 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 16, No. 3, Nov/Dec, 2011, pp. 58-63 Pyomyositis and its risk factors in patients of Gulu Regional Referral Hospital, Uganda. A Descriptive Cross-sectional Study Design D.L. Kitara1, P.O. Bwangamoi2, H. Wabinga3 1Department of Surgery, Faculty of Medicine, Gulu University, Gulu,
Uganda. Code Number: js11051 Background: Pyomyositis is a suppurative infection of the
skeletal muscles and is characterized by localized muscle pains, swelling and
tenderness. Pyomyositis accounts for 10-15% of hospital admissions in some
units in northern Uganda. We described the demographic characteristics and risk
factors of Pyomyositis patients treated at Gulu Hospital between January to
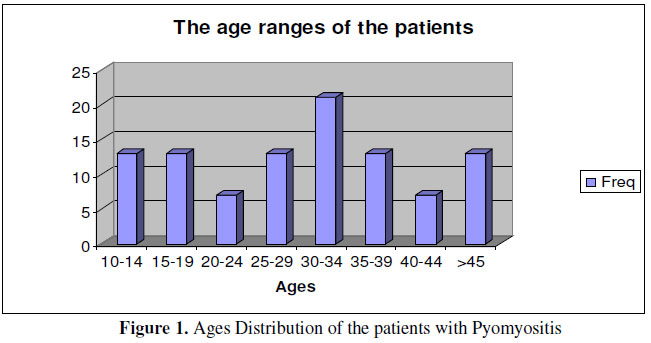
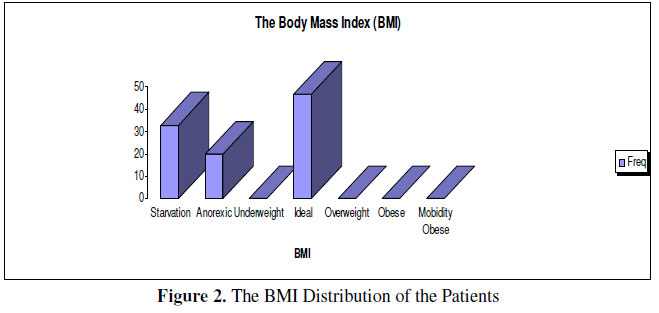
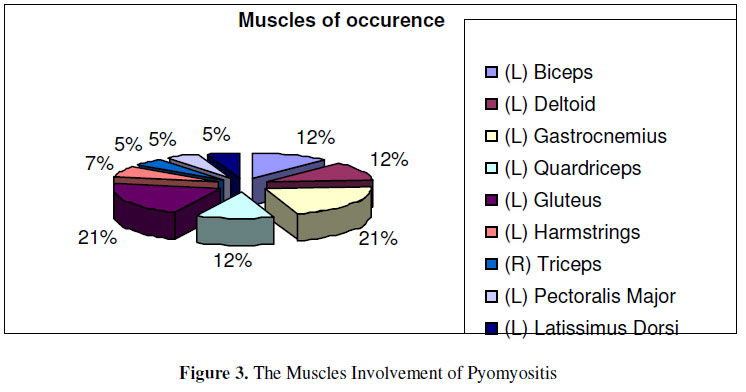
September 2009. Introduction Originally Pyomyositis was restricted to certain well-defined areas1. Large series were reported from Nigeria, Cameroon, Uganda and Solomon Islands and occasional occurrences from countries in Africa, Asia and South America5,19. Between 1960 and 1973, the incidence of up to 10 cases per 10,000 populations was observed in Uganda. In East Africa, the disease concentrated in regions of high altitude, warm and humid climate. In Rwanda and Burundi, Pyomyositis used to be extremely rare, but Rwandan immigrants to Uganda were affected just as often as the local population. In contrast, no cases have been registered among members of the European community in endemic regions5 .With the spread of HIV/AIDS, the pattern of distribution has changed in a dramatic way. In a recent African studies, 63– 80% of patients with Pyomyositis were HIV–positive. The regional incidence of pyomyositis in tropical countries is now closely linked to HIV sero-prevalence, which implicates an extension of disease to previously unaffected areas5,19. The close link between the advanced HIV infection and Pyomyositis suggests that the occurrence of muscle abscesses may be an indicator of stage III HIV disease, according to WHO clinical classification5. Hospital based data show that pyomyositis is relatively rarer in the southern part of Uganda accounting for 4-4.5% of all surgical admissions1,22 compared to the prevalence of 10-15% found in Gulu and the neighboring districts of northern Uganda1,2,3,4,21. The factors leading to its increased occurrence in this region remains unknown. Pyomyositis has been associated with various conditions such as HIV/AIDS5,6, Malnutrition5, Diabetes mellitus7, Alcohol abuse8, and Felty’s syndrome9. There is now considerable epidemiological evidence showing the role of malnutrition and HIV/AIDS in the development of Pyomyositis in Uganda5. It therefore follows that if malnutrition and HIV/AIDS play a major role in the development of Pyomyositis and that the prevalence and incidence of malnutrition and HIV/AIDS is higher in northern Uganda compared to the rest of the country (8.2% and 6.4% respectively)10,11,12. The current upsurge of Pyomyositis in the region follows this defined trend. Patients and Method We conducted a descriptive cross-sectional study from January to September 2009 with pyomyositis patients in Gulu Regional Hospital. This hospital is situated in Laroo division, one of the sub-counties in Gulu Municipality of northern Uganda. This hospital is situated in a region which is just recovering from the 20 year-old civil war. Gulu is strategically located and endowed with its transport terminals and pivoted role in the vast and profitable distribution of goods in the region. It is the regional center for northern Uganda and draws a largely rural population, many people were displaced into camps famously known as the internally displaced peoples camps (IDPS) near the hospital for safety from the insurgency. Patients were selected consecutively from the outpatients department and the casualty unit of the hospital. Informed consent was obtained from each individual patient for the research and each person was free to dissent treatment at any stage of their management without any effect to their follow up treatment. Ethical approval was obtained from ethical review committee and management of the hospital. Overall 100 patients who met the inclusion criteria were included in the study. Non consenting patients and those with secondary pyomyositis were excluded from the study. Data collection The patients were assessed preoperatively, operatively and postoperatively. The demographic characteristics, the physiological status and risk factors investigated. The findings were recorded in a prepared data sheet (questionnaire) designed earlier-on to assess the risk factors and physiological status of the patients. All patients underwent emergency incision & drainage (I & D) procedure. The operative procedures were conducted in the same manner by making a wide incision to ensure that the pus was well drained. The abscess cavity was washed with normal saline and packed with sterile gauze. The patients followed up postoperative until discharge and in the outpatient department in the weekly postoperative surgical review. Data was cleaned and presented in graphs, charts and figures. Results The patients’ ages ranged from 12 to 60 with a mean of 30.3 years. The peak age range was 30-34 years. Fifty three patients (53%) were females and forty seven (47%) males. The male to female (M: F) ratio of 1:1.1. (Figure 1). Figure 2 shows the BMI of the patients. Most (53%)of the patients were malnourished with a BMI less than 17.5; 47 (47%) patients had ideal BMI of greater than 18.5, and none of the patients had a BMI greater than 25. Figure 3 shows the risk factors of Pyomyositis in these patients (Figure 3). Apart from malnutrition, the 0ther risk factors found were HIV/AID (40%) and trauma in 7 (7%) of the patients. All the patients investigated had no other co-morbid condition of Diabetes mellitus and/or hypertension. Figure 3 shows the muscles groups involved. The gluteal, gastrocnemiusand quadriceps were most commonly involved muscles in pyomyositis. Figure 4 shows the distribution of the patients by occupation. The majority (66%) of patients were peasant farmers, 34% were pupils or students. History of previous occurrence of pyomyositis was recorded in a third (33%) of the patients while 67% had first experience. Regarding the Length of symptoms and signs in the patients, all the patients presented late at diagnosis of the disease. The majority (53%) spent weeks before getting correct diagnosis while (47%) took months to have the case diagnosed. Eighty four of the patients who had delayed diagnosis for months were HIV positive. Serology for HIV was positive in 40% of the pyomyositis patients and was negative in 60%. There were no hospital deaths. Discussion The Predisposing factors for Pyomyositis include immunodeficiency, trauma, injection drug use, concurrent infection, and malnutrition. Immunodeficiency has been implicated in the development of Pyomyositis in both temperate and tropical climates13. The common causes of immune deficiency in our environment include; Malnutrition, HIV/AIDS, Diabetes mellitus, malignancy, Liver cirrhosis, renal insufficiency, organ transplantation and administration of immunosuppressive agents13. The age pattern of the study population was specifically consistent with the pattern of the general population of Uganda and particularly northern Uganda which has a young population14. More so previous findings show that Pyomyositis occurs in the young and healthy population13,. The sex distribution of the study population was more or less the reflection of the demographic characteristics of the Uganda in which women constitutes over 51% of the total population of Uganda. But more importantly, most studies show the distribution of 1:1 between males and females13,14,15. The BMI of the patients: Majority (53%) of the patients were malnourished. Recent surveys by UNICEF (2007, 2008, & 2009) indicated that there was a high prevalence of malnutrition in northern Uganda. The most probable reason advanced was inadequate intake of food due to food insufficiency. World Food Program report showed that the populations in the IDP camps were receiving only 60% of the required calories per person per day. This population did not have options of other sources of food since they were in the camps. This could be the reason for the high levels of malnutrition in the region. The HIV status was positive in 40% of the patients and all HIV positive patients were malnourished. The reason for the malnutrition of the HIV patient can be explained in the same way for the general population where there was inadequate food provided by the world food program16. Otherwise, HIV/AIDS also makes the patient lose weight, vomit, diarrhea and other opportunistic infections17. The majority (66%) of the patients were peasant farmers. This is a reflection of a normal demographic characteristic of population in northern Uganda14. Pupils constituted and students constituted a third of the study population. This again is consistent with the fact that Pyomyositis occurs in healthy young individuals5,13. Of all the patients who were malnourished 50% were peasant farmers and 50% pupils. Of all the patients who were HIV positive, 71% were peasant farmers and 29% were pupils and none was a student. HIV infection overloads surgical staff in sub-Saharan Africa as mentioned by many reports on surgical infections/ inflammations: appendicitis in HIV–positive patients23. Forty seven (47%) of the patients were diagnosed after months with the symptoms and signs while fifty three were diagnosed after weeks. The length of symptoms clearly showed how our community responds to their medical problems. But it could also show that patients report early but only delayed to have a proper diagnosis. Most (86%) of the patients who spent months before getting diagnosis were HIV/AIDS positive patients. This is unusual because HIV patients frequent medical institution more often than the rest of the population because of the recurrent opportunistic infections. Early diagnosis is critical for saving the tissue and life of patient but is often missed because of unfamiliarity with the disease, atypical presentations, a wide range of differential diagnoses, and lack of early specific signs18. We noted a high rate of re-interventions, long periods of hospital-stay and high occurrence of surgical site infection in HIV-positive patients in comparison with those HIV negative24. A third (33%) of the patients patients gave a history of previous occurrence of pyomyositis. Out of this only 20% was HIV positive whereas 60% of the patients that had previous history of Pyomyositis were malnourished with a BMI of less than 17.5. In this case therefore the presence of malnutrition was more associated with recurrence5. The muscles involved: The muscles involved in this study were mainly those of the upper and lower limbs. This is consistent with the previous studies conducted elsewhere on Pyomyositis5,19. The lower limb was inolved in 60% of the Pyomyositis and the upper limb in 40%. The majority of the muscle involved was Gluteus maximus, followed by gastrocnemius, Pectoralis major, Deltoid and the rest within other muscles. Muscles frequently involved are quadriceps, glutei, pectoralis major, serratus anterior, biceps, iliopsoas, gastrocnemius, abdominal and spinal muscles5,19,20. This is consistent with previous studies conducted elsewhere in which they reported that Pyomyositis occurred in larger trunk and lower limb muscles5,19. Of special interest to note is that most of the muscles involved were on the left limbs of the patients as opposed to previous studies. Conclusion and Recommendations
Acknowledgement We wish to recognize the enormous contributions of the health workers of Gulu Regional Referral Hospital who supported us during the research work and follow up of the patients. Special appreciation to Gulu hospital administration for the support they offered during the study, the patients for agreeing to be part of the study. References
Copyright 2011 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js11051f1.jpg] [js11051f3.jpg] [js11051f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}