 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 16, No. 3, Nov/Dec, 2011, pp. 64-68 Cold versus hot dissection tonsillectomies: The Nigerian experience A.A. Adoga Department
of Otorhinolaryngology, Faculty of Medical Sciences, University of Jos, PMB
2084, Jos, Plateau state, Nigeria. Code Number: js11052 Background: Tonsillectomy is performed by various techniques but the commonest used in
Nigeria is the cold dissection method. Our study highlights our experience from
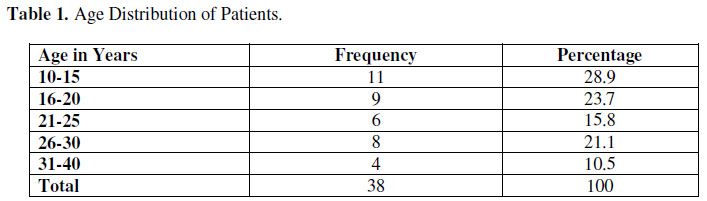
comparing the cold and hot dissection methods of tonsillectomy. Introduction Tonsillectomy is one of the commonest surgical procedures performed worldwide1,2. Various techniques have evolved over the years with the aim of reducing the postoperative morbidity and complications of tonsillectomy. It is generally accepted that the ideal technique should effectively reduce surgery time, intra and postoperative hemorrhage and the morbidity experienced following tonsillectomy3. However, the superiority of one technique over the other has not been clearly demonstrate2, 4. Chronic infections of the tonsils and its systemic repercussions have affected humans for as long as creation. One of the most popular cases is that of the first president of the United States of America, George Washington who died of peritonsillar abscess in 17995. Cornelio Celsus, a Roman aristocrat in the 1st century BC was the first to describe tonsillectomy surgery and its difficulties in the absence of anesthesia. At that time some indications for the removal of tonsils included nocturnal enuresis, convulsions, laryngeal stridor, hoarseness, chronic bronchitis and asthma6,7. Other methods for tonsillectomies arose in the middle ages such as the use of strings tied around the base of tonsils which were tightened daily until the tonsils fell off7. The procedures were abandoned until the 16th century when instruments were fashioned out to perform tonsillectomy. Pare in 1564 and Scultetus in 1655 created the guillotine cutter for uvulotomy. Hildanus in 1646 and Heister in 1763 presented instruments similar to this. These instruments were modified by Physick referred to as the father of American surgery and in 1882, he created the tonsilotome which he used successfully for tonsillectomies6,7. Several others all over the world developed similar instruments which they used with the aim of accomplishing surgery as fast as they could and recording varying success rates6,7. Tonsillectomy which was initially performed by general surgeons became the Otolaryngologists’ care at the end of the 19th century due to the best techniques of illumination which they knew. At the beginning of the 20th century, forceps and scalpels were introduced with reduction in intraoperative hemorrhage. In 1909, tonsillectomy became a safe procedure with the use of ligatures by Cohen to control hemorrhage. The first reported use of carbon dioxide laser for tonsillectomy was in 19738. After these, other methods have been developed such as the powered microdebrider, the harmonic scalpel and most recently coblation all in the aim of increasing the precision of the procedure. The commonest technique of tonsillectomy in Nigeria is the cold dissection tonsillectomy. To the best of my knowledge no report has emanated from this part of the world regarding other forms of tonsillectomy. This study aims to compare operative time, intraoperative hemorrhage and postoperative morbidity such as hemorrhage and pain following cold dissection tonsillectomy and electrodissection using bipolar diathermy. Patients and Methods This was a prospective randomized single-blind study spanning fifty seven months (April 2006 to December 2010). Consent was obtained from all the patients or their parents in the case of minors. Thirty eight patients were drawn from the pool presenting to Victoria Memorial Hospital, Jos, Plateau State, Nigeria with tonsillitis. The inclusion criteria were;
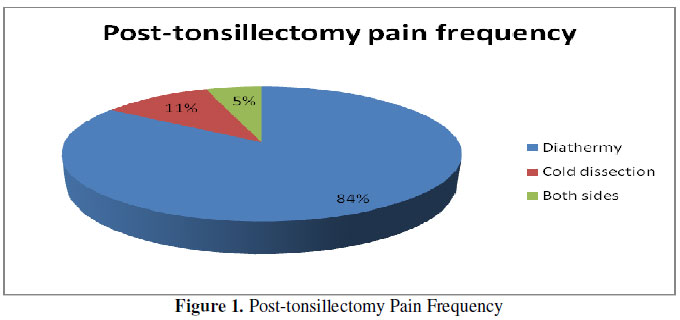
The patients with bleeding disorders, on aspirin and those with unilateral tonsil enlargement were excluded from the study. Preoperatively, patients had routine blood investigations which include Full Blood Count (FBC), Prothrombin/Partial Thromboplastin Time (PT/PTT). Patients were randomized into 2 groups of 19 each. The first group had their right tonsils removed by cold dissection using blunt dissection and the left tonsil by electrodissection using the R. Wolf bipolar generator, model 2351 with probe. The second group had theirs in the reverse order. Patients were not informed of the technique of tonsillectomy used for either side. The method of tonsillectomy was subcapsular. The time taken to remove each tonsil, the intraoperative blood loss, patient reported pain, postoperative hemorrhage and the amount of healing in each tonsil bed on the 7th postoperative days were all recorded. Pain from each tonsil bed was recorded daily by asking the patients to indicate the most painful side from the time they were fully awake from anesthesia. The time taken to remove each tonsil was recorded commencing from the moment a nick was made on the tonsils to the time satisfactory hemostasis was achieved. Estimation of blood loss in this study was subjective. There are other more objective ways of estimating blood loss during surgery and they are by gravimetric, colorimetric, patient weighing and red cell volume studies. Each patient was discharged home on the 2nd postoperative day and given a chart to record the most painful side daily. On the 7th postoperative day, the percentage of remucosalized tonsil bed was recorded. The data collected was analyzed using EPI-INFO database and statistical software for public health professionals version 3.3.2. The results are presented in simple descriptive forms Results A total of 43 tonsillectomies were carried out in the study period of which 38 patients were drafted into the study aged between 10 years and 31 years. There were 21 (55.3%) males and 17 (44.7%) females giving a male to female ratio of 1.2:1. Eleven (28.9%) patients were in the age range 10 to 15 years (Table 1). Removal of tonsils by cold dissection took an average of 11.14 (SD= 9.89) minutes and by diathermy, 9.10 (SD=7.86) minutes. Thirty two (84.2%) patients affirmed that pain was consistently worse on the diathermy side compared with the side on which cold dissection was used right from the day of surgery. Four (10.5%) patients affirmed they felt pain equally on both sides and 2 (5.3%) patients, on the cold dissection side (Figure 1). There was no incidence of postoperative hemorrhage. Examination of the tonsil fossae on the 7th postoperative day revealed more clinically significant eschar on the sides in which diathermy was used with less than 25% healing compared with the sides in which cold blunt dissection was used. Discussion The commonest technique of tonsillectomy in Nigeria is by cold blunt dissection with no records in literature on the use of other techniques from this part of the world. Tonsillectomy like every other surgical procedure is fraught with complications and since various techniques exist in carrying out this procedure, the ideal one will therefore be that in which lesser complications are encountered. However, the technique with the most superiority has not been clinically demonstrated because each technique has advantages and drawbacks. Beginners usually learn the procedure using the cold dissection technique and thereafter, depending on the available facilities and individual preferences, surgeons opt for the technique that best suits them. The complications of tonsillectomy include pain and hemorrhage. Bleeding following tonsillectomy can be severe and life threatening. Many surgeons especially in the developed world use electrocautery for tonsillectomy because it reduces intraoperative hemorrhage thereby reducing dissection time and therefore technically less cumbersome for the surgeon9. However, this technique is fraught with greater postoperative pain both in severity and duration as compared with cold dissection4,9. Our study found that the average time required to remove a tonsil by cold dissection was longer than that for diathermy tonsillectomy. This time difference is statistically significant (P=0.001) but is of little importance in determining the best technique between these two for tonsillectomy. The findings in our study differ from those from other parts of the world. Here it is noted that more intraoperative bleeding was recorded from the sides in which diathermy was used. This is at variance with the findings from studies in other parts of the world in which lesser cases of intraoperative hemorrhages are recorded with diathermy tonsillectomy although the operative times were shorter1, 4,10. Estimation of intraoperative hemorrhage in this study was purely subjective and the use of bipolar diathermy for hemostasis was completely avoided. No incidence of postoperative hemorrhage necessitating re-assessment in the operating room or readmission was recorded in this study. Diathermy technique produces more inadvertent burns and destruction to surrounding tissues blood vessels inclusive, therefore, causing more hemorrhage. The burns and damage to surrounding tissues will also explain the observation in this study of the presence of more eschar on the tonsil beds in which the tonsils were removed by diathermy. These findings compare favorably with those from other studies in which delayed healing of tonsil beds following diathermy tonsillectomy was found to be more significant than in other techniques. Pain is the most significant obstacle to the rehabilitation of patients who have undergone tonsillectomy. This can be in the form of throat pain or referred otalgia. Adequate analgesia is therefore required to ease the agony of pain and to reduce the episodes of hemorrhage because pain increases vascular congestion in the head and neck region which can provoke bleeding13. Assessment of pain at home was unsatisfactory because of lack of its application by the patients and parents and a host of other social factors. This study found that pain was consistently more on the sides following diathermy tonsillectomy conforming to findings in other studies3,14. Increased incidence of pain following diathermy tonsillectomy could be due to excessive thermal damage to the tonsil bed and the experience of the surgeon with the technique. Conclusion In conclusion, diathermy tonsillectomy from this experience has the advantage of shorter operative time but cold dissection tonsillectomy is still more advantageous because it is a safer and more effective method with lesser postoperative morbidity. References
Copyright 2011 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js11052f1.jpg] [js11052t1.jpg] |
| |||||||||

{kind=link}
{kind=link}