a neurosurgery programme exists, recruitment into this programme has been erratic with several students abandoning the programme. Currently only one neurosurgery candidate is in training and no candidate has graduated from the programme. The government sponsors the majority of surgical trainees and eligible trainees must have completed two years internship and two years community service in a public hospital. There appear to be no training targets or protected government funding for surgical training and programmes are supported in an adhoc manner by the ministry of health. Approximately 7 trainees are funded annually. Although there is a formal requirement for government funded trainees to work for the government, this is not enforced. Local student cost is US $1,800 annually to train compared to US $5,000 annually for a foreign student. COSECSA Training: Nine (9) surgeons have graduated from the COSECSA fellowship programme, 9 have finished the membership programme and there are currently 8 candidates in training. There are 5 accredited training facilities. 5. Non Physician Clinicians in the Delivery of Surgery 5.1 Overview Non Physician Clinicians (NPCs) are trained in several COSECSA countries and provide surgical services. Their scope of training and surgical responsibility varies from country to country. In addition, their titles also vary which can sometimes cause confusion and is an opportunity for COSECSA as a regional surgical training institution to lead in developing standardised policy guidelines in the training and responsibilities of non-physician surgeons. Where NPCs reach a senior grade an alternative career progression into medicine can be made but they would need to meet the entry requirements for joining a medical school like other medical students. There are no NPCs doing surgical procedures in Zimbabwe and Rwanda. 5.2 Ethiopia Ethiopia has a cadre of 800 NPCs however it is not clear the structure of their programme or which cadre performs surgical procedures. It was also not possible to assess their deployment or career structure. There is evidence of nurse anaesthetists, emergency surgery health officers and obstretic health officers working in Southern Ethiopia. There are also nurse cataract surgeons working in the Gondar region from the Tropical Health and Education Trust (THET) organisation that supports health links partnering with UK hospitals and universities.15 There is little in the literature discussing NPCs in Ethiopia however a recently published retrospective assessed obstetric care in 11 hospitals and 2 health centres in the Tigray. Between 1st January, 2006 and 31st December 2008, NPCs performed 63% of the 11,059 obstetric procedures which had similar outcomes postoperatively to physicians.16 5.3 Kenya There are 25 approved training institutions for clinical officers training in Kenya. The programme was started between 1927 and 1929 and upon completion clinical officers are awarded a Diploma in Clinical Medicine. They are registered by the Clinical Officers Council and are accepted by the Medical Practitioners and Dentists Board as a part of the medical personnel in the Country. It is unlikely the total number of trained clinical officers since 1927 is known. The current average annual output is 579 (Kenyan strategic plan 2008-2012) and records from the Chief Government Clinical Officer at the Ministry of Medical Services shows that there are 9,200 are registered clinical officers.17 It is estimated that half the clinical officers trained are lost from government service. Nurses are also trained in anaesthesia and can undertake a diploma in Clinical Medicine. They then cease to be registered with the Nursing Council and fall under the Clinical Officers Council. Nearly all the anaesthesia outside the urban settings is administered by clinical officers. They are also in great demand in urban hospitals due to the shortage of anaesthesiologists. A huge proportion of ophthalmological surgery outside Nairobi is also performed by clinical officers. Caesarean sections however are not performed by clinical officers in Kenya. The career path for clinical officers is structured and they are able to move to senior grades provided funding is secured for their training. There is no system of credit transfer currently available to them. They are required to undertake continuous professional development (CPD) but this is ungraded. Alternatively, they can obtain a Master of Science (MSc) degree in Clinical Medicine and Community Health. This programme is offered in four Universities and the four year degree course was first offered in 1999. Alternatively, they can enter medical school and train to be doctors. Clinical officers are deployed at all levels and can work independently at dispensary and health centre level. They are however supervised by medical officers if working in district, provincial or national hospitals. Surgical clinical officers working in the private sector areas fall under the Clinical Officers Act allowing them to perform certain roles; managing cuts, abrasions, cellulitis, abscesses, uncomplicated arthritis/arthralgia, circumcisions, dental extractions and providing emergency burns treatment. The Act is yet to take into consideration the new cadre of postgraduate clinical officers who have higher levels of training. 5.4 Malawi Malawi has a cadre of clinical officers and their training programme first started in 1975. Upon completing a three year training period they are awarded a Diploma in Clinical Medicine by the Malawi College of Health Sciences, a government run institution or the Malamulo College of Health Sciences, a faith based training institution. Both of these institutions are also colleges for training other paramedical officers such as radiographers, pharmacy technicians and laboratory technicians. General clinical officers have to do an internship period of one year at a district or central hospital supervised senior clinical officers or medical officers. They are formally recognised by the Medical Council of Malawi and the Ministry of Health. These officers are deployed up to the level of central hospitals in Malawi. They can work independently and are supervised by medical officers. Like all other health care workers they have to do mandatory CPD courses to qualify for annual registration with the Malawi Medical Council. Their career paths in the civil service mean that they can be promoted to more senior clinical officer grades based on experience but unfortunately there are no higher qualifications in this cadre. To progress along the clinical ladder, they have to train as doctors by joining the first year of medical school and their level of experience and diploma does not allow any them any reduction in the length of their medical training. They are permitted to provide private practice after ten years of clinical work however any private practice registered by a clinical officer must have a registered supervising medical officer (doctor). To date, approximately 900 general clinical officers have been trained. The scope of their work includes: removing lumps and bumps; hernia repair; hydrocoele surgery, laparatomy for acute abdominal emergencies; obstetric and gynaecological conditions such as caesarean sections, surgery for ectopic pregnancy, tubal ligation, uterine dilatation and curettage. Following the success of general clinical officers, post basic clinical officer programmes were introduced in orthopaedics, anaesthesia, and ophthalmology where candidates train for another 18 months after several years of clinical practice as clinical officers. Anaesthetic clinical officers are the major providers of anaesthesia in the whole country at district and central hospital levels. Ophthalmic clinical officers manage acute eye emergencies and can perform cataract surgery and evisceration of the globe. Specialised orthopaedic clinical officers have been trained since 1985 and are deployed primarily in rural district hospitals managing 80% to 90% of the orthopaedic workload in Malawi. Since the program began, 140 orthopaedic clinical officers have been trained of whom 82 are in clinical practice. This is an increase from what is in the literature (117 trained).18 The scope of work for orthopaedic clinical officers includes: debridement of open fractures and application of external fixators, managing acute pyogenic musculoskeletal infections, manipulations of major joint dislocations and closed fractures, conservative treatment of degenerative musculoskeletal conditions, club foot disorders and other developmental childhood conditions. Research from Malawi on clinical officers has shown that they perform major and general surgery safely with similar outcomes to surgeons. A retrospective study evaluated the contribution of clinical officers to major general surgery at Zomba Central Hospital between 2003 and 2007. The results found that out of 2,931 major general surgical procedures 51% were performed by clinical officers. They also performed 50% of prostatectomies, ventriculo-peritoneal-shuntings and strangulated hernia repairs.19 Another study from Southern Malawi assessed surgical registers in 17 hospitals. In 2004, clinical officers performed 61% of the 18,524 surgical and gynaecological procedures. This increased to 87% in 2007 (of 19,644 procedures). Certified clinical officers performed 8.4% of major surgical operations increasing to 17.7% in 2007.20 5.5 Tanzania Partial data was provided by Tanzania representatives. Tanzania has a cadre of non-physician clinicians called assistant medical officers. These officers are deployed up to the level of district hospitals. They can work independently and are supervised by medical officers. They are not permitted to do private practice and are required to undertake activities in CPD which are ungraded. Their career path is not well structured and it is difficult to move to any other grade from this position. A review of obstetric complications in 14 Tanzanian hospitals showed that assistant medical officers provided most of the surgery outside of major cities. In an analysis of the 1,134 complicated deliveries and 1,072 major obstetrical operations, there were no significant differences between assistant medical officers and medical officers in outcomes, risk indicators, or quality of care. 21 5.6 Zambia Zambia has a cadre of junior non physician clinicians called clinical officers and a more senior cadre called Medical Licentiate. The programmes were started in 1936 (formally called Medical Assistants) and 1978 (formally called Assistant Medical Officer). Upon completion they are awarded a Diploma and higher Diploma respectively awarded by Chainama College. The higher diploma for the medical licentiate is underwritten by The University of Zambia. Both are formally recognised by the Medical Council of Zambia. Clinical officer programmes are three-year pre-service training programmes and an entry qualification of ‘O’ Level secondary school education is required. Four programmes are offered in general medicine, psychiatry, environmental health and maternal health nursing. Clinical officers do not do any major surgical procedures but can suture wounds and excise minor lumps and growths. To date, there are 2,656 clinical officers registered with the medical council but data of the total number trained since inception of the programme is unavailable. The Medical Licentiate course is offered as a two-year post basic programme. Entry qualification is a clinical officer diploma plus a minimum of three years of clinical experience. They do a one year internship post graduation. The programme started in 1978 as an Assistant Medical Officer course which was modelled on the Tanzanian programme of Assistant Medical Officer. This was changed to Medical Licentiate in 1991. Medical Licentiates work as assistants to doctors and are posted at district hospitals. They are able to perform emergency surgical, gynaecological and obstetric procedures such as hernia repairs and caesarean sections. Graduates are bonded to work for the government for two years. Since the programme started, 140 Medical Licentiates have been trained and currently 92 are on the medical council register. Training for both programmes is done at the Chainama College which is a Ministry of Health institution. Practical attachments are done at district / provincial hospitals including Kabwe, Monza, St Francis, Ndola and Kitwe. Training and practical supervision is undertaken by specialist doctors. Other post-basic clinical officer programmes are offered in anaesthesia, ophthalmology, and dermatology. Career progression as a Medical Licentiate is limited. They can join medical training but have to join in the first year having met the necessary academic requirements for medical training. It is not clear whether they are allowed to have private practice. There is also little in the literature regarding clinical officers in Zambia. A survey carried out in 7 Zambian hospitals found that 86% of 21,245 operations performed were straightforward enough to be taught to non-surgeons. General anaesthesia was also an area often managed by clinical officers22. 5.7 Rwanda The NPCs found in Rwanda are anaesthetic assistants. They train for three years at Kigali health institute and approximately 25 students are enrolled annually. The programmes started in 1996. It is not clear how may have been trained so far or their career progression. They can work independently and are supervised by anaesthesiologists. They are however not allowed to have private practice. 5.8 Mozambique Mozambique has a cadre of non-physician clinicians called surgical technicians. The programme was started in 1984. Upon completion of the programme they are awarded a diploma / licentiate given by the ministry of health. The surgical technician is a generalist paramedic trained to be competent in procedures in general surgery, orthopaedics, obstetric / gynaecology, plastic surgery and ENT. To date a total of 100 surgical technicians have been trained. Technician programmes in anaesthesia, ophthalmology, theatre nursing and theatre technicians have also been introduced. Plans are underway to introduce a four year licentiate nurse programme to train nurses in obstetric and gynaecological procedures such as caesarean sections, ectopic pregnancy surgery and hysterectomy. Training is done at the Maputo Central Hospital which is a government institution and practical attachments are done at district / provincial hospitals. Training and practical supervision are done by specialist doctors. The scope of work for surgical technicians ranges from minor procedures such as excision of minor lumps and bumps to more complicated surgical and obstetric / gynaecological procedures such as hernia repairs and caesarean sections. Technicians are deployed at district hospitals but occasionally at central hospitals. They can work independently but have to report to medical officers. There are no mandatory CPD requirements and their career progression is limited with previous experience not being taken into account when considering career changes. Their salary can continue to increase with years of service to be equivalent to that of doctors. An economic evaluation of costs found that surgically trained assistant medical officers (tecnicos de cirurgia) in Mozambique were more cost effective than specialist physicians (medical officers, surgeons and obstetrician/gynaecologists) as a cost per major obstetric surgical procedure. The 30-year cost per obstetric surgery was US $38.9 for tecnicos de cirurgia per procedure and US $144.1 for surgeons and obstetrician/gynaecologists. Even a doubling of their salaries was still cost effective, at a cost per surgery of US $60.3 per procedure versus US $144.1 for physicians.23 Regarding their retention, a cross-sectional study assessing obstetric procedures performed by 'tecnicos de cirurgia' and in 34 district hospitals in 2002 showed that after 7 years, 90% of clinical officers were still working in district hospitals, while almost no physicians were left. They also conducted more than half of obstetric operations overall (57% of 1,217 operation) and 92% of 3,246 operations in district hospitals.24 5.9 Uganda Uganda has a cadre of non-physician clinicians in surgery, orthopaedics, anaesthesia and public health started in 1958, 1952, 1971 and 1972 respectively. Clinical officers are trained in Mulago paramedical training school and three government schools in Mbale, Fort Portal and Gulu. They are formally recognised by the Paramedical Council of Uganda and upon completion they are awarded a diploma in clinical medicine and public health. A total of 1,787 have been trained. The scope of their work includes excision of minor lumps and bumps; draining abscesses and circumcision procedures. They are deployed at health centres and can work independently and can do private practice. CPD requirements are not mandatory. With only 10 Ugandan physician-anaesthesiologists, most of the anaesthesia care provided in rural areas is by non physician anaesthetic officers.25 There are also non-Governmental institutions training clinical officers. These are Medcare health professionals’ college in Kampala, Kabale institute of health sciences, St. Elizabeth Gulu institute of health sciences and Kampala international university. 6. Surgical Capacity 6.1 Surgeons Currently Practising in COSECSA Countries. Table 2 above, gives a breakdown of the number of surgeons practising in different specialities and shows that most surgeons are general surgeons. Figure 6 represents the number of surgeons per million people in the COSECSA. Kenya hasthe highest proportion of surgeons; 11 surgeons per million people. Mozambique has the least number; 1 surgeon per million people. It is well known than that there is a lack of clinical workforce in Sub Saharan Africa (discussed in the introduction section). Another example from the literature states that there are 27 neurosurgeons in East Africa for 250 million people.27 This is a similar rate to the total numberof neurosurgeons in Table 2; 39 per 272.6 million people. Surgeons represent a small proportion of total number of clinicians; approximately 10 to 20% of the clinical workforce (Table 13). 6.2 Surgical Camps/Outreach Programmes Surgical camps / out reach programmes were provided in 6 countries; Ethiopia, Kenya, Malawi, Tanzania, Uganda and Zambia. There is need to explore ‘cross-border’ surgical camps whereby a team of specialists drawn from the region can provide surgical services not normally available in a member country. 6.3 Access to Surgical Services Ethiopia has the highest number of medical schools but it is unclear how many medical graduates are produced annually. Kenya seems to have the highest output of medical graduates but it is likely that the estimates are an under representation. Countries with the least number of medical schools were Malawi, Rwanda and Zambia with 100 graduates per year. Table 12 below gives a very crude overview of the health care worker population as the figures may represent different collection times and sources. The numbers of health care staff were calculated to represent health staff per 100,000 people. Nurses were the most common health care group; with Uganda having the most at 191 per 100,000 population and Ethiopia having the lowest at 4 per 100,000 population – almost a 60 fold difference. These figures reflect the challenges of data quality and should be interpreted with caution as some datasets were not available to give full comparisons. They would also need validating with national and WHO estimates.10 6.4 Health Service Capacity It is well known that the health worker population is below the WHO standard for many African countries. For example, Kenya almost meets the WHO standard for the doctor: patient ratio of 1:5000 (Kenya’s figure is 1: 5,300) but does not meet the WHO standard for the nurse: patient ratio of 1:800 (Kenya’s figure is 1: 1430).28 All COSECSA countries reported providing free access to emergency surgical care; 5 countries provided national insurance, 3 countries provided a public ambulance service and 6 countries provided a private ambulance service. It is difficult to estimate the vacancy rates in COSECSA countries in table 13 above. At best these estimates combine various documents from different institutions produced at different times. Even in Kenya, other datasets suggest that vacancy rates could be as high as 43% for doctors, 45% for clinical officers and 57% for nurses which are higher than the above figures.28 6.5 Impact of COSECSA Training in the Region It is not clear what the total numbers of COSECSA members or fellows. Table 14 shows 203 foundation fellows (not including Zimbabwe and Tanzania). The literature estimated there were 300 COSECSA foundation fellows.29 The present number of members and fellows is approximately 633.30 7. Discussion This survey has reaffirmed that improving the standards of surgical care, education and training will help address the huge gap in surgical skills in the COSECSA region. The survey provides baseline information and a guide for future surveys as well as highlighting the latest data intelligence on the surgical activity through COSECSA. 7.1 Major Findings All COSECSA countries provide at least three MMed surgical programmes that are government funded and taught by the universities. They last approximately four years and trainees may be required to formally work for the government post training. All COSECSA countries have increased their surgical training programmes with more subspecialties available to trainees. Most countries offer general surgery and orthopaedics as first line surgical training programmes. Foreign students are also accepted in most countries but sometimes at a training cost higher than for local students. The increase in surgical training is a positive step and needs to continue as many medical students and junior doctors choose surgery as a career option. A Kenyan study on 300 medical students showed that surgery was their top career preference.31 Similarly in Malawi, 46% of clinical medical students from College of Medicine in Blantyre chose surgery as a career option; with general surgery being the most popular (27%), followed by neurosurgery (22%) and orthopaedics (19%).32 Students however shy away from a surgical career due to excessive workload, low financial returns, inadequate number of scholarships, inadequate supervision, inadequate facilities and poor work conditions.33 As a response, Uganda has published its strategy on improving surgical training needs and to recruit future surgeons. This includes re-designing the undergraduate and internship curriculum so doctors have better surgical skills before embarking on internship posts. As well as expanding training for anaesthesia, nursing and allied health disciplines.32 Non physician clinician programmes in the COSECSA region vary from country to country. The programmes last between two and four years depending on whether it is a basic or post-basic programme. The most common surgical programmes are general surgery, orthopaedics and anaesthetics. Non physician clinicians have autonomy and are also allowed to practice independently including having a private practice in most countries. There are several examples in the literature of the important roles of clinical officers. For example, in Mozambique, Uganda and Tanzania clinical officers perform 36% of major surgery and minor surgery and 8% of the anaesthesia for major surgery.34 Studies also show that non physician clinicians have similar clinical outcomes to physicians/surgeons especially if supervisory or training frameworks are in place. 16, 19, 21, 22 Training and supervisory roles also increased their confidence to perform surgical procedures and manage basic wound and surgical infections. 20, 35 7.2 Recommendations and Conclusions It is important for COSECSA to consider the barriers and facilitators of surgical training in the region and use this report as a baseline guide for its strategic plan and mapping out its training programmes. COSECSA needs to be more visible to both prospective surgical students and policy making stakeholders by advancing the concept of a ‘college without walls’ which decentralises surgical training away from centralised university teaching hospitals to accredited regional and provincial hospitals. This results in greater numbers of surgical trainees staying in their home countries and providing surgical services. All COSECSA countries must recognise the specialist COSECSA training and raise its profile to encourage future trainees to join the programme. At the time of the survey, Malawi, Uganda, Zambia, Zimbabwe and Rwanda had the COSECSA qualification fully recognised as a specialist qualification. Re-inforcing the hypothesis that recognition encourages uptake in training programmes. At a political level all Ministries of Health must be encouraged to fund surgical training through COSECSA and give COSECSA maximum financial, moral and political support. In addition, surgical training through COSECSA must be complimentary with existing university based programmes and not be seen as a competitor. They must harness positive synergies by strengthening each others’ weaknesses. The case for task shifting / task sharing of basic surgical procedures to NPCs and non-surgeon clinicians is more or less settled. Their justifications based on cost effectiveness, competency and retention of NPCs in rural areas as well releasing specialist surgeons from routine work are well established in the literature. The importance of COSECSA as a key stakeholder in surgical practice and training for NPCs in the region cannot be underestimated. Particularly if countries have well established NPC programmes. This includes designing standardised courses for future NPCs delivering basic surgical care at the district hospital level. This is crucial in the region as general medical officers spend several years at a district hospital immediately after graduating and often feel unprepared for surgical practice. Where NPC programmes are not established or are resisted, COSECSA must use evidence based best practice to influence policy makers and map out clear career paths for NPCs to ensure they continue to provide surgical care. COSECSA also needs to influence and advocate policy makers to improve basic surgical facilities, increase the number of health care workers and acute surgical care provision such as ambulance services. At undergraduate level, COSECSA must encourage medical students to take up careers in surgery as output from medical schools is increasing in the region. This can happen by encouraging formation of ‘surgical clubs’ as has been successfully done in the medical School in Rwanda. More information sharing needs to occur between COSECSA countries (like the Uganda example above) so that areas of good practice can benefit other members including MMed trainees and COSECSA members conducting future audits or research. This includes exploring the current ‘cross-border’ surgical camps where specialist teams can provide surgical services to other member countries enhancing best practices in the region. The scarcity of good surgical data from this survey shows that COSECSA must play a leading role in meticulous data keeping which can also support future requests made to policy makers. These recommendations are meant to improve the quality of surgical care to patients and bridge the staffing gap required to manage a population of 272.6 million people in the COSECSA region. 8. Appendices Appendix 1: Data on Surgical Programmes in the COSECSA Region by Country Table 16, Table 17, Table 18, Table19, Table 20. Table 21, Table 22, Table 23, Table 24 Appendix 2: Abbreviations
References
Copyright 2011 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js11047t6.jpg] [js11047t11.jpg] [js11047t7.jpg] [js11047t1.jpg] [js11047t12.jpg] [js11047t15.jpg] [js11047t4.jpg] [js11047t5.jpg] [js11047f5.jpg] [js11047f4.jpg] [js11047f6.jpg] [js11047t8.jpg] [js11047t23.jpg] [js11047t22.jpg] [js11047t3.jpg] [js11047t13.jpg] [js11047t17.jpg] [js11047t18.jpg] [js11047f1.jpg] [js11047t19.jpg] [js11047f2.jpg] [js11047t14.jpg] [js11047t16.jpg] [js11047t10.jpg] [js11047t9.jpg] [js11047f3.jpg] [js11047t24.jpg] [js11047t20.jpg] [js11047t2.jpg] [js11047t21.jpg] |
| |||||||||

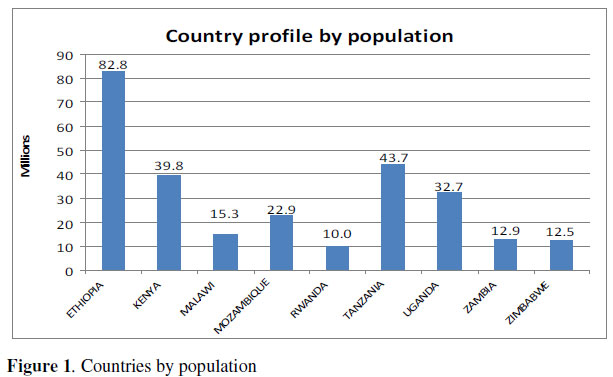{kind=link}
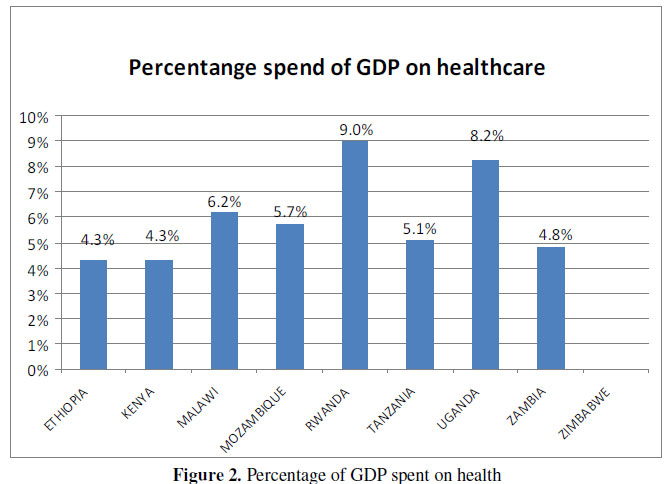{kind=link}
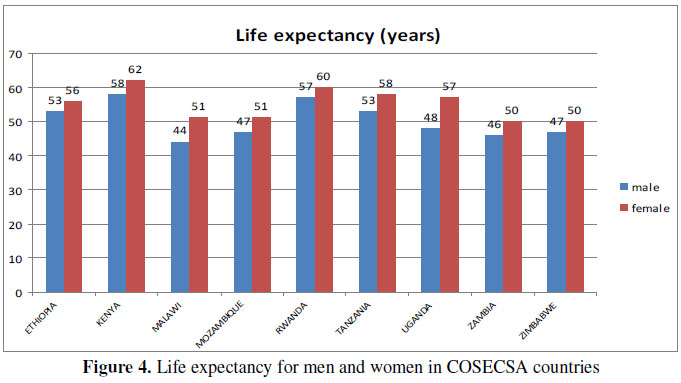{kind=link}
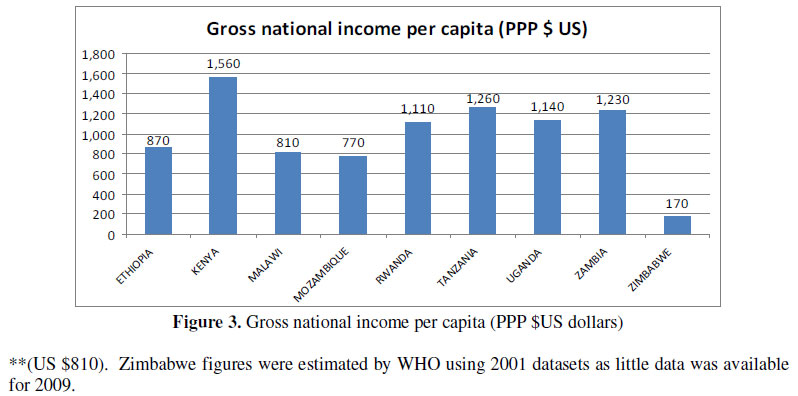{kind=link}
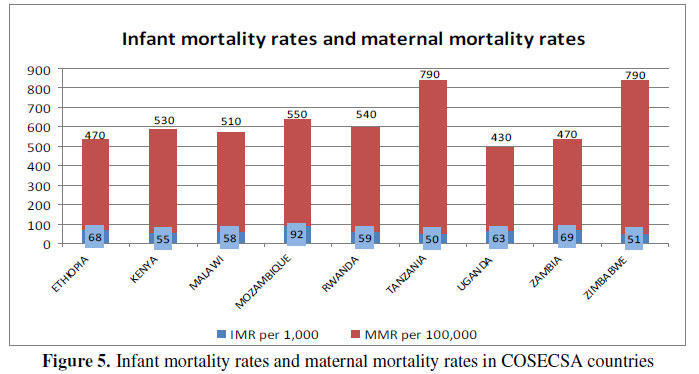{kind=link}
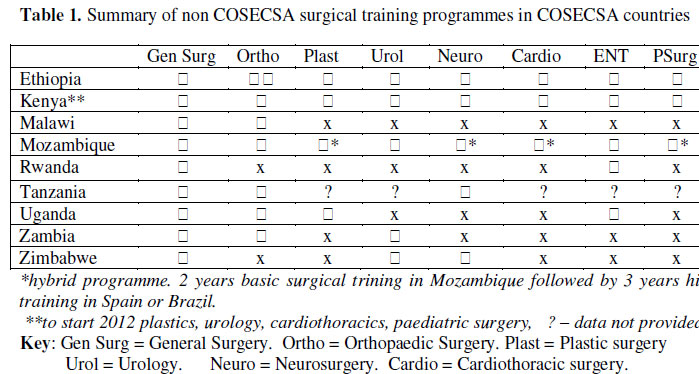{kind=link}
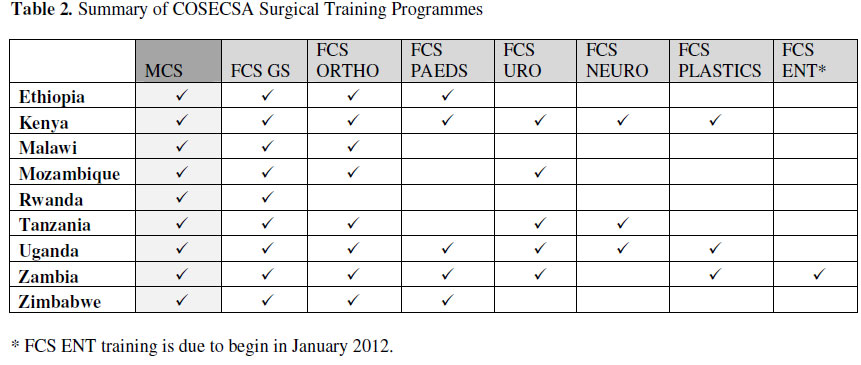{kind=link}
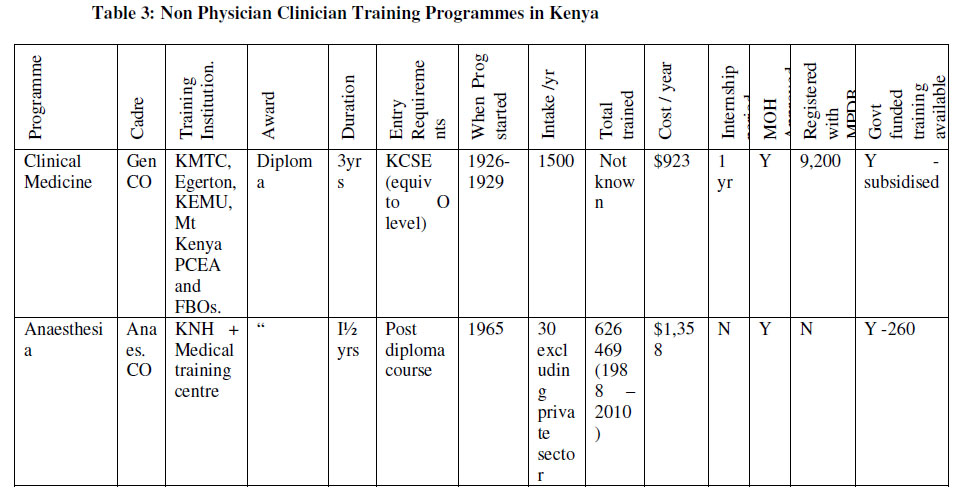{kind=link}
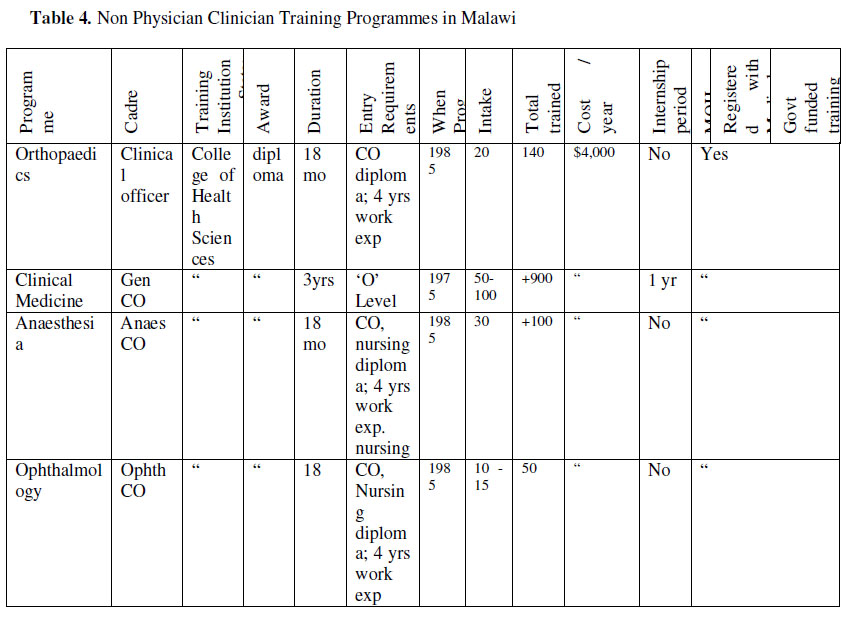{kind=link}
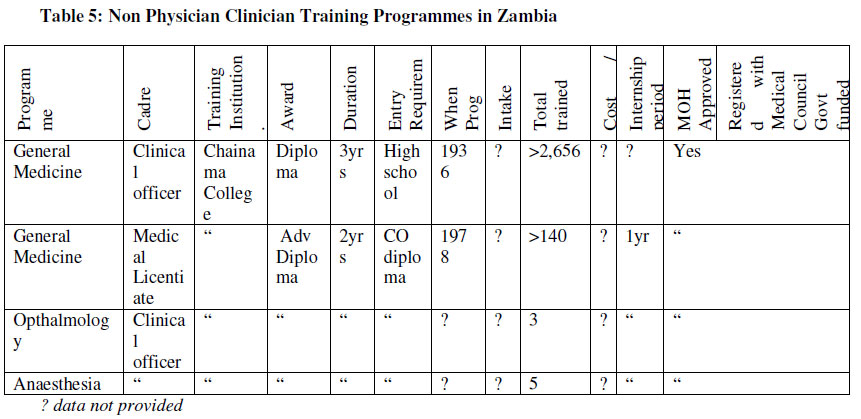{kind=link}
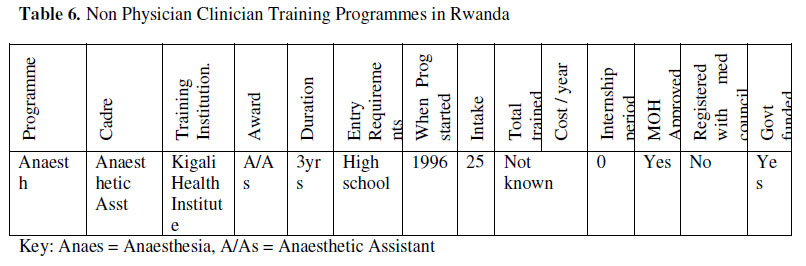{kind=link}
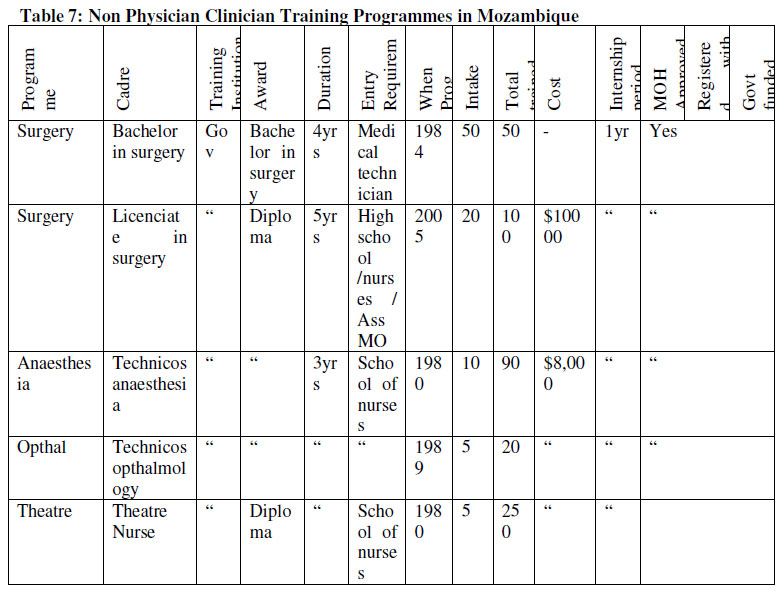{kind=link}
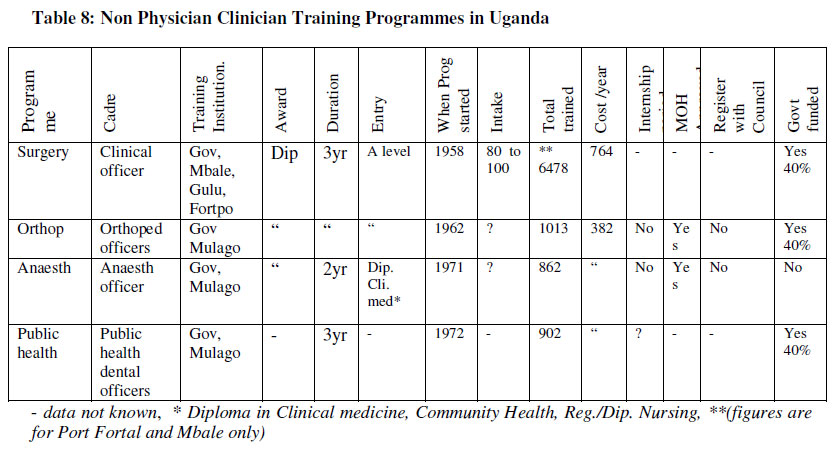{kind=link}
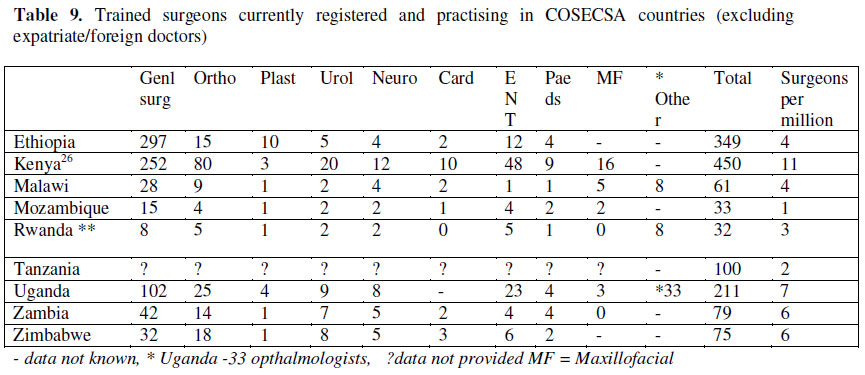{kind=link}
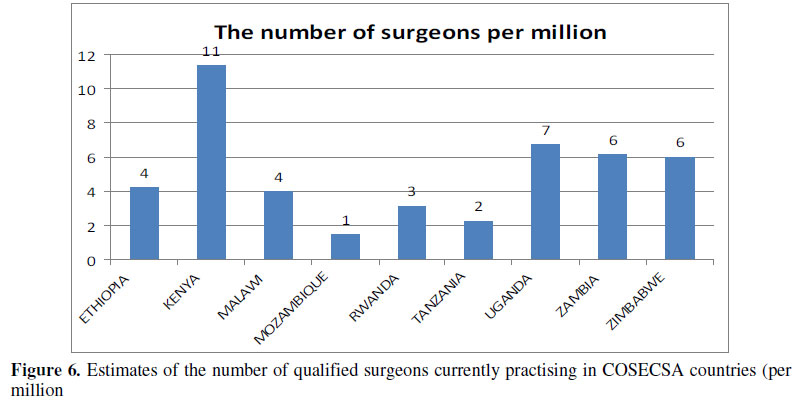{kind=link}
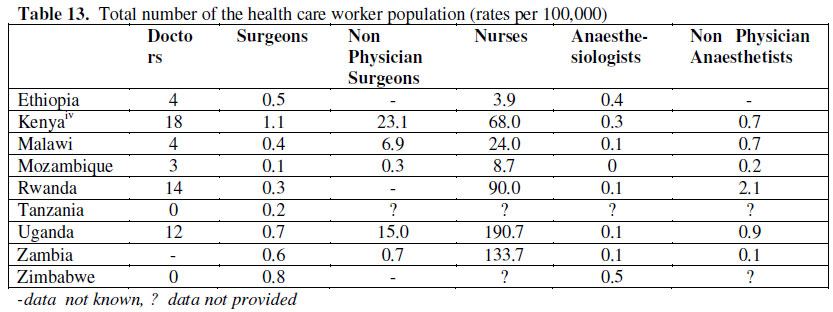{kind=link}
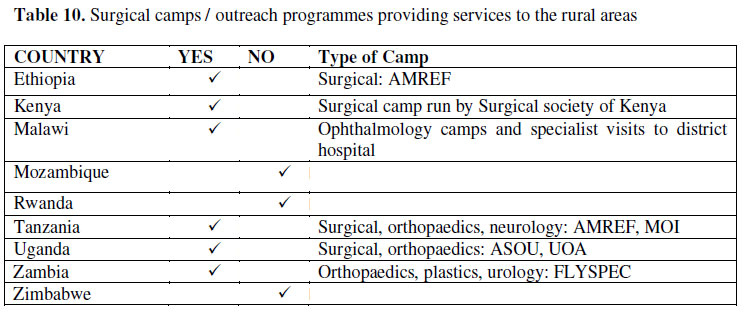{kind=link}
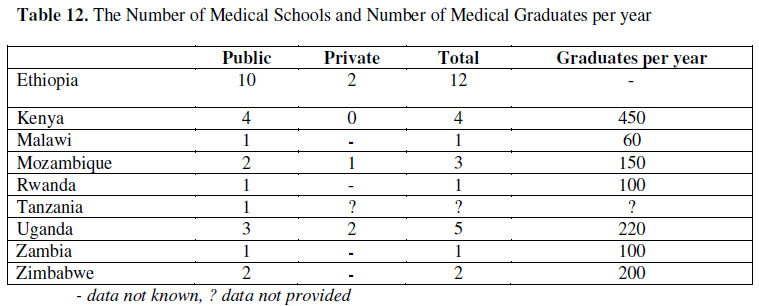{kind=link}
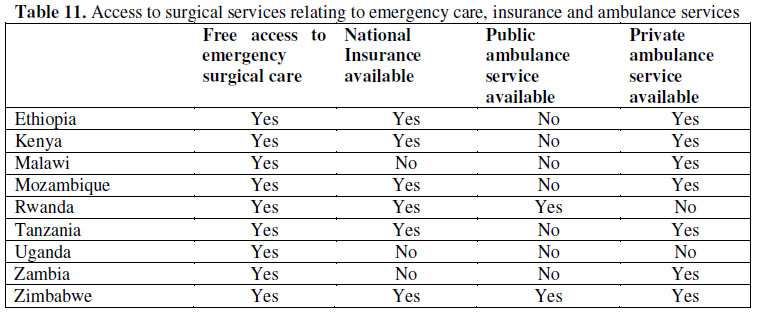{kind=link}
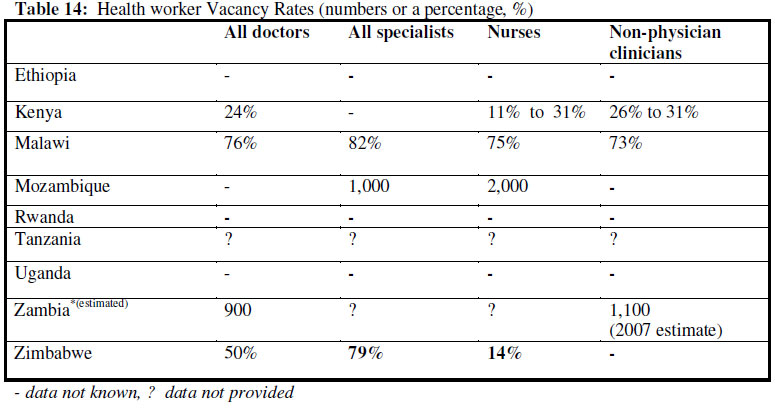{kind=link}
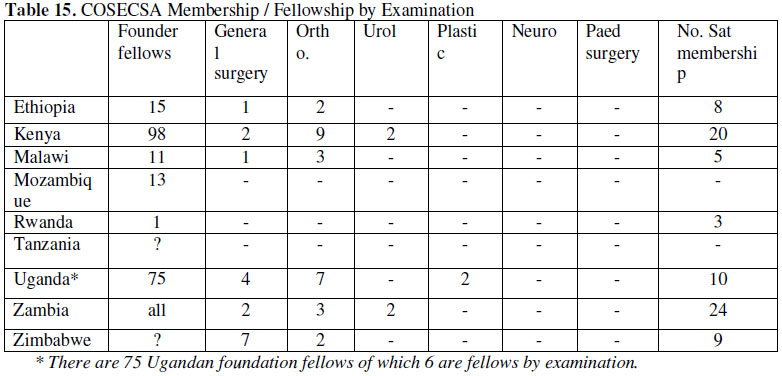{kind=link}
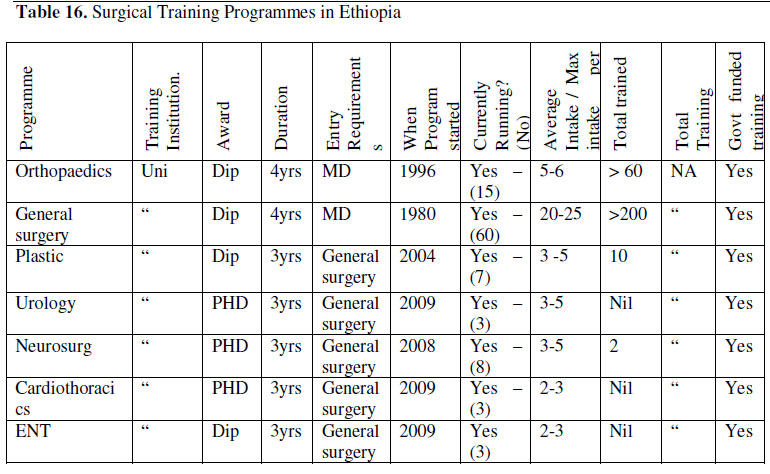{kind=link}
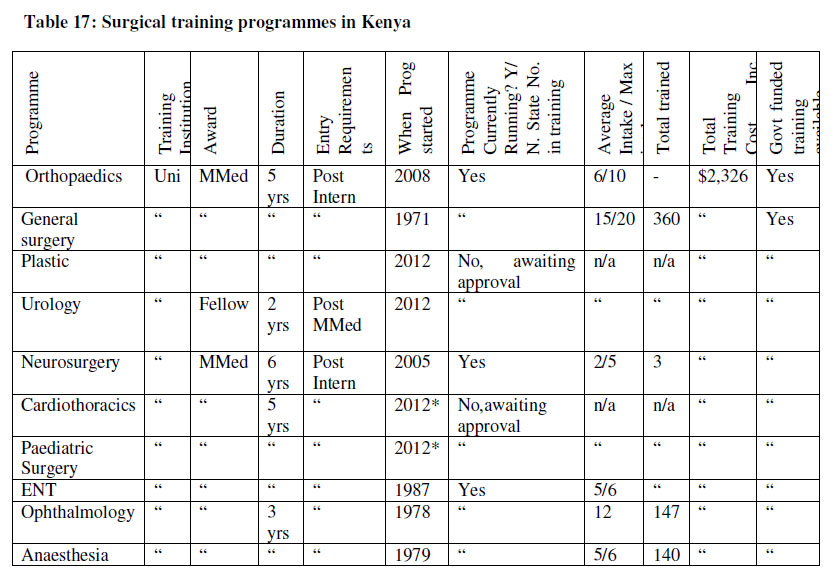{kind=link}
{kind=link}
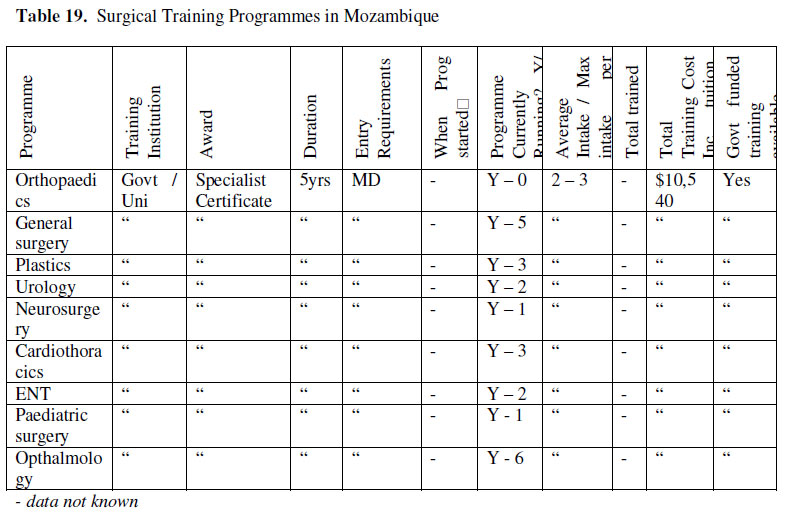{kind=link}
{kind=link}
{kind=link}
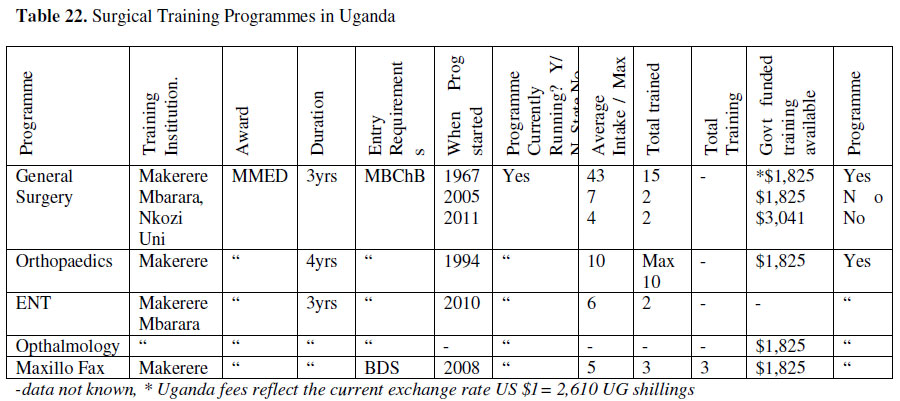{kind=link}
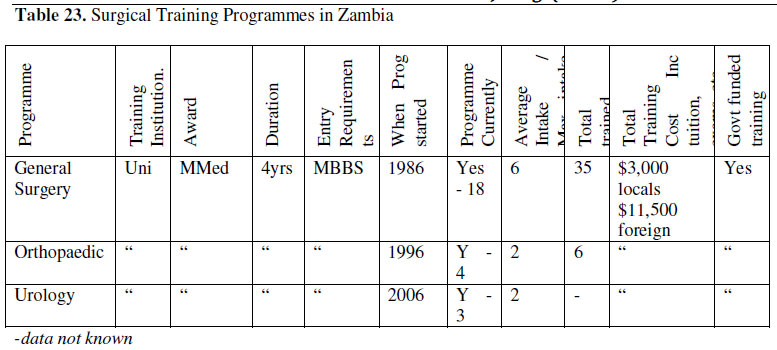{kind=link}
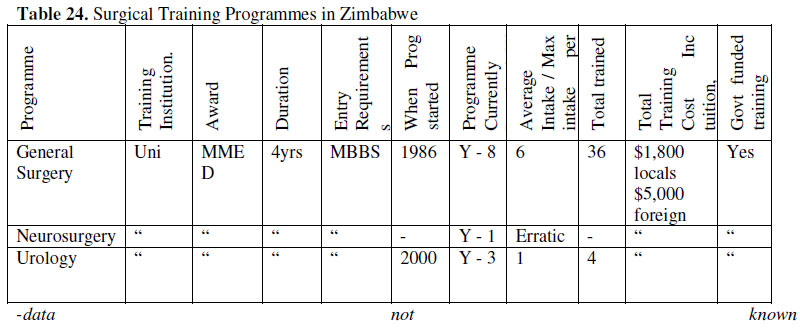{kind=link}