 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Wilms’ Tumour: Experience in a Developing Tertiary Centre in Nigeria R.I .Osuoji, O.M.Williams, O.T.Ajai, O.C.Idika, A.A.Abolarinwa, M.A.Bankole Department of Surgery, Lagos State University Teaching
Hospital, Ikeja, Lagos, Nigeria. Code Number: js11050 Background: Children
with Wilms’ tumour present early in the developed countries with
correspondingly good prognosis. The same however is not true in the developing
countries where the patient present rather late. This study evaluates the
impact of late presentation on the management of childhood Wilms’ tumour in our
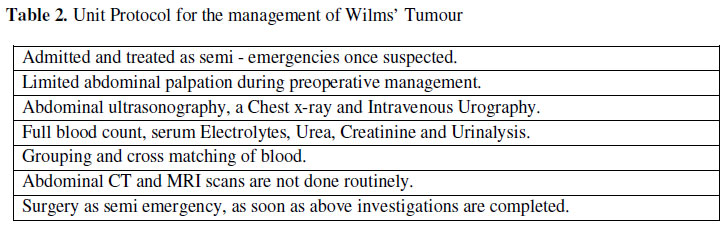
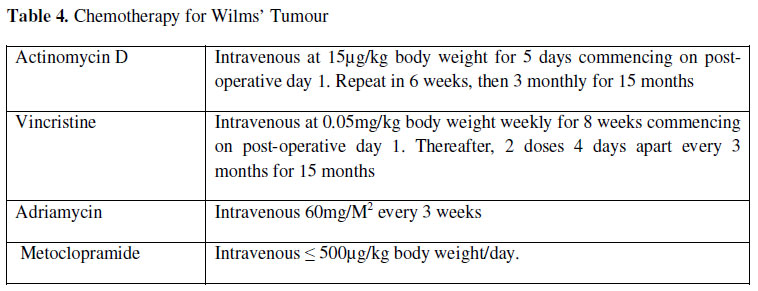
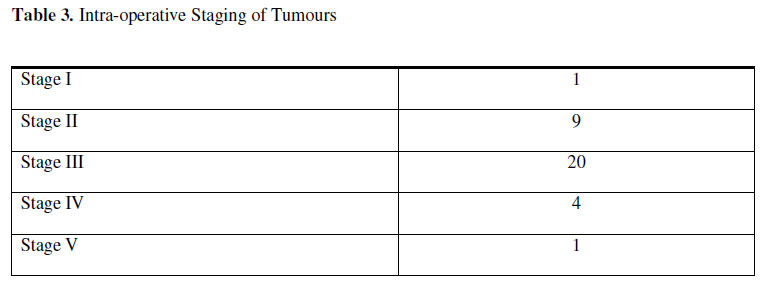
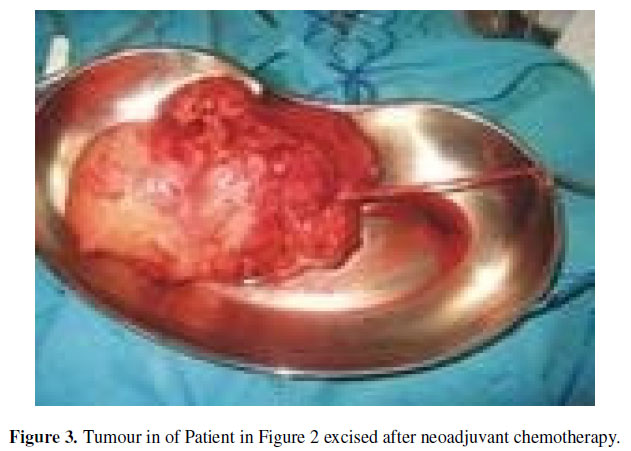
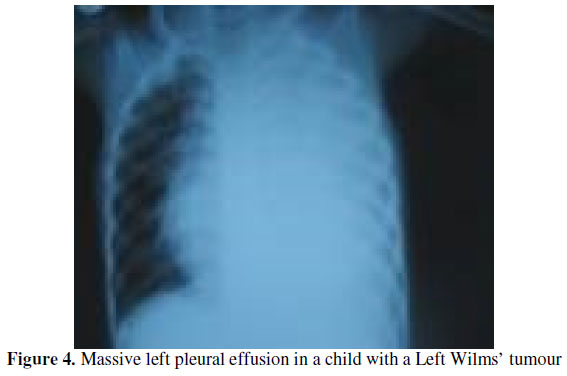
environment. Introduction Wilms’ tumour is the most common abdominal malignancy in children in Sub-Saharan Africa1. It is an embryonal tumour of the kidney that may contain the 3 germ cells: the stroma cells, the blastema cells and the epithelial cells in various combinations. If they contain the 3, they are termed triphasic, if they contain 2, they are diphasic, and monophasic if they contain 1 germ cell. Recent advances in technology coupled with a significant increase in the level of health awareness among the populace have made it possible to diagnose and treat Wilms’ tumour early in developed societies.This, in effect impacts positively on the prognosis in such societies. Two years survival of stages I and II Wilms’ tumour is about 90-95% and about 75%for stages III and IV disease2. The aim of this retrospective study is to assess how we have fared with these patients that presented late to our unit in a Sub-Saharan region. Patients and Methods This was a retrospective study of children aged 0-15 years who underwent nephroureterectomy for histologically confirmed Wilms’ tumour from January 2004 to December 2010, at the Lagos State University Teaching Hospital, Lagos, Nigeria. This hospital is a referral centre for the most populous geopolitical zone of South Western Nigeria. There were a total of 35 patients and all their case notes were available for analysis. Of the 35 cases, 21 patients were males and 14 were females (M: F=3:2). Their ages ranged from 6 months to 13 years with mean of 3.4years. The duration of symptoms prior to admission ranged from 2 weeks to 8 months with a mean of 3.5 months. Table 1 shows the presenting symptoms. Table 2 shows protocol for the management of suspected Wilms’ tumours in our unit. The haematocrit of patients seen ranged from 22% to 39% on presentation with a mean haematocrit of 29.5%. Patients were transfused intraoperatively as required and before adjuvant chemotherapy. Abdominal ultrasound was used to rule out other causes of renal enlargement in this age group, indeed 3 cases were initially misdiagnosed on abdominal ultrasonography as multicystic lesions, hydronephrosis, and renal abscess. An abdominal CT scan was done in 1 patient and it showed an infiltration of the inferior vena cava and para-aortic lymph nodes with a nonfunctioning left kidney. Intravenous urography showed non-functioning ipsilateral kidney in 6 patients and calyceal distortion in 2, others were not stated in the case files. Operative Technique All our patients had a laparotomy under general anaesthesia administered by qualified and competent paediatric anaesthetiologists. Under general anaesthesia in a supine posture after urethral catherisation, the abdomen was cleansed with antiseptic solutions, an extensive transverse supraumbilical incision was made and the incision was deepened to gain access into the peritoneal cavity. Once in the peritoneal cavity, we inspected the liver for the evidence of metastases, we made efforts to palpate the normal contralateral kidney first. But because most of these tumours are really huge, this maneuver is left to the end. In a right sided lesion, the ascending colon which is usually displaced medially and upwards is held with Babcock tissue forceps and a vertical incision is made laterally. As this area is usually avascular, a blunt dissection is achieved with a swab on a stick. The renal pedicle is approached towards the midline. We try to mobilize the renal mass making sure there is no tumour spillage (If it is not possible to mobilize the tumour, an incisional biopsy is done and the abdomen is closed). The next step is to identify the renal pedicle in the midline, look for the renal artery which is posterior to the renal vein and ligate it first before ligating the vein. The ureter is ligated at the vesicoureteric junction to complete the nephroureterectomy. The para-aortic nodes are biopsied if any are present. Some of these tumours could be very large, displacing the renal pedicle. In that instance, we try to ligate the ureter first and trace it up to the renal pedicle and indeed the displaced renal vessels. For left sided tumours, the maneuver is basically the same except that the involved segment of colon is usually the descending colon. We irrigate the operative site with sterile water before closing the abdomen. We usually do not drain the abdomen. All specimens were sent for histopathological examinations done by qualified pathologists. All patients had adjuvant chemotherapy commencing on the 1st postoperative day (see Table 4 for our unit’s protocol). The only 6 month old child with a stage I Wilms’ tumour did not receive adjuvant chemotherapy Results The intra - operative staging is illustrated in Table 3. The only child with a stage I disease had a fulminating recurrence 6 months later and died. This child was not given adjuvant chemotherapy because the lesion was assumed to be a mesoblastic nephroma. Three patients had a laparotomy and an incisional biopsy before the commencement of neoadjuvant chemotherapy (Figures 1, 2 and 3). One patient had a haemorrhagic left pleural effusion. He had a tube thoracostomy (Fig 4) before a left nephroureterectomy. This child died 14 days post operatively. Three deaths occurred intraoperatively from haemorrhagic shock. This included the child with a bilateral tumour. Five patients (14.28%) have completed their chemotherapy and are presumed cured. Two children reacted adversely to adriamycin, showing cardiomegaly confirmed on 2D echocardiography and congestive cardiac failure. Ten patients were lost to follow up while the rest are still in various stages of chemotherapy being followed up with clinical examinations, 3 monthly abdominal ultrasonography and yearly intravenous urography as long as they survived. Discussion Childhood Wilms’ tumour is characterized with late presentation in our setting. Whereas presentation is early in the developed world, presentation is still late in the Sub-Saharan sub-region3. Ekenze et al reported 40 cases of late presentation in a period of 10 years3. Hadley et al4 noted a similar feature of late presentation that was associated with malnutrition. These compare with our 6 years’ experience with late presentation of Wilms’ tumour in 34 children (only 1 child had a stage I tumour). Incidentally this period coincides with the era when medical treatment in children (aged 0-12years) was made free by the state government. Indeed it is still free for that age group. Apart from ignorance, negligence on the part of parents may probably be one of the reasons responsible for the late presentation despite the free medical treatment for this age group in our setting. The consequences of late presentation include very huge and advanced tumours which make operative intervention very difficult and prognosis correspondingly poor. Other factors that might influence the prognosis include; inadequate drug supply (chemotherapeutic drugs are not free in our setting despite the free medical services for this age group) and comorbidities affecting the patient: malnutrition, human immunodeficiency virus/acquired immune deficiency syndrome(HIV/AIDS), tuberculosis4. Although these diseases may affect the prognosis, we did not routinely screen our patients for them. Operating on these patients could be challenging and daunting for the inexperienced even for the experienced surgeon. Firstly, torrential bleeding may be a problem and because the tumours are usually of very large size, considerable amount of blood may be may be lost when the tumour is resected. To minimize this blood loss intra-operatively, the renal artery should be ligated first before the renal vein (which should be ligated later after some minutes interval). This reduces the amount of stroke volume going into the mass5. Besides, ligating the vein later does not worsen the prognosis6. Secondly, because these tumours are usually large, the usual renal pelvis anatomy is distorted, the renal vessels could be obscured and displaced by the large mass, consequently, gaining vascular control becomes difficult7. We overcame this difficulty for the definitive operable cases by first ligating the ureter as low as possible. The proximal portion of the ligated ureter becomes a guide to the renal pelvis which lies immediately posterior to the renal artery. The latter is then ligated before the vein as earlier mentioned. Three patients had neoadjuvant chemotherapy and a subsequent nephroureterectomy. The chemotherapy regime consisted of vincristine weekly for 8 weeks, a course of daily Actinomycin D for 5 days and 2 doses of Adriamycin given 3 weekly. This regime was found to be effective in reducing the tumour mass8,9. Like most cytotoxic drugs, these drugs have their side effects but peculiar to Adriamycin is cardiotoxicity10. Two children had an adriamycin induced cardiomyopathy and the drug was discontinued. One of them died but the other survived with significant heart failure, he is currently out of heart failure. Clearly, this study has some limitations. Firstly, it is a retrospective study with its attendant problems; 10 patients were lost to follow up. Secondly, although there was multidisciplinary collaboration involving paediatricians, paediatric surgeons, paediatric anaesthetiologists and paediatric histopathogist, a paediatric oncologist was not available. Ideally the work up of these patients should include computed tomography (CT) and magnetic resonance imaging (MRI) which characterize the tumours and show the extent of spread. These investigations were not done. We relied on the clinical findings, intravenous urographs and chest x-rays for our diagnosis. Paediatric patients are given free medical treatment in our unit, however this does not include the supply of cytotoxic drugs and the consequence is poor compliance to the chemotherapeutic protocol. Patients did not have radiotherapy. It has been stated that comorbidities like malaria fever, tuberculosis (TB) and human immunodeficiency virus/ acquired immune deficiency syndrome (HIV/AIDS) may affect the prognosis in these patients4. We did not routinely test patients for these conditions. Finally, the histopathologist did not say whether the tumours were either favourable or unfavourable histology. This practice which has since been corrected, robbed us of information of prognostic value during this retrospective study. Conclusion
References
Copyright 2011 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js11050f2.jpg] [js11050f1.jpg] [js11050t2.jpg] [js11050t3.jpg] [js11050f4.jpg] [js11050t1.jpg] [js11050t4.jpg] [js11050f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}