 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 16, No. 3, Nov/Dec, 2011, pp. 45-50 Prehospital and First Health Facility Management of Patients with Severe Musculoskeletal Injuries in Uganda T. Otieno1, J. Phillips2,3, B. Mbonye1, T. Beyeza1, E. Naddumba1 1Department of Orthopaedic Surgery, College of Health
Science, Makerere University, Kampala, Uganda Code Number: js11049 Background: There
is a dearth of evidence outlining the state of prehospital and first health
facility care of the musculoskeletal injury patients in Uganda. Further
documenting the current impediments in prehospital care may provide a basis for
prioritizing interventions aimed at improving the system. Introduction Injury has become a major cause of morbidity, mortality and economic loss, resulting in 5 million deaths, accounting for 10-11% of global mortality and 13% of all disability adjusted life years (DALYs)1-3. Major causes of injury in contemporary Africa have been identified as, first and foremost, road traffic accidents (RTAs), then falls, assaults, and blast injuries4-10,23. RTAs alone are estimated to account for 20-50 million disabling injuries around the globe, with an overwhelming proportion of these injuries requiring orthopaedic management. The incidence of RTAs is predicted to rise as developing countries undergo rapid motorization, taking to ill prepared roads with cheap and readily available second hand vehicles2. In Uganda, injury has been shown to be amongst the top six causes of death. Countrywide it is estimated that 2000 deaths per annum are attributable to RTAs, and in metropolitan Kampala, 39% of all injuries are the result of RTAs19. The prime contributors being accidents involving boda boda motorcycles and omnibuses, the predominant modes of taxi transport. Kigera et.al21 reported that 62.5% of the annual budget allocated to Directorate surgery at Mulago hospital goes to treat boda boda injuries alone. The aim of prehospital emergency medical services is to ensure expeditious delivery of a live, safe, and comfortable patient to the in-hospital trauma team without causing secondary injury6,12,13,14. Early management of musculoskeletal injury (MSI) in the field and at lower level facilities can significantly impact patient outcomes. Prompt detection and appropriate management of limb fractures and dislocations with the application of splints, simple reductions, administration of analgesics and antibiotics is critical14-16. Early immobilization in patients with high risk for spine injury is mandatory to prevent exacerbation of existent spinal cord injury during extrication, initial treatment and transport5,13,16. Effective advanced communication of the nature of the injury and anticipated emergency interventions necessary is crucial in enabling the in house team to adequately prepare for an incoming patient4,11. Uganda has no formal prehospital emergency system in place and care at lower level facilities varies considerably. Responsibilities of prehospital care have been left to the police, taxi drivers, patient, family, and well wishers. With the global health burden of injury on the rise, optimizing existing systems and encouraging developing economies to invest in this sector will be necessary to mitigate increasing morbidity and mortality. Through a structured questionnaire we sought to further evidence the current status of prehospital and lower level first health facility care delivered in Uganda to musculoskeletal injury patients. Subjects and Methods A cross sectional descriptive analysis was undertaken. Between November 2006 and January 2007, all MSI patients presenting to the Mulago Hospital Accident and Emergency Unit (MHAEU) within the first 24 hours after injury were enrolled in the study on arrival. The study design, consent forms, and assessment tool were approved by the institutional review board at Makerere University prior to initiation. A structured questionnaire was designed under the direction of the chief of the Department of Orthopaedic Surgery at Mulago Hospital. Patients were consented for participation at time of arrival. In the case that a patient was incapacitated, the patient’s guardian was consented. Questionnaires focused on socio-demographic, injury data, and eight content areas deemed important in the delivery of prehospital/first health facility care. It is available upon request from the corresponding author and included.
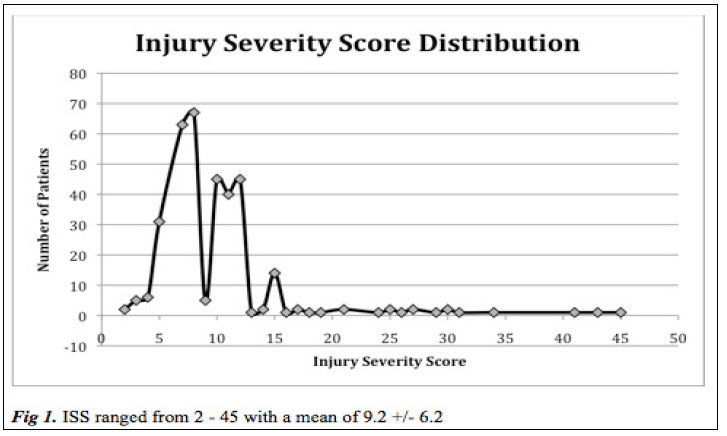
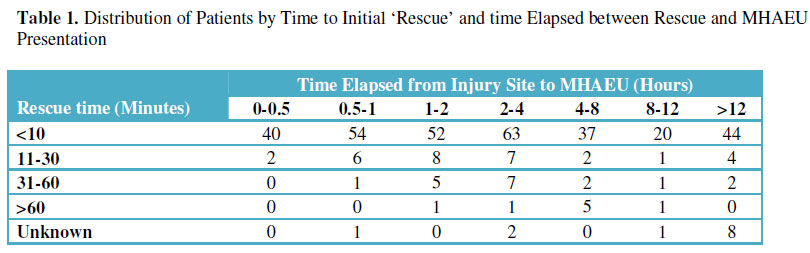
Results A total of 378 patients were enrolled over the study period. Males accounted for 296 (78.3%) of those enrolled. The mean age was 28.5 years (SD+/-13.66). The youngest patient enrolled was 3 months and the oldest 78.0 years. Patients aged between 20 to 40 years accounted for 60.8% of all those studied. Road traffic crashes accounted for 66.1% of all injuries. Other common causes of injury were falls (16.1%), assaults (6.9%), falling objects (6.3%) and missile injuries. Less common causes included occupational and sports injuries. ISS ranged from 2 to 45 with a mean of 9.2 and standard deviation of 6.2 (Fig 1). Interval between injury time /site to presentation at the MHAEU ranged from 10 minutes to 24 hours with 104 (27.5%) patients arriving within one hour following injury (Table 1). Of those who initially presented to first health care facilities, 24 (15.3%) arrived at MHAEU within 1 hour of injury, 57 (36.3%) in 1-3 hours, 36 (22.6%) within 3-12 hours and 39 (24.8%) arrived >12 hours status post injury occurrence. Prehospital assessment, bleeding control, and resuscitation A total of 56 (18.4%) of the interviewed prehospital caregivers made an attempt to assess the patient at the time of rescue. Of those assessed, 3 were reported to have breathing difficulty at the scene. In 206 patients, caregivers reported obvious bleeding wounds. In 61/206 (29.2%) there was an attempt to arrest active bleeding. Intravenous fluid infusion of 0.5-2 litres was administered to 43 (11.4%) patients. All were patients who had first presented to other health facilities. No patient arriving at the MHAEU direct from the accident scene received intravenous fluid (IVF) resuscitation in the prehospital period. Of the patients who had IVF initiated in the pre-hospital period, only 4 (1.1%) presented with venous access in place. Spine precautions Not a single patient had cervical-spine immobilization in place before or during extrication from the scene of injury. On presentation to the MHAEU, 323 (85.4%) were found to have an indication for spine precautions, 64 patients having relative, and 259 (68.5%) having absolute indications based on nature and severity of injury and clinical findings.Of those with an absolute indication for spine protection, those who required cervical spine, thoracic and lumbar, or whole body protection were 66 (25.5%), 50 (19.3%), and 143 (55.2%) respectively. At the time of presentation 2 patients had a cervical-collar in place. Of the 259 with absolute indications for spine protection, 16 had a vertebral column fracture or dislocation, while 12 had a serious neurological deficit (paraplegia or quadriplegia or paresis) and 21 died soon after arrival. Worsening neurological deficits in the prehospital period were reported to be 10 of the 12 patients who presented to MHAEU with paraplegia, quadriplegia or paresis. Fracture management Of those with fractures or dislocations initially presenting to outside health facilities, 38 (24.2%) were splinted (Table 2). In case of 333 patients, limb splinting was deemed necessary at the time of presentation to the MHAEU Of those presenting first to an outside health facility, wounds were not dressed, and no antibiotics administered in 28(40.6%) and 47(68.1%) of open fractures respectively. In patients who had not passed through a health facility first, 11 (5.3%) were splinted. 3 (3.5%) open fractures had a dressing applied and none had received antibiotics. Pain management Pre-hospital analgesia was considered adequate in 57 (15.1%) patients, inadequate in 20 (5.6%), and was not administered in 301 cases (79.6%). 80 of 157 (51%) patients presenting initially to an outside health facility received no analgesia. 221 of 221 (100%) patients presenting directly to the MHAEU had not received any form of analgesia in the field. Hospital attendance, transportation and communication Of the 378 patients seen, 97 (25.7%) passed through outside hospitals for initial resuscitation, 60 (15.9%) through outside clinics, and 221 (58.5%) patients presented primarily to the MHAEU. A total of 152 (40.2%) of the patients were transported by means of saloon cars, 97 (25.7%) by means of pickup truck, while only 51(13.5%) of the 378 patients were transported by way of ambulance. Pre-hospital caregivers communicated to MHAEU in advance in only 1.1% of cases (n=4). In 3/4 cases, communication was deemed to be adequate for advanced preparation by the MHAEU team. Prehospital caregiver skill level Ambulance teams, police officers, and laypersons were the lead actors in retrieval and transport of 9 (2.4%), 47 (12,4%) and 322 (84.2%) patients respectively. Of 305 prehospital caregivers interviewed, 73% had no exposure to any form of medical or emergency care training, 11% were policemen with minimal previous training that was not up to date, 14% reported being trained medical personnel while the medical training of 2% could not be accurately established. Of the 305 interviewed prehospital care givers, 124 (40.7%) were patients’ relatives, 44 (14.6%) were immediate friends or neighbors, and 136 (44.7 %) were unrelated to the patients they cared for. Discussion Absence of a well functioning and widely accessible pre-hospital trauma care system leaves unskilled and inadequately skilled caregivers to fill the gap. This unique situation has been observed in other studies7,15 with prehospital care delivered by lay persons in 322 of the 378 cases. It is therefore not surprising that a very small percentage of patients in this study received any form of assessment, resuscitation, or appropriate care in the pre-hospital period. This study revealed that most patients with severe musculoskeletal injuries were in their most productive years with 60.8% being aged between 20-40 years while the most common cause of injury was RTAs accounting for 66.1% of injured patients seen. From the economic perspective, the importance of minimizing the long-term sequelae on these wage earners and breadwinners cannot be overstated. Further, the financial strain on the healthcare system is significant. Improved prehospital management may shorten hospital stays and reduce systemic costs. The majority (82.0%) of the patients were “rescued” within 10 minutes after injury. Though not a single patient received a full complement of the basic interventions expected in the prehospital period, to include an assessment of respiratory status, airway protection, monitoring and assistance, bleeding control, IV access; spine precautions and wound care4 This absolute deficiency in pre-hospital care was noted in 245 patients who were “rescued” by lay caregivers and 47 cared for by policemen, but was also observed in a very small percentage of patients attended to by “health professionals” in the field. Only a very small proportion (1.1%) of patients had ongoing IV access or intravenous fluid (IVF) infusion instituted (11.4%) in the first health care facility with 98.9% of all patients presenting to MHAEU without ongoing access or resuscitation. The low rate of resuscitation in this cohort potentially may have led to adverse outcomes. Without clinical outcomes data, and a large enough number of patients receiving resuscitation for a comparative analysis, we can only speculate as to the scope of the clinical impact. Though with a mean ISS of 9.2 and 206/378 patients with bleeding injuries, likely there were a significant number that may have benefited from early fluid resuscitation. This observation may be due to inadequate skills and material resources, though poor work ethic with little accountability may explain some pre-hospital caregivers’ failure to provide better care in a resource constrained setting. Lack of spine protection in spine injury victims can lead to worsening of neurologic injuries, which often are irreversible. The two (0.3%) patients with indication for spine precautions and a c-collar in place were evacuated from the injury site without any such protection and only later had the collar applied at a lower level facility. Hasty extrication, non-uniform transport, and spine precautions not observed throughout the process may have had a significant detrimental impact on the clinical outcomes of these patients. Twenty-one (52.5%) patients of the forty whom later died, had a neurological deficit or a vertebral fracture and had passed through a lower level facility prior to MHAEU. Only 24.2% of fractures first seen at outside health facilities arrived at the MHAEU splinted. With various options available, even in a significantly resource constrained setting, for the most basic of improvised splints, there is little reason, other than to expedite the transfer of a critically injured patient to a higher level of care, that a known fracture should not be splinted. Splinting provides a means to decrease pain, prevent potential neurovascular damage, and avoid further soft tissue damage. Considerably fewer (5.3%) of those initially seen by lay persons had any form of splinting attempted. Contrary to our expectation, analgesic administration occurred in none of the patients arriving direct from the field as most were initially seen and transported by lay providers. Severe trauma with significant emotional stress can result in post traumatic stress disorder in up to 40% of major trauma patients20-21. Adequate pain control in significant trauma likely will require opioid analgesics, which carry significant inherent cardiopulmonary risk. Until the prehospital system is further developed with well trained providers, the cost/benefit ratio of administration opioid analgesics in the current prehospital environment will likely favor their disuse. The mode of transport used affects the quality of prehospital intervention; time to hospital; and safety and comfort of patients while en-route. It is therefore a key factor in being able to provide early intervention and improve clinical outcomes. Only 13.0% of patients studied arrived at MHAEU by way of ambulance, with the rest (including 74% of those who had passed through other facilities) arriving via other less desirable methods. Exacerbation of spine injuries in patients forced to sit up right or slumped into the back of pickup trucks without rigid back support may have occurred. The basics of trauma care, placement of peripheral lines for IVF resuscitation, and rigid back support could be provided in an ambulance while not in other modes of transport. Prehospital communication occurred in a minimal number of the injury cases in this study. Advanced communication allows the in house team to prepare personnel and equipment to provide optimal care. It also avoids the chaotic service disruptions in other ongoing patient care that can occur with the unannounced delivery of a critically injured patient. In this study, the arrival of only 4 (1.1%) patients were announced in advance. 3/4 were considered adequate to facilitate prior preparation. With the widespread use of cellular communication, especially in metropolitan Kampala, advanced communication could be more readily practiced if a direct number to the MHAEU was widely known. Conclusion This study adds further evidence to document the current status of prehospital care in Uganda. Significant deficits in care provided are noted throughout each of the 8 areas under scrutiny. It echoes the findings of other studies in developing countries, identifying the frequent use of unskilled or poorly skilled persons with inappropriate equipment and transport, in administering prehospital care17-18. The most appropriate way forward may be targeted training of selected laypersons to fill the gap in prehospital care. Previous investigators have shown that a context-appropriate, 1-day, basic first-aid course for lay responders can be implemented in Uganda23. If targeted appropriately the knowledge gained from such a course may prove beneficial in improving upon the current status quo of prehospital care for the musculoskeletal injury patient. References
Copyright 2011 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js11049f1.jpg] [js11049t1.jpg] [js11049t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}