 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 16, No. 3, Nov/Dec, 2011, pp. 80-84 Pattern of Lower Third Impaction and Outcome of Treatment in a New Tertiary Center - A 5-year Survey B.O. Akinbami, L.I. Ifomala Department of Oral and
maxillofacial surgery, University of Port Harcourt Teaching Hospital, Port
Harcourt, Nigeria. Code Number: js11055 Background: Third
molar surgery is the commonest dentoalveolar surgery in clinical practice and
outcome is dependent on the assessment of the nature of impaction, meticulous
care and adherence to instructions. The purpose of this study was to document
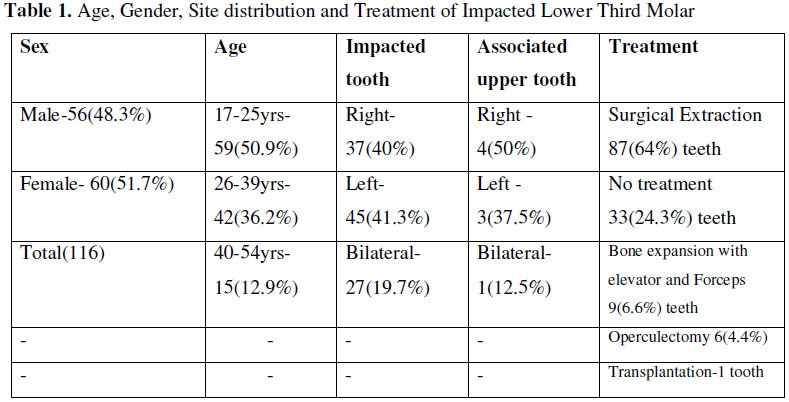
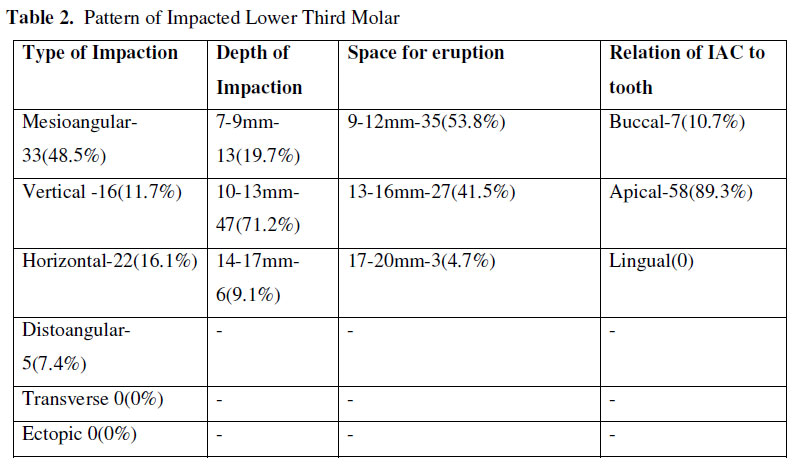
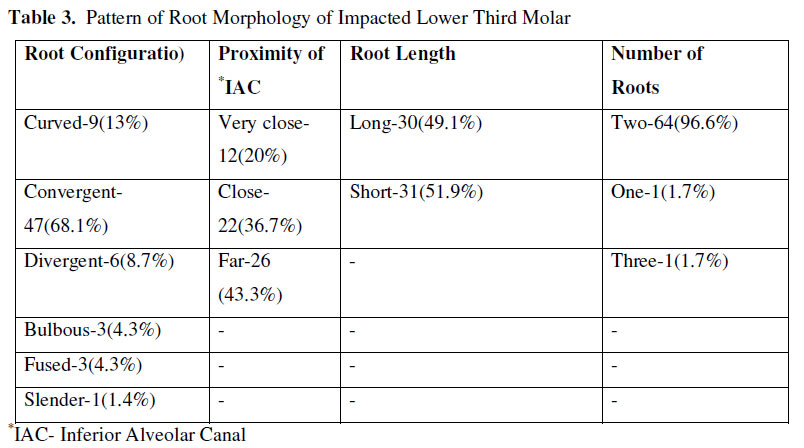
our five –year experience. Introduction Impaction of lower third molar is the commonest reason for dentoalveolar surgery during and after adolescence. The tooth is the last to form and erupt in the dentition at about the age of 4-6 and 16-23 years respectively1. Angulation, position, configuration of the roots, proximity of the inferior alveolar neurovascular bundle, density of surrounding alveolar bone and most importantly the depth of the impacted tooth are factors relevant to the difficulty that will be experienced in the extraction of the tooth and these invariably also determine the type of extraction whether surgical, only forceps or combined forceps/elevator extraction3.Techniques of surgical extraction are also based on thorough clinical and radiological assessment described by Pederson as well as available facilities3,4. Impactions with low difficulty index (0-3) and soft tissue impactions are readily treated by forceps extraction alone4.However, it is not all impacted third molars that must be extracted. The complication of lower third molar surgery that has generated much concern and even litigation issues has to do with injury to the inferior alveolar and lingual nerves. However with the improvement in contrast CT imaging, helical CT, MRI, as well as the 3D cone beam CT machines which reduce exposure to irradiations, there is better assessment of the proximity of the inferior alveolar canal to the tooth5. Coronectomy mostly without root canal therapy is the latest form of treatment applicable in the treatment of impacted third molar to avoid injury to the inferior alveolar neurovascular bundle6,7 Various articles on diverse topics related to lower third molar impaction abound in the medical literature, notwithstanding the oral and maxillofacial surgical department of the University of Port Harcourt Teaching Hospital, Port Harcourt. Nigeria, is a new tertiary center and our aim was to document the 5-years’ survey of the pattern and treatment outcome of lower third molar impaction. Patients and Methods The study was a retrospective and descriptive analysis of the consecutive patients that attended the Oral and maxillofacial surgery department of University of Port Harcourt Teaching Hospital, Port Harcourt between May 2006 and April 2011. Approval to carry out the study was given by the hospital’s ethics and research committee. Case files were obtained from the Dental center record’s department. Included in the study were all cases of unilateral or bilateral lower third molar impaction with or without upper third molar impaction that had presented to the clinic during the 5 year period. Intraoral periapical views were used to assess the parameters. Clinico-radiological information retrieved included patients’ biodata, number of impaction, associated pathologies like pericoronitis, cysts or tumors and associated upper molar impaction. Others are type/angulation, position and depth of the teeth, number and configuration of the roots, proximity of the inferior alveolar canal, method of extraction and outcome of extraction. Type/angulation of impaction was classified as mesioangular, vertical, horizontal, distal, transverse and ectopic. Position of impaction was classified as I, II and III depending on the amount of space available between the second molar and ramus. The depth of impaction was categorized as A,B and C depending on the distance (Winter’s line) between the summit of the impacted tooth to a line drawn along the alveolar crest (Amber line) or to a line drawn along the occlusal surface of the remaining teeth (White line). Configuration of the roots were either convergent, divergent, fused, curved, straight, bulbous, slender, short or long. Proximity of inferior alveolar canal was simply apical or buccal and the apical relationship further classified as far, near, very close. Number of cases that were treated by each method of extraction, time taken to extract as well as the complications were documented. A case of transplantation of the third molar into the socket of the second molar extracted due to resorption of the root from pressure of the impacted third molar was also highlighted. Extractions were done either by the specialist or the resident in training. Data was entered into the computer and statistical analysis was done using the SPSS version 10 software packages (Illinois, Chicago). Results were expressed in simple frequencies and proportions. Results There were 116 patients with a total of 136 impacted lower third molar and 9 impacted upper third molar that presented to the hospital within the study period. Complete data information was retrieved in 56 (48.3%) patients. Fifty six (48.3%) patients of the one hundred and sixteen, were males and 60 (51.7%) were females. Age range was 17-54years; Mean (SD), 28.2(8.2). Mesioangular impaction constituted the majority, 66(48.5%) while distoangular was the lowest 10(7.4%) (Table 1). The distance between the distal surface and retromolar pad (space for eruption) ranged between 9-20mm. None of the teeth was completely buried in the ramus. The depth of impaction ranged between 7 and 16mm (Table 2). The impacted teeth that had two roots were 64, those with one or three roots were 1 respectively. The roots were long in 30 cases and short in 31 cases. There were 7 teeth with curved roots, 47 were convergent, 6 were divergent, 3 were bulbous, 3 were fused (Table 3). The impacted teeth showed a buccal relationship to inferior alveolar canal in 7 cases and apical in 58 cases. In those with apical relationship, the apices of the roots were very close to the inferior alveolar canal in 10 cases, they were close in 22 cases and far from the canal in 26 cases.Thirty three (24.3%) impacted teeth did not undergo any surgical treatment. Extraction of 9(6.6%) teeth was done using elevators and forceps, surgical extraction of 87(64%) teeth was done using the buccal guttering technique, and operculectomy was done around 6(4.4%) teeth. Deeply buried teeth and those with divergent roots or severely curved roots were more difficult and took more than 45 minutes to extract. Transplantation of extracted impacted lower third molar tooth into the socket of a second molar tooth was achieved in one of the patients. The second molar tooth was extracted due to pain from the pressure resorption of the third molar. Other associated preoperative sequelae were acute and recurrent pericoronitis found in about one third of the patients. There were no cases of dentigerous cysts or unicystic ameloblastomas. There were only 2(1.9%) patients that presented with neuropraxia following surgical extraction. This however improved within 6 weeks with neurovitamins. There were 5 (4.9%) patients with dry socket and 3(2.9%) patients with excessive swelling. There were no fractures of the jaw or adjacent tooth even in the cases that had bilateral or multiple extractions same day. There was satisfactory incorporation of the transplanted tooth 3 weeks following treatment without any evidence of mobility and infection with a follow-up of six months. Discussion In our study mesioangular impacted lower third molar was the most common form of impaction in line with other studies1,3,8.However, our study showed horizontally impacted lower third molar to be more common than vertical and distoangular impacted lower third molar which is contrary to findings in other studies. The gender and age distribution seen in our study as well as location of unilateral impaction were comparable with other reports3,8. The space available for the lower third molar tooth is a significant factor that influences impaction of the tooth, and this is largely determined by the functional growth of the mandible and alveolar arch, as well as sizes of the earlier erupted teeth2,4. The average size of a lower third molar is about 15mm and a retromolar space of about 4mm must still be available to minimize the occurrence of impaction. More than 90% of our cases had less than 17mm available space for the teeth to erupt. This phenomenon has been adduced to the increasing refined nature of diet and inheritance4. Impacted third molar teeth can be completely buried in the jawbone. In such cases, it is a bony impaction. If the wisdom tooth has erupted out of the jawbone or even through the gum, it is a soft tissue impaction. This effect is closely related to the depth of impaction and height of the body of the mandible. Completely buried tooth in a high body of the mandible will have a high vertical (winter’s) line with a greater difficulty in extraction and possible complications3,9,10.Cases with high winter’s line in our study constituted 9.1% with increased time to extract and more post-operative swelling. Cases with divergent, excessively curved roots and slender roots gave some difficulties during extraction as well with resultant fracture in one of the roots or apical portion. There were no cases of perforation of the roots or bridging of the inferior alveolar canal in our study, this is usually signified by discontinuity in the upper and lower radio-opaque lamina of canal7,10,11.Cases of inferior alveolar neurovascular bundle perforating through the two converging roots of some impacted molars have been reported with greater risk of damage to the nerve and bleeding, 8-13 patients should be well informed of the possibilities of post operative sensory loss on the lip which may last for variable period of time. However, meticulous root division and/ or coronectomy is useful to avert such problems6,7 . In a small portion of patients, cysts and tumors occur around impacted wisdom teeth, requiring surgical extraction but none was found in our study. Estimates of the incidence of cysts around impacted teeth vary from 0.001% to 11%, with a higher incidence in older patients, suggesting that the chance of a cyst or tumor increases the longer an impaction exists.Only 1-2% of impactions resulted in malignant tumors15. Pressure resorption of the second molar constitute the highest preoperative sequelae experienced with third molar impaction,though there were two cases seen in this report4. Proponents of prophylactic extraction of impacted tooth based their argument on the fact that leaving the tooth has the risk of developing the above mentioned pathologies, harbouring some organisms that can cause congenital diseases, and also that the wisdom tooth has little function in the dentition15. But opponents have argued that such risks are minimal and that presence of impaction minimizes risk of condylar fractures by allowing forces to concentrate on the angle, therefore not every patient should be subjected to the trauma of extraction based on mere speculation or expectation of a sequelae, however a joint committee on third molar management has emphasized the presence of cyst, tumor, resorption of adjacent tooth, caries, recurrent pericoronitis(not single episode), orthodontic, and prosthodontic problems associated with the tooth as indications for extraction14,17.In our study, none of these effects was found in 33 patients and the teeth were not treated. This study also reported the possibility of transplanting the third molar into the socket of second molar, the first case was successful but the second case we attempted did not work because the socket of the second molar was smaller than the size of the third molar. Typically mesioangular impactions are the most difficult to extract in the maxilla and easiest to extract in the mandible, while distoangular impactions are the easiest to extract in the maxilla and most difficult to extract in the mandible8. Our study gave similar experience, although we had few cases of associated upper third molar. Horizontal and distoangular impactions will most times require tooth division to allow the root to be moved into and out of the socket with elevators10. It is certain that difficulty index of extraction is dependent on the type of impaction, depth of impaction, density of bone, morphology of roots but the assessment of this index does not have to be based or determined only on the time taken to do the extraction because the skill and experience of the surgeon, facilities available, pain threshold and mode of anaesthesia play a significant role3,19,20 .For instance, a deeply buried horizontally impacted lower third with divergent roots partly in the ramus extracted surgically under general anaesthesia or even local anaesthesia in a highly co-operative patient may not take more than 45 minutes in the hands of skilled surgeon while a well spaced mesioangular or vertically impacted tooth with crown almost at the level of the occlusal line, convergent root not encasing neurovascular bundle but within a dense bone may take as much time or more in the hand of the same surgeon if dealing with an uncooperative patient under local anaesthesia. However, less than 10% percent of the extractions we did lasted more than 45 minutes. Also, complications has a lot to do with strictly abiding by the principles of surgery especially irrigation and avoidance of neurovascular bundle, and thorough preoperative evaluation and surgeon’s skill are important8-16,19-23. These incidence of complications in our study were lower than those obtained from other studies.9-12 Conclusion Deeply buried teeth and divergent roots were more prone to fracture and difficult to extract. In other to ensure a smooth postoperative recovery for the patient, thorough radiologic evaluation of the third molar and contiguous structures to determine the challenges that must be surmounted to achieve acceptable outcome is vital. Transplantation must be considered when the second molar is damaged by resorption or caries to avoid loss of two teeth. References
Copyright 2011 - East and Central African Journal of Surgery The following images related to this document are available:Photo images[js11055t1.jpg] [js11055t3.jpg] [js11055t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}