 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 16, No. 3, Nov/Dec, 2011, pp. 75-79 Causes and Risk Factors of Non-traumatic Sub-arachnoid Haemorrhage among Patients at Kenyatta National Referral Hospital, Kenya V. Wekesa, N.J.M. Mwang’ombe, C.K. Musau, J.G. Kiboi Neurological Surgery Unit,
Department of Surgery,Kenyatta National Hospital. Code Number: js11054 Background: Subarachnoid Haemorrhage (SAH) has been shown to have a global incidence of
2-49 cases per 100 000 population, and it is associated with a high morbidity
and mortality. There is a scarcity of data regarding this condition in Kenya.
This paper presents the causes and risk factors for this condition in patients
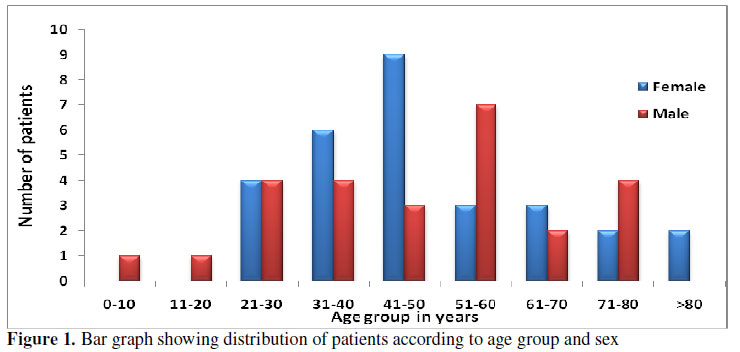
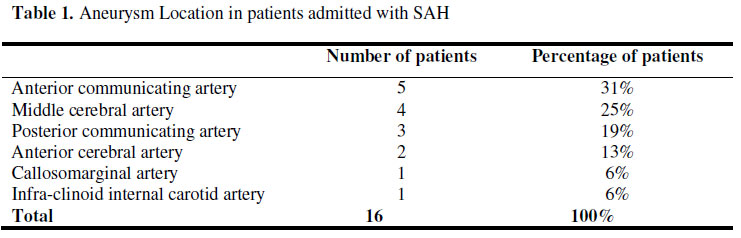
presenting to our hospital. Introduction Subarachnoid hemorrhage (SAH) is the extravasation of blood into the subarachnoid space1. It is a devastating condition with high morbidity and mortality. This disorder is also associated with a significant burden on health care resources, mainly due to hospitalization2,3. It contributes to about 5% of all stroke deaths and to over 25% of potential life years lost through stroke4. Diagnosis to date rests on a high index of suspicion, as this condition can easily be confused with other clinical conditions such as bacterial or viral meningitis. This misdiagnosis will not only delay definitive diagnosis, but it may be fatal due to complications like re-bleeding of ruptured aneurysms or vasospasm. There is a scarcity of data regarding subarachnoid haemorrhage in Kenya. This paper presents the causes and risk factors for this condition among patients presenting in our hospital. Methods This descriptive cross sectional study was conducted at Kenyatta National Hospital between December 2010 and March 2011. This is a national teaching and referral hospital in Nairobi Kenya, with fully established departments for various specialties including neurosurgery and neurology, under the departments of surgery and medicine respectively. Patients admitted with confirmed diagnosis of non traumatic SAH, and had given a written informed consent were included in the study. Data on causes, pattern, and socio-demographic characteristics was collected using a questionnaire administered to patients who met the inclusion criteria. Data collected was entered and analyzed using Statistical Package for Social Sciences (SPSS) for Windows® version 16.0. Approval for the study was granted by University of Nairobi/ Kenyatta National Hospital Research and Ethics Committee. Results A total of 55 patients who met the inclusion criteria consented and were recruited into the study. There were 26 (47%) male patients and 29 (53%) female patients giving a male to female ratio of 1:1.12. The mean age for the patients was 47.5± 18.3 years and a median age of 45 years. The male group had a mean age of 46.3 years while female group had mean age of 49.3 years. The extremes of ages formed the least group of patients in this study with most patients (75%) falling between 21 and 60 years of age (Figure 1). Causes of SAH Intracranial aneurysms were seen in 29% of patients in this study. The commonest area of occurrence of these aneurysms was the anterior communicating artery (31%). The middle cerebral and posterior communicating artery aneurysms represented 25% and 19% respectively, (p=0.416). Other vessels in which aneurysms occurred are shown in Table 1. The other causes of SAH were Arterio-Venous Malformation in 4% of cases, (p=0.010), and Tumor in 2% of the cases. Risk factors for SAH Most patients (51%) presenting with SAH had poorly controlled hypertension, of these 60% had elevated blood pressure at the diagnosis of SAH. Other risk factors included alcohol intake (31%), cigarette smoking (15%) (P=0.117). Amongst female study subjects, use of hormonal contraceptives was reported in 22%. When asked whether there was a history of SAH in the family, 7% of the patients responded positively while the rest (93%) did not have a family history of the condition Discussion Subarachnoid hemorrhage (SAH) is associated with high morbidity and mortality. In a virtual study in which Computed Tomography (CT) scanning was applied to all patients, the incidence was calculated to have been 5.6 per 100,000 patient years5. In a meta-analysis of relevant studies, the global incidence rate was 10.5 per 100,000 person years5. Women have a 1.6 times {95% Confidence interval (CI 1.5-2.3) higher risk than men5, while blacks have a 2.1 times (95% CI 1.3-3.6) higher risk than whites of suffering from SAH6. Ebrahimi et al7. however found no significant difference between male and female involvement. The incidence of the disorder increases with age and peaks in the 6th decade8,9. Landtblom et al10, found the median age of presentation to have been 58 years, while Martinez- Manas et al.11, found the mean age of SAH to have been 53.67 (16-88) years. Ruptured aneurysms are the commonest causes of spontaneous SAH3. In this study, aneurysmal SAH was noted in 29% of patients but could not be confirmed in 25% of cases. Anterior communicating artery aneurysms were the commonest, accounting for 31% of all the aneurysms, followed by the middle cerebral artery aneurysms (25%). No aneurysm was however noted in the posterior circulation by the time the study was concluded. This contrasts to a study by Nrupen et al.13 in which aneurysmal SAH accounted for 70.4% of cases of SAH in his series. The anterior communicating artery aneurysm was the commonest in Nrupen’s series accounting for 25.8% of cases, followed by ICA and MCA respectively at 24.5% and 21% respectively. AVMs accounted for 1.5% of SAH in the same study of Nrupen et al. This contrasts to the findings of this current study where we noted AVMs to account for 4% of cases with SAH. A study by Gao Yongzhong27 reported the incidence of SAH in brain tumors as 2.3%, which compared closely to the findings in this study of 2%. Risk factors of SAH are divided into modifiable and non-modifiable factors. Familial predisposition is an important non-modifiable risk factor. A number of studies have reported a positive family history in 5% -20% of SAH cases12. This compares closely to findings in this study where a positive family history was seen in 7% of patients with SAH. First degree relatives of patients with SAH have a 3 to 7- fold increased risk of suffering from SAH14-18. The incidence in the second degree relatives is similar to that in the general population14. Autosomal dominant polycystic kidney disease (ADPKD) is an important heritable clinical condition associated with SAH. It is found in 2% of all patients with SAH19. Other heritable conditions include fibromuscular dysplasia and pseudoxanthoma elasticum20. Modifiable risk factors for SAH include smoking, hypertension and heavy drinking21. Cocaine use has been associated with SAH, and there is always an underlying aneurysm22. In the present study, patients who had SAH and were cigarette smokers accounted for 15% of cases, those taking alcohol accounted for 31% of cases, while contraceptive use was observed in 22% of female patients. Fifty one percent (51%) of patients were known hypertensives prior to the SAH episode, while 60% of patients had elevated blood pressure at the diagnosis of SAH. Sankai T et al.23 noted that heavy drinking among men was an independent risk factor for SAH with a relative risk of 4.3 (95% CI). No added risk was however, found for women. The use of oral contraceptives has been shown to have significant risk for SAH24. The risk of rupture depends on the size and location of the aneurysm25. According to the international study of un-ruptured intra-cranial aneurysms in patients with no history of SAH25, the five-year cumulative rate of rupture of aneurysms located in the internal carotid artery, anterior communicating artery, anterior cerebral artery or middle cerebral artery is zero for aneurysms less than 7mm, 2.6% for 7-12mm, 14.5% for 13-24mm, and 40% for 25mm or more. This contrasts with a rupture rate of 2.5%, 14.5%, 18.4% and 50% respectively, for the same sizes of aneurysms in the posterior circulation and posterior communicating artery. Conclusion
References
Copyright 2011 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js11054f1.jpg] [js11054t1.jpg] |
| |||||||||

{kind=link}
{kind=link}