 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
The Epidemiology of District Surgery in Malawi: a Two Year Study of Surgical Rates and Indices in Rural Africa P.M Fenton Formerly
Professor and Head, Department of Anaesthesia, College of Medicine, Malawi.
1986-2001 This article originally appeared in 1997 and is being republished as the original version is not available online. Code Number: js11048 Background: The
true surgical requirement of a rural African population is not precisely
known. Introduction Surgical output in developing countries has been extensively reviewed by Nordberg and others1-5. The general conclusions have been that there is insufficient statistical data from African countries on rural surgical practice, that district surgical services are inadequate and inconsistent and that large scale, population-based surgical output in Africa do not exist. The true surgical requirement of a rural African population is also not precisely known, but based on western on western practice of surgical need, estimates of the proportions of people who get adequate treatment compared to those who do not have varied from 1 out of 6 for inguinal hernia to less than 1 out of 10 for caesarean section2. In urban areas of Africa the commonest scenario, in the author’s experience, is one of decaying services in the large government hospitals with increasing amounts of surgery being carried out in an unmonitored, informal private sector with no output figures available. International comparisons of population-based surgical output show considerable disparity between rich and poor countries. Studies of all surgical procedures performed per 100,000 population per annum have ranged from 8,2536, 1,7697, 1,920 (1972, L Levy, personal communication) in Zimbabwe to 1248 in rural Pakistan. Estimates for the United Kingdom (UK) are around 5,000 procedures per 100,000 per annum1. Based on random examinations of ambulant people in an African population, Levy9 has counted over 5,000 conditions amenable to surgical correction per 100,000 (1 in 19). A 1990-91 study in Kenya recently reported a rate of 263 major operations/100,000 5. Rates of surgical output from Malawi, in southern central Africa have never been reported. In this densely populated country of 11 million people, health and economic indicators are among the least favourable on the continent10. The population growth is estimated at 3.2% per annum. As elsewhere in Africa, surgical services are concentrated in a few overcrowded urban referral hospitals. In 1989, 70% of all surgery in the most populous Southern Region was carried out in just two urban hospitals out of the ten facilities with operating theatres11. In contrast to this centralisation of surgical activity, approximately 90% of the population are impoverished rural dwelling subsistence farmers who have limited access to transport and live far from the urban areas. A single patient referral has been estimated to cost 50 times the annual per capita expenditure on health12. The mean distance of patients from a district hospital is 21km and two thirds of all women live more than 12km from a district hospital (National Statistical Office, 1994). While there may be significant transfer of surgical patients from district to central hospitals it is more likely that rural patients generally do not seek or receive as much surgical treatment as urban patients. These factors have been considered 3,9. If, as we will show, the great majority of major operations in the district are obstetric-related, a centralised surgical service may be expected to increase maternal mortality (estimated in Malawi in 1992 at 40913 and 62014 deaths/100,000/year). A centralised service also has negative effects on the family and society due to referrals of mothers away from the home district for surgical treatment. The objectives of the study were to determine the rates of surgical output for the rural population, to compare rates between individual hospitals and to propose a realisable target figure for rural surgical output. In addition, various indices of surgical activity were examined to identify where surgical services were weakest. Comparisons were made with the types and numbers of operations performed at the country’s largest hospital, Queen Elizabeth Central Hospital, Blantyre. This 950-bed facility resembles a large district hospital more than a referral centre of excellence, having mostly patients from rural areas or townships of low socioeconomic status. Surgical presentation and management is generally similar to that of the population in the study. While the fact of low surgical output is well known, this study aimed to quantify the low level of African output. Contemporary trends in health service development in Africa have for more than two decades emphasised the preventive sector; a surgical service is relatively costly in terms of manpower and consumables and, with the current severe budgetary constraints, it is certain to suffer decline. However, the absence of any comprehensive, population-based figures on surgical output means that if, indeed, such a decline exists, it will not be reported. Within the traditional, Western-based, divisions of the curative services, Government-sponsored surgery may thus become quietly sidelined as a health activity in Africa.The author’s own travels in neighbouring states have shown some surgical services in a state of near terminal decline. There is anecdotal evidence that this process is well advanced in other African countries15. Methods Eighteen District Hospitals (14 Government and 4 Mission) were selected on the basis of their widespread location to cover as much of the country as possible. With the exception of hospital F, all data were personally collected by the author direct from the theatre operations book. The classification of cases as “major” or “minor” was based on the existing system of logging cases. Most operations classified as “major” were procedures such as inguinal hernia repair, caesarean section, laparotomy and limb amputations (also called level II operations)7. “Minor” operations (level I) were typically uterine evacuation, operations for hydrocele, tubal ligation, cataract extraction (under local anaesthesia), suturing and abscess drainage. This differs from classifications in other reports which have included tubal ligation, hydrocele operation and lens extraction as major cases and which would therefore given an increase in the reported number of major cases compared to Malawi5. Hospitals were visited at three to six monthly intervals throughout the duration of the project. The following data were collected for eight consecutive three-month periods from September 1993 to August 1995:
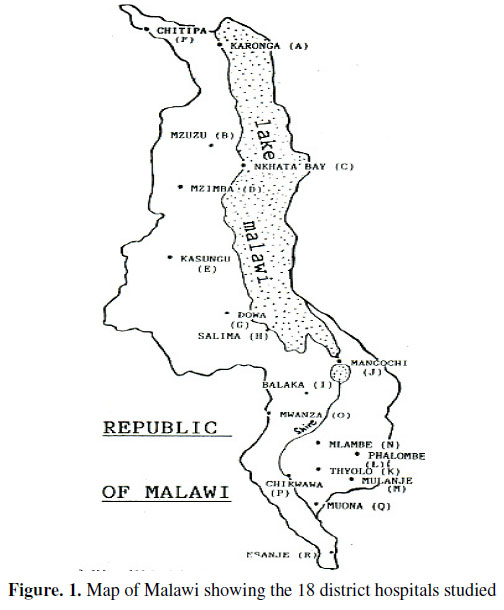
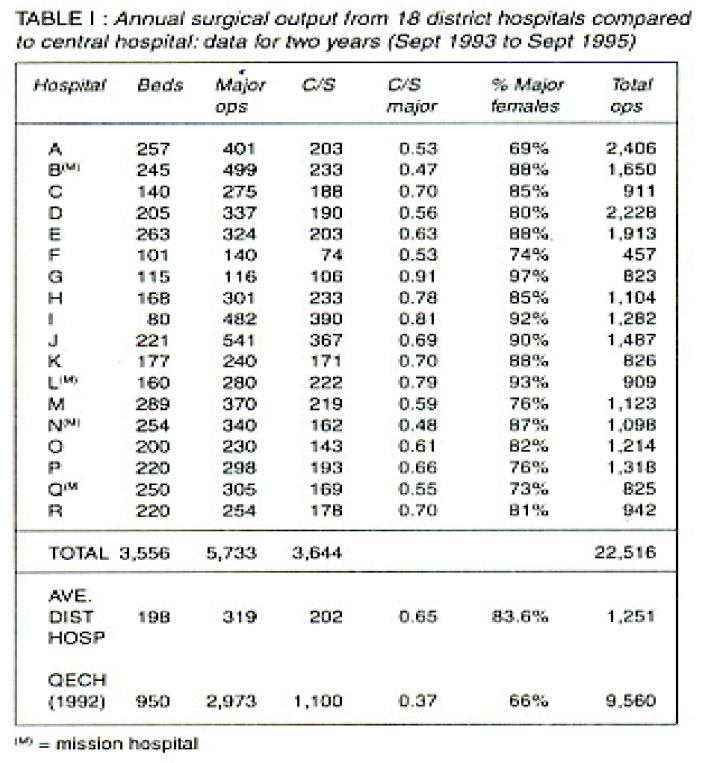
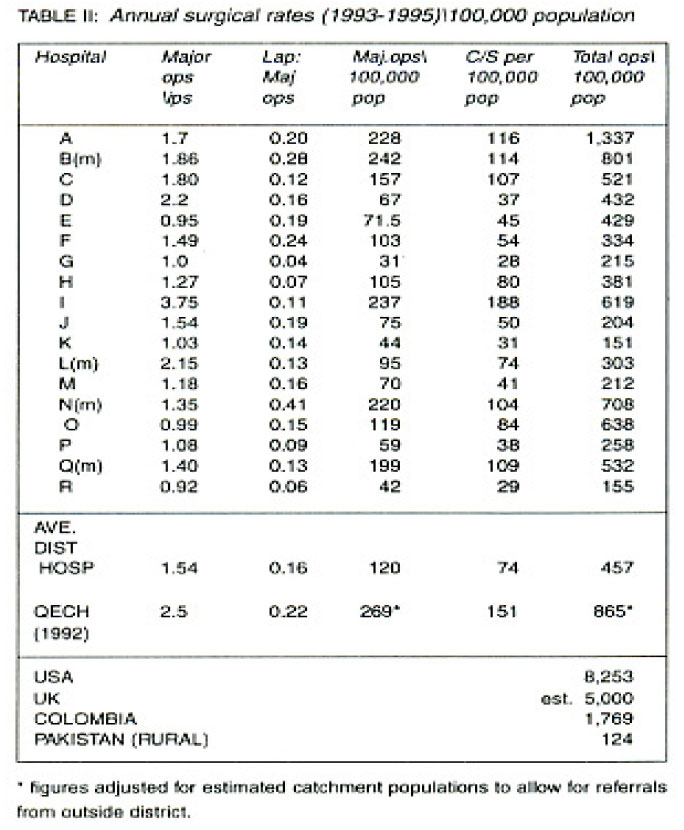
A higher than 50% incidence of ketamine administration (as a sole anaesthetic agent) was arbitrarily chosen by the author to indicate that either the anaesthetist was not trained in other techniques, or was not utilising his training fully or that equipment for alternative techniques, such as oxygen source, means of ventilation, anaesthesia vaporizers, etc., was lacking. Populations were based on the 1987 Malawi census and extrapolated to deduce the population on each occasion of data collection using the official growth rate of 3.2%. The total 18-hospital catchment area population was 5,911,000 at the start and 6,295,000 at the end of the study (average 6,100,000). In-patient populations were obtained at the time of each visit from the administration, usually based on nurses’ daily reports. In the absence of these reports, in-patient populations were estimated by the author by multiplying the known number of beds by a factor based on the number of floor beds noted during a brief tour of the wards. Only four hospitals in the study had bed occupancies less than 100%. Where two hospitals shared the same district, separate non-overlapping estimates of their respective catchment populations were made based on available local hospital data. Results A separate study of referrals to Queen Elizabeth Central Hospital (QECH) showed that of 279 patients chosen at random having major general and gynaecological surgery, 34% were from outside Blantyre District. However, only 5% of CS performed at QECH were referred from elsewhere. Therefore, for the purposes of comparing major general and gynaecological surgery at QECH to the districts the Blantyre population of 729,000 was multiplied by the factor (1 +34/66) to become 1,105,000. For comparing population-based CS rates, the actual Blantyre district population was used as a close enough approximation. The locations of the 18 District Hospitals studied are shown on the map (Figure 1). During the study period 45,032 operations were performed at these hospitals of which 11,466 were classified as major procedures. Of these major cases, 7,288 were caesarean sections (63.6% of all majors). For a mean catchment population of 6,100,000 this gave an annual average surgical rate (1993 to 1995) of 369 per 100,000 for all procedures, 94 per 100,000 for major procedures and 60 per 100,000 for CS. All major procedures could be accurately tabulated. However, minor operations were often not properly described, nor recorded in an available source, or were performed outside the theatre with no record at all. Individual District Hospital surgical outputs and indices were cumulated over two years and expressed as annual output and rates/100,000 population. The 18 District Hospitals can be compared with each other and with the Central Hospital, QECH, in Table I and Table II. (The data for QECH were gathered over one year in 1992/3). These data show that there is great variation in surgical rates between individual district hospitals. Some newer district hospitals had indices that resembled the specialist central hospital. Older hospitals had the lowest rates. Caesarean section The average rural rate for caesarean section was half that at the central hospital. Even allowing for possible excessive intervention during labour in a central hospital, many mothers in the district apparently do not get operative delivery when it is required since, when extrapolated for the whole Malawi rural population of about 10 million people, the district CS rate of 60 per 100,000 population represents only 6,000 CS carried out. Using the central hospital CS rate of 151 per 100,000, there is a shortfall nationwide of up to 9,000 operative deliveries, depending on the ratio of urban to rural populations. Considering that large, unknown numbers of women deliver at home without medical attention, the significance of this figure is an interesting matter for speculation. Does it truly represent that number of obstructed or haemorrhaging labours which receive no intervention during a village confinement? The reduced CS rate can be considered alongside the current rate for maternal mortality in Malawi of 620 per 100,000 live births which approximates to 2,500 maternal deaths (based on WHO data for the birth rate). If there is a 9,000 deficit per annum in CS performed, many of which will result in the death of the mother, it represents a four fold increase on the measured maternal death rate. A recent study in Zimbabwe has examined this association in more detail 16. On the other hand, a high ratio of CS:majors should identify hospitals where the surgical service is not functioning well, since women in labour destined to have CS are more likely to find their way to hospital from far away and, once admitted, the operation is more likely to be carried out, compared to patients needing correction of general surgical problems which may pose diagnostic and management dilemmas, both at the community level and to health workers. Thus a high value of CS:majors coupled with low overall rates for major surgery indicates an inadequate service. Laparotomy The average ratio of lap : majors for all district hospitals was 0.14. The range was 0.03 to 0.52. At hospitals where this ratio was low, CS was almost the only major surgical activity and overall rates were also low. This index correlated adequately (r=0.515. p=0.02) with major output and serves as a convenient method of assessing hospital performance in surgery where data on catchment populations may not be available (Table II). Major surgery on women The percentage (% major:females) was also determined. An average 85.6% of all major surgery was carried out on women. Apart from CS, virtually all these cases were laparotomy for ruptured uterus, ruptured ectopic or drainage of peritoneal pus. Use of Ketamine anaesthesia Methods of anaesthesia were usually poorly recorded as either “GA”, “LA” or “Ketamine”. At nine hospitals there was a higher than 50% use of ketamine as the sole anaesthetic agent. Of these nine hospitals, five had no trained anaesthetist. All hospitals where less than 30% of cases were done under ketamine had a trained paramedical anaesthetist in post. Personnel performing surgery The status of the ‘surgeon’ was as follows: 0.8% of all surgery was performed by visiting specialists, 8.2% by the District Health Officer and 75% by paramedical Clinical Officers or Medical Assistants. An average of 16% of all operations were performed by medically untrained theatre workers (range 0 — 75%), though these cases were confined to suturing and incision and drainage. In six hospitals, all surgery was carried out by non-doctors. Personnel giving anaesthesia All anaesthesia was given by paramedical cadres and no case using general anaesthesia or ketamine was recorded as being given by untrained staff such as a theatre servant Discussion District Hospital surgery in Malawi The average district rate of major procedures in Malawi was 94 per 100,000 population (range 21 - 242) which is considerably less than that reported from Colombia (1,285 majors per 100,000) in 1974. The 1972 Zimbabwe (then Rhodesia) rate of 1,920 total operations per 100,000 may be assumed to comprise at least 500 major operations per 100,000, some five times the rate in Malawi today. Current rates in Zimbabwe are not known. From other large population-based studies, the only reported rate lower than Malawi was from Pakistan where about 50 major operations per 100,000 were performed in 1983. Allowing for the different methods of classifying major operations, comparison with published reports from Kenya and Tanzania shows rates to be between 50% and 80% higher in those two countries than in Malawi. Based on the output of the specialist referral hospital, which some newer hospitals approach, the author proposes a target surgical rate of 250-300 major operations per 100,000 population which is an achievable target. At present this figure has about 35% attainment. It is clear that the rural dweller in Africa is still not well served by his or her District Hospital and in the most deprived areas of Malawi, surgical rates are about 2.5% of rates in South America 20 years ago and less than 1% of rates in Europe and North America. The surgery of women Over 80% of all major surgery in the districts was obstetric or gynaecological. Apart from the large numbers of CS, laparotomies accounted for most major surgery and in the district this operation was almost exclusively performed on women for either pelvic infection, ruptured uterus or ectopic pregnancy. This sex bias has been noted elsewhere in Africa5. The few major operations performed on men in district hospitals were almost entirely hernia repairs and trauma surgery. At one peri-urban mission hospital with an active surgical service (hospital “N”), the ratio of lap:majors increased in an almost straight line from 22% to 52% in two years, without a change in other indices. Virtually all these laparotomies were performed on women for one of the three indications above. If this explosive increase in surgical work at one hospital represents a genuine trend, it serves as an indicator of the future pattern of African surgery. An associated statistic, the Maternal Mortality Rate, has been noted in Zimbabwe to have increased by 200—300% in just two years17. The high prevalence of AIDS and the failure of population control measures are undoubtedly significant factors responsible for the current increase in female major surgery in Malawi. Other laparotomies (eg for bowel obstruction) are common at the Central Hospital (77% of all major general surgery at QECH in 91/92 were laparotomies) but rarely performed in the district. Such cases that do present at District Hospitals are usually referred away, but the numbers of successful referrals do not match the expected incidence of these conditions in the district. The presumption is that these predominantly male cases die outside the hospital for lack of an operation. Surgical facilities The difference in output between different District Hospitals was much greater than any difference between the best District Hospital and the Central Hospital. The great discrepancy between numbers of operations carried out at different hospitals is only attributable in small degree to patient referrals: in the majority of cases the operations are simply not done. The age of the hospital was the most significant factor in this respect. The level of activity was also determined by resources such as staff levels and interest in surgery, equipment and hospital budgets as well as local perceptions among the population about the efficacy of the hospital and the acceptability of surgery itself as a cure for disability and disease. The current building programme of new district hospitals should eventually produce a more equitable distribution of surgical services. However, even new, efficient District Hospitals such as Hospital D have very low population-based rates due to their location serving a large but scattered population without access to transport. Clearly, the distance of the patient from the surgical facility is at least as important as the effective internal functioning of the hospital. Given the overwhelming preponderance of female surgical patients and the relative uniformity of their surgical and anaesthetic management, the building of many scattered, smaller units with a capability aimed at obstetric surgery and anaesthesia would seem to be the simplest and most effective solution to the problem of low surgical rates in Malawi. Malawi’s very high Maternal Mortality Rate would fall concomitantly. This strategy, however, would cause male major surgical rates to fall yet further. Doctors as surgeons Our results carry clear implications for the training of district surgeons in order to meet the lowest level of demand. Basic surgical skills in a limited number of straightforward procedures should be conferred as widely as possible to paramedical practitioners. Malawi already depends on this cadre for the performance of most surgery at district level 18. The only remaining area of controversy is to what extent Malawian hospitals should aspire to something above the lowest level, for instance to meet the presumed requirement for male laparotomy that is not being met at present. Doctors at the District Health Officer level appear to have two important roles in sustaining a surgical service: they may be keen (though untrained) surgeons and they have an important supervisory and disciplinary function in logistics and administration. Although surgical outcome proved difficult to assess and was not reported in this study, most hospitals showed that the basic major surgical requirement for women appeared to be adequately met without any doctor ever appearing in the operating theatre, except in the guise of an administrator. A belief widely held among surgeons and health manpower planners in Africa, however, is that the way to increase the amount of surgery available to the population is to train only doctors as surgical specialists. Surgical rates from Kenya 3,4 (where such a philosophy prevails), when compared with those from this study show that this is almost certainly fallacious: rates for CS from one well-staffed mission-supported Kenyan district hospital are similar to those for the average Malawi Government district hospital where only 0.8% of the surgery is performed by specialist surgeons (72 and 74 per 100,000, respectively). In the same report, the ratio of lap: majors is higher where doctors practice (0.29 cf 0.14) and the ratio CS:majors closely correlates to the same index from the specialist-staffed Central Hospital in Malawi, QECH (0.36 cf 0.37), both indices demonstrating a wider surgical repertoire where doctors are surgeons. The average Malawi district CS: majors ratio was 0.65 (range 0.48-0.97). In these studies, however, the CS:majors and lap:majors index differences between doctor-surgery and non-doctor-surgery was mainly due to increased numbers of hernia repairs, an operation that hardly justifies extensive specialist surgical training. Notwithstanding all the above, one would generally expect that the appointment of a surgical specialist would improve the service, especially in the field of general surgery. The pertinent questions in this era of emphasis on “Safe Motherhood" appear to be: By how much? For which patients? and: Can Africa afford or sustain it? Conclusions
Acknowledgement The author thanks the Trainee Anaesthetic Clinical Officers (TACOs) who gathered the QECH data for 1 year in 1992/93, Mr. Cyril Goddia, ACO, who collected the data at Chitipa District Hospital and Prof. Malcolm Molyneux who did the statistical analysis. Funding The Malawi Anaesthesia Support Project from 1993 to 1996 was funded entirely by the British Overseas Development Administration (ODA) as part of its development aid to Malawi. References
Copyright 2011 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js11048t2.jpg] [js11048t1.jpg] [js11048f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}